

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Symptomatic epilepsy is defined as epilepsy having gross anatomic or pathologic abnormalities secondary to anacquired or genetic cause (1). Its natural course and response to medical treatment are determined by its etiology. Approximately 25% of symptomatic epilepsy cases are refractory (2). In such cases, accurate localization of the epileptogenic zone (EZ) is one of the strongest prognostic factors since it allows complete surgical resection and effective seizure control (3). Currently, localization is achieved by a combination of seizure semiology and electroencephalography (EEG) along with structural magnetic resonance imaging (sMRI). In cases with negative sMRI or discordant findings, interictal 18-flurodeoxyglucose positron emission tomography (PET) and ictal single-photon emission computed tomography (SPECT) can be used for localization. However, these modalities involve ionizing radiation with limited resolution. Although invasive EEG is highly accurate, it has a limited sampling area (4). A more circumscribed localization with non-invasive imaging can help guide the placement of these electrodes (5).
Arterial spin labelling (ASL)-based magnetic resonance (MR) perfusion is a technique that has potential to be used as a non-invasive and non-irradiating supplementary method of localization. In this article, we review clinical insights and advantages gained from its use in the evaluation of epilepsy.
Principles of ASL
Arterial spin labelling uses an inversion pulse to tag flowing blood in the neck. Following a short post-labelling delay (PLD) to allow for intracranial transit, these ‘labelled’ spins are imaged during exchange into the brain parenchyma. Subtracting a paired set of ‘labelled’ and unlabelled ‘control’ images will yield parametric maps of absolute cerebral blood flow (CBF) that may be used for qualitative and quantitative evaluation. In effect, ASL uses blood as an endogenous contrast material, making it non-invasive and repeatable. Thus, it has significant advantages, particularly for pediatric population (6).
Scans are performed on a 3T GE Discovery 750w scanner (GE Healthcare, Milwaukee, USA) using a three dimensional-pseudocontinuous ASL sequenceprior to contrast administration per recommendations by the International Society for Magnetic Resonance in Medicine (5). Post-processing includes CBF quantification and fusion with relevant sMRI sequences.
Basis of ASL in Epilepsy Imaging
Two important concepts are necessary to understand the aim and utility of ASL in epilepsy: the EZ and the principle of neurovascular coupling.
The Epileptogenic Zone
The part of the cortex from which seizures originate is referred to as the ictal onset zone (IOZ). Some lesions such as arteriovenous malformations (AVMs) and tumors have a perilesional EZ that does not necessarily overlap with the IOZ. It is capable of generating seizures by itself even after removing the inciting lesion. Spread of epileptic activity to adjacent areas will manifest as semiology of the seizure. This is designated as the symptomatogenic zone. A functional deficit zone (FDZ) corresponds to areas with altered interictal function while the irritative zone generates interictal spikes that are secondary to inhibitory neural networks (Fig. 1). EZ represents the minimum amount of tissue that must be surgically resected or disconnected. Its accurate delineation is the holy grail of presurgical evaluation since it impacts post-operative seizure freedom and neurocognitive outcomes (5789). Evidence has emerged that FDZ identified by neuropsychological evaluation or regions of PET hypometabolism may expand horizons of EZ, particularly in temporal lobe epilepsy (TLE), thus requiring additional resection (91011). EZ is thus a theoretical construct that can only be estimated based on combined evidence from seizure semiology, electrophysiological tests, and imaging. Alterations in perfusion as reflected on ASL may occur not only in EZ, but also in FDZ and symptomatogenic zones. ASL has a reasonable overall accuracy of 70% in localizing the seizure focus, which is lower than the overall accuracy of 95% by electroclinical localization (12). Thus, interpretation of ASL in isolation is limited. Electroclinical evidence must be considered to reach a more accurate estimation of EZ location.
Neurovascular Coupling
Neurovascular coupling is the phenomenon that links transient neural activity to a corresponding increase in regional CBF. This is an active process. It is not merely dependent on an oxygen debt as previously thought. Changes in neuronal activity can modulate vascular smooth muscle tone via neuronal synaptic activity and glial release of vasoactive mediators occurring at the level of neurovascular unit (13). Although highly controversial, neurovascular coupling has been shown to be largely intact within the EZ (141516). This forms the basis of perfusion techniques such as ASL and SPECT in detecting alterations of blood flow related to abnormal synaptic activity. Most epileptogenic foci are hypoperfused during the interictal period and become hyperperfused during seizures. This indirect information must always be correlated for concordance with the original electroclinical hypothesis since this may encompass the IOZ and potentially FDZ (17).
Positron emission tomography has been found to have higher level of concordance with electroclinical localization in mesial TLE (MTLE) (78%) than that in extratemporal epilepsy (28.6%) (18). Data from SPECT studies have shown that this sensitivity is increased when patient is additionally imaged in the peri-ictal period compared to in the interictal period alone (19). Hence, a significant advantage of ASL over PET is that it can show both peri-ictal and interictal abnormalities. This implies that, for a useful evaluation of ASL, it is imperative to know if the patient is imaged in the peri-ictal or interictal period based on clinical history or EEG findings and compare focal abnormalities on ASL to seizure semiology and expected hemodynamics of the lesion.
Application of ASL in Symptomatic Localization Related Epilepsy
We will describe the utility of ASL in the evaluation of five basic substrates for epilepsy: 1) mesial temporal sclerosis, 2) malformations of cortical development (MCDs), 3) neoplasms, 4) vascular malformations, and 5) infections, inflammations, and gliosis. In addition, we will describe the application of ASL in sMRI-negative epilepsy. Where studies on ASL specific to the entity are lacking, we will describe comparable modalities such as PET and dynamic susceptibility contrast (DSC) imaging.
Mesial Temporal Lobe Epilepsy
Hippocampal sclerosis is the most common cause of intractable epilepsy (2). Approximately 20–30% of patients with MTLE have no sMRI identifiable abnormality (20). While visual inspection of ASL CBF maps may identify obvious areas of altered perfusion (Fig. 2), quantitative methods are needed for cases with ambiguous lateralization. Mean CBF values derived by regions of interest over the right (R) and left (L) mesial temporal regions may be used to calculate Asymmetry Index (AI) using the following formula: AI = 100 × (L − R) / (R − L), with negative values indicating left lateralization (21). However, caution is needed since normal subjects may show physiological left temporal lobe hyperperfusion. Seizure frequency and severity inversely are correlated with ipsilateral hippocampal CBF, but not with the magnitude of AI possibly due to secondary involvement of contralateral temporal lobe (2223). Since these changes occur in sMRI-negative cases as well, ASL can improve the overall sensitivity of MRI. It has shown a good concordance with both PET and electrical source imaging (242526). Another important caveat is peri-ictal hippocampal changes in conditions such as status epilepticus that may occur regardless of the site of ictal onset. Interval imaging may be necessary to look for reversibility or evolution into sclerosis (2728).
Malformations of Cortical Development
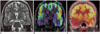
Malformations of cortical development comprise between 10–50% of pediatric and 4–25% of adult surgical epilepsy patients (29). Focal cortical dysplasias (FCDs) are probably the most common cause of intractable extratemporal epilepsy (30). On nuclear imaging, FCDs commonly show interictal hypometabolism and peri-ictal hypermetabolism. These areas typically appear larger than sMRI-visible lesion (Fig. 3) (31). While this has conventionally been attributed to altered synaptic/epileptic activity, Wintermark et al. (32) have suggested that these findings might be related to higher microvessel density measured by immunohistochemical staining of CD34 positive endothelial cells on surgical resection specimens. They also found significantly higher vascular density in the adjacent normal appearing cortex and hypothesized that interictally hypervascular FCDs might require larger resection margin (32). ASL is also a viable substitute for nuclear imaging to localize the offending tuber in tuberous sclerosis (33).
Hemimegalencephaly is a prime example of pathology in which perfusion and metabolism may be uncoupled. Involved areas may show variable metabolic activities on PET with a paradoxically opposite perfusion pattern on SPECT that suggests a role of either vascular proliferative abnormalities or subclinical seizures (34). ASL has shown similar variability in perfusion of these lesions (Fig. 4) (3536).
Polymicrogyric cortex shows variable patterns of metabolic activity compared to normal cortex on PET (37). Band heterotopia may show similar or higher metabolic activity compared to overlying cortex appearing as a ‘double cortex’ similar to structural imaging. In both these entities, altered perfusion might be related to synaptic activity of neurons regardless of whether it results in clinical seizures (3839). ASL shows perfusion patterns concordant with PET (Fig. 5). ASL also allows ruling out of contralateral perfusion anomalies related to microstructural or network alterations since these anomalies could potentially impact post-surgical outcomes (3140).
Neoplasms
Tumors associated with drug resistant epilepsy for a duration of usually two years or longer are termed long-term epilepsy associated tumors, with gangliogliomas and dysembryoplastic neuroepithelial tumors being the commonest (41). Early resection is preferred for both seizure control and tumor remission (42). The utility of ASL in predicting tumor grade has been well established (43). However, when the primary goal of surgery is seizure control, EZ, not just the tumor, should be resected. It has been shown that EEG and ictal SPECT are useful in delineating EZ around tumors (44). Peri-ictal ASL has similar potential. It may reduce the need for a separate study. Alterations of perfusion may also represent ictal activity propagation to a symptomatogenic zone (Fig. 6).
Vascular Malformations
Seizures in vascular malformations are caused by neuronal toxicity and gliosis secondary to hemosiderin deposition during overt or subclinical hemorrhage. Chronic venous congestion, impaired peri-nidal cerebrovascular reserve, and steal phenomena are additional factors in the epileptogenicity of AVMs (45).
Arterial spin labelling allows characterization of both vascular malformation and its secondary effects on the brain parenchyma. Venous signal on ASL is a sensitive marker of shunting in occult malformations (46). Using a single compartment model, semi-quantitiative estimation of shunt fraction can be calculated. Multi-PLD ASL allows estimation of transit times. It is useful for monitoring patients after shunt reduction interventions or radiosurgery (47). Peri-nidal hyperperfusion and steal phenomena can also be identified and quantified (Fig. 7). Areas of peri-ictal hyperperfusion distant from the AVM nidus have been found to be consistent with secondary EZs (48).
Epileptogenic cavernomas may demonstrate peri-ictal hyperperfusion of the adjacent cortex (49). Developmental venous anomalies may also be associated with epilepsy, even when they are isolated (50). Although variable peri-lesional parenchymal perfusion changes may be seen, hyperperfusion must be interpreted with caution since it might be related to micro-shunting within the parenchymal microvasculature, not necessarily a peri-ictal change (51). In Sturge-Weber syndrome, DSC perfusion studies have demonstrated that white matter perfusion is increased in early stages with progressive hypoperfusion with increasing severity and duration of epilepsy (52).
Infections, Inflammations and Gliosis
Inflammatory Epilepsies
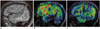
Rasmussen's syndrome is the prototypical T-cell mediated pediatric immune disorder characterized by refractory focal seizures and development of progressive unilateral neurological deficits (53). PET and ASL imaging have shown areas of hypermetabolism/perfusion consistent with ictal activity on EEG. However, dissociated area of hyperperfusion might be related to ongoing inflammation. It can be used as a marker of disease activity (Fig. 8) (5455).
Other humorally-mediated autoimmune epilepsies clinically present with a syndrome of subacute limbic or neocortical encephalitis (56) characterized by variable limbic or extralimbic sMRI abnormalities (57). ASL may show peri-ictal hyperperfusion. However, changes related to inflammation may precede sMRI findings. They can be used to monitor response to therapy (5859).
Infective Epilepsies
Seizures can occur during the acute phase of infection or as its sequelae. Epileptogenicity is multifactorial and dependent on pathogen virulence, lesion type, degree of cortical involvement, and host inflammatory response (60). In herpes simplex encephalitis, ASL shows hyperperfusion consistent with inflammation which may help differentiate other hypoperfused lesions such as diffuse astrocytomas. In meningitis, gyral hyperperfusion,and less commonly, hypoperfusion, may be seen (Fig. 9). Abscesses show low perfusion along their rims, differentiating them from necrotic glioblastomas (61). Whole-brain CBF has been found to be reduced in human immunodeficiency virus-related encephalopathy. However, in progressive multifocal leukoencephalopathy, hyperperfusion is associated with disease progression and inversely related to the incidence of immune reconstitution inflammatory syndrome (6263). Thus, ASL can lead to better characterization of pathogen-host relationship. It might be used to non-invasively monitor response to therapy.
Gliosis-Related Epilepsies
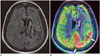
Gliosis is identified by non-specific neuronal loss and reactive astrogliosis. The most common causes encountered in epilepsy are those secondary to perinatal insults, infarctions, trauma, and demyelination (29). Surgical outcomes are inferior in this subgroup as pathologies are poorly circumscribed, often involving eloquent cortex that constrains complete resections (64). Most encephalomalacic lesions are characterized by interictal hypoperfusion on ASL (65). Hypoperfusion extending beyond the electroclinical EZ or sMRI abnormal areas can adversely impact outcomes. Peri-ictal hyperperfusion of the overlying cortex in post-stroke seizures and in Wilson's disease (Fig. 10) has also been reported (666768).
Structural MRI-Negative Epilepsy
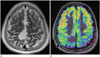
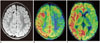
An estimated 20–40% of surgical epilepsy patients have no identifiable causative lesion on sMRI. This adversely affects prognosis and presents difficulties for surgical resection (69). The most common underlying pathologies identified are FCDs, gliosis, hamartomas, and hippocampal sclerosis, with the rest being negative for any histopathological abnormality (7071). Invasive EEG monitoring before surgical resection can be aided by prior non-invasive lateralization or localization. PET has shown a high concordance of lateralization with intracranial EEG (44.3–100%), but a more variable localization value (11–69% concordance) (72). PET positivity itself is a good prognosticator for post-surgical outcomes (20). ASL has shown excellent and high concordances with PET in lateralization and localization of EZ. It is a promising utility in the evaluation of MR-negative epilepsies (Fig. 11) (73).
Imaging in Acute Settings
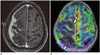
Failure to terminate seizures can lead to permanent neurological damage termed status epilepticus (or epilepsia partialis continua for partial seizures). A less easily recognized ‘non-convulsive’ status may also occur (74). sMRI may disclose a range of findings, including gyral swelling and secondary hippocampal or thalamic involvement with variable diffusion restriction, persistence of which indicates poorer outcomes. ASL demonstrates focal or diffuse hyperemia with high sensitivity and concordance with EEG (49). Distribution of abnormalities may encompass the EZ as well as areas of seizure propagation (Fig. 12) (4968). ASL also allows serial follow-up and prognostication (7475).
CONCLUSION
Accurate identification of the EZ is crucial in presurgical evaluation of epilepsy since it influences prognosis. ASL is a non-contrast MR perfusion technique that demonstrates alterations in perfusion related to abnormal synaptic activity, akin to nuclear imaging. This not only allows localization of the epileptogenic focus, but also provides functional characterization of abnormalities identified by sMRI. ASL is a useful supplementary investigation. It has potential to make MRI a one-stop-shop in epilepsy evaluation.






 XML Download
XML Download