

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Claudins are structural molecules of tight junctions (TJs).1 Twenty-seven claudins are known, and their expression is responsible for changes in the electrolyte and solute permeability of cell layers.2 Claudins 1, 3, 4, 5, 7, 8 and 18 are expressed in human bronchi and bronchioles.34 An integral membrane protein, claudin-5 (CLDN5), is mainly expressed by the vascular endothelium, including in the pulmonary microcirculation, and is a critical component of endothelial TJs that control pericellular permeability.5 CLDN5, albeit expressed weakly in the epithelium, is expressed strongly in the endothelium of normal lung and intensely in the endothelium of lungs with interstitial pneumonia.4
Lung CLDN5 expression tends to be inversely correlated with the severity of lung injury. CLDN5 expression was more increased in injury-resistant mouse strains compared with injury-sensitive mouse strains subjected to acrolein-induced acute lung injury.6 CLDN5 was down-regulated in lung tissue in human immunodeficiency virus type 1 (HIV-1)-infected patients with interstitial pneumonitis.7 The plasma CLDN5 levels were lower in patients with stable asthma compared with in control subjects and higher in those with exacerbation compared with in those with stable asthma.8910
Chronic obstructive pulmonary disease (COPD) is characterized by a progressive deterioration of lung function. In many patients, the disease course is punctuated by exacerbations, an acute worsening of symptoms that, in severe cases, can necessitate hospitalization and even result in death.1112 Exacerbations are the major cost driver, directly and indirectly, in COPD.13 COPD exacerbations cluster in time and patients who have experienced 1 episode are at increased risk of further exacerbations.14 Furthermore, exacerbations accelerate the deterioration of lung function,15 which in turn increases the likelihood and severity of further exacerbations.
However, there has been no report on the biology of CLDN5 in COPD. We thus investigated the association between circulating CLDN5 levels and clinical variables in patients with COPD.
MATERIALS AND METHODS
Subjects
We collected clinical data from 30 COPD patients registered in a cohort of the Genome Research Center for Allergy and Respiratory Diseases in Korea. All patients were randomly recruited from Soonchunhyang University Bucheon Hospital. The biospecimens and data used for this study were provided by the biobank of Soonchunhyang University Bucheon Hospital, a member of the Korea Biobank Network.
Both male and female adults were enrolled, aged 40 years and over and with a clinical diagnosis of stable COPD or moderate-to-severe COPD (GOLD 2015 criteria)16 and a smoking history of at least 10 pack-years. Both current and ex-smokers were included. Inclusion depended on confirmed post-bronchodilator spirometry criteria: forced expiratory volume in 1 second (FEV1) ≥ 30% and < 70% of the predicted normal and FEV1/forced vital capacity (FVC) < 0.70. Key exclusion criteria included a history of a clinically significant disease other than COPD that could interfere with the assessments (including asthma), and a history of malignancy within the past 5 years.
All subjects17 underwent standardized assessments, which included analyses of the complete blood cell count with differential counts, chest posteroanterior radiography and spirometry. All data were collected at the time of stable status and during the period of exacerbation. The healthy control subjects were recruited from the spouses of patients or members of the general population, based on the following criteria: 1) negative responses on a screening questionnaire for respiratory symptoms and other respiratory diseases, 2) FEV1 values >80% of predicted values, and 3) normal findings on simple chest radiographs. Exclusion criteria included respiratory infection during inclusion, asthma, vocal cord dysfunction, obstructive sleep apnea, Churg-Strauss syndrome, cardiac dysfunction, allergic bronchopulmonary aspergillosis or poor adherence to treatment. This study was approved by Soonchunhyang University's Institutional Review Board.
COPD exacerbation: Defined as a worsening of respiratory symptoms that required treatment with oral corticosteroids, antibiotics or both.
Spirometry
Spirometric testing was performed in accordance with American Thoracic Society (ATS)/European Respiratory Society (ERS) standards18 using established reference values19 with modification.17 Spirometry was performed before and after bronchodilator use. Baseline FVC and FEV1 measurements were obtained in the absence of bronchodilator use (within 8 hours).20 Basal and post-bronchodilator FEV1 and FVC values were measured. Vmax Series 2130 Autobox Spirometer (Sensor Medics, Yorba Linda, CA, USA) was used.
Enzyme-linked immunosorbent assay (ELISA)
Plasma CLDN5 level was measured by ELISA (USCN, Wuhan, China). To compare results from different plates, test sample optical densities (ODs) were adjusted relative to the positive and negative control samples supplied in each kit. The mean OD of duplicate wells was calculated. The index value of each tested serum sample was calculated by the following formula: index = (OD of tested serum − OD of negative control)/(OD of positive control − OD of negative control) × 100. The lower limit of detection was set at 0.061 ng/mL for CLDN5 as per the manufacturer's recommendations.
Statistical analysis
The data were entered into the SPSS statistical software package (ver. 14.0; SPSS Inc., Chicago, IL, USA) for analysis. The data are expressed as means ± standard deviation (SD) or standard error of the mean (SEM). Group differences were compared using the 2-sample t test, Mann-Whitney test or Pearson's χ2 test for normally distributed, skewed and categorical data, respectively. Differences between the patient populations were analyzed by the χ2 test with Fisher's exact test when low expected cell counts were encountered. A P value of < 0.05 was considered to indicate statistical significance.
RESULTS
Clinical characteristics of the subjects
The period of study was from January 2014 to November 2017. The clinical characteristics of 30 COPD patients (mean age = 67.61 ± 6.4 years) and 30 control subjects (66.3 ± 7.4 years) are presented in Table. The initial FEV1 (%pred.), FVC (%pred.) and FEV1/FVC values were significantly lower in COPD patients than in control subjects. BMI was significantly lower in patients with COPD than in control subjects. FEV1%pred., FVC%pred. and FEV1/FVC values were significantly lower in patients with exacerbated COPD than in those with stable COPD. Blood neutrophil percents were significantly higher in exacerbated COPD patients than in those with stable COPD.
Table
Clinical characteristics in patients with COPD
Data expressed as mean ± standard deviation.
COPD, chronic obstructive pulmonary disease; NS, non-smokers; ES, ex-smokers; CS, current smokers; ND, not done; ICS, inhaled corticosteroid; OCS, oral corticosteroid; BMI, body mass index; FEV1, forced expiratory volume in one second; %pred., % of predicted value; FVC, forced vital capacity; WBC, white blood cells.
*P < 0.05 compared with control subjects; †P < 0.05 compared with stable COPD.
Alterations of CLDN5 levels in patients with COPD
The mean plasma CLDN5 level of patients with COPD was 0.63 ± 0.05 ng/mL and that of healthy controls was 6.9 ± 0.78 ng/mL (Fig. 1A, P = 0.001). The mean plasma CLDN5 level was 0.71 ± 0.05 ng/mL in patients with exacerbated COPD and 0.63 ± 0.04 ng/mL in those with stable COPD (Fig. 1B, P < 0.05).
Fig. 1
Plasma CLDN5 levels in patients with COPD and control subjects (A), and in patients with stable or exacerbated COPD (B).
NC, normal control; CLDN5, claudin-5; COPD, chronic obstructive pulmonary disease; STA, stable; EXA, exacerbated.
*P < 0.05, control vs. STA COPD; †P < 0.05, STA vs. EXA COPD.

Relationship of circulating CLDN5 levels with clinical variables in patients with COPD
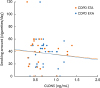
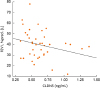
The plasma CLDN5 level was correlated with the smoking amount in COPD patients including stable and exacerbated status (Fig. 2, r = −0.530, P = 0.001, COPD STA r = −0.007, COPD EXA r = −0.006). The plasma CLDN5 level in COPD patients including stable and exacerbated status was correlated with FEV1%pred. (Fig. 3, r = −0.481, P = 0.037). The plasma CLDN5 level was not correlated with age.
Fig. 2
Relationship between plasma CLDN5 level and smoking amount in COPD subjects. The plasma CLDN5 level was correlated with smoking amount (r = −0.530, P = 0.001, COPD STA r = −0.007 orange line, COPD EXA r = −0.006 blue line).
CLDN5, claudin-5; COPD, chronic obstructive pulmonary disease; STA, stable; EXA, exacerbated.
DISCUSSION
In this study, we investigated the role of circulating CLDN5 in patients with stable or exacerbated COPD. Several novel findings emerged. First, we demonstrated that the CLDN5 level decreased in patients with COPD. Secondly, we found that the CLDN5 level increased in patients with COPD exacerbation. Thirdly, the CLDN5 level was correlated with clinical variables, such as smoking amount, BMI and lung function, suggesting that CLDN5 be involved in pathogenesis of COPD.
TJs act as a semipermeable barrier (or gate) to the paracellular transport of ions, solutes and water as well as cells, and are considered to also function as a fence that divides apical and basolateral domains of plasma membranes.2223 In addition, like other cell–cell and cell–extracellular matrix junctions24 TJs coordinate a variety of signaling and trafficking molecules that regulate cell differentiation, proliferation and polarity, thereby serving as a multifunctional complex.252627 These functions of TJ are critical for establishing via epithelial and endothelial cell sheets, distinct tissue compartments within the body as well as for maintenance of homeostasis. The CLDN5 expressed highly by the endothelium and also expressed in alveolar epithelial cells.152829 Our previous study of acrolein-induced acute lung injury in different mouse strains showed that CLDN5 more increased in injury-resistant strains as compared with injury-sensitive strains,16 indicating that lung CLDN5 expression tends to be inversely correlated with the severity of lung injury. In HIV-1-infected patients with interstitial pneumonitis, CLDN5 was down-regulated in lung tissue.7
The alveolar barrier has dual functions, which plays a protective role in acute respiratory distress syndrome through promoting blood-brain barrier function and has increased sensitivity to ventilator-induced lung injury.1
COPD, the fourth-leading cause of death worldwide,30 is induced by environmental exposure to noxious gases, particles, indoor fumes and pathogens, and most importantly, by active or passive exposure to cigarette smoke. COPD is characterized by progressive airflow limitation due to an abnormal inflammatory response and structural pathological remodeling of the lung due to exposure to these environmental agents.30 COPD is an inflammatory disorder characterized by progressive airflow limitation. Exacerbations of COPD lead to a progressive decline in lung function, with even a single episode of exacerbation having a prolonged effect on health status.3132 COPD exacerbations aggravate pulmonary emphysema by triggering bacterial or viral infections. The mechanisms by which COPD inflammation causes TJ alterations are unclear.34 In this study, neutrophil numbers in blood were more increased in patients with COPD than those in control subjects as well as in exacerbated patients than in stable patients with COPD, suggest that neutrophilic inflammation can cause aggravate COPD status.
Airway microvascular permeability and disruption of vascular integrity are increased in the airways of patients with COPD, disease exacerbation or lung injury.34353637 Increased permeability of endothelial cells could be disintegration of TJs,343536 which causes paracellular permeability to solutes and large molecules leading to airway inflammation.33 The expression of structural membrane proteins — such as ZO-1, CLDN5 and AmotL1 — is related to TJ permeability.
However, the role of claudins in patients with COPD has not yet been fully elucidated. It is likely that patients with COPD who are former or current smokers have endothelial dysfunction, resulting in a change in lung function. Clearly, these observations need to be clarified in future studies.34 Therefore, we investigated the impact of CLDN5 of the endothelial parts of the alveolar barrier in patients with exacerbated or stable COPD. The CLDN5 level more decreased in patients with COPD compared with healthy controls and more increased in those with exacerbated COPD compared with those with controlled COPD, suggesting that CLDN5 may be a diagnostic marker and therapeutic target in COPD. Further studies are needed to clarify the role of CLDN5 in the pathogenesis of COPD.
Cigarette smoke contains a complex mixture of approximately 4,800 chemicals,37 hampering determination of the cellular mechanisms that lead to smoking-related features of COPD and airway injury. A recent study demonstrated a transient decrease in airway epithelial barrier function in bronchial epithelial cells.38 In addition, human adenocarcinoma Calu-3 cells exposed to mainstream smoke exhibited decreased transepithelial electrical resistance as a result of a highly regulated yet undefined process, rather than the cytotoxicity of cigarette smoke.39 Down-regulation of apical TJ components including claudins was observed following chronic exposure of bronchial epithelial cells to cigarette smoke extract.4041 However, there are no data on the endothelial TJ protein CLDN5 in patients with COPD. In the present study, there was a negative relationship between CLDN5 and the smoking amount, suggesting that smoking may damage lung endothelial cells and down-regulate CLDN5. COPD is defined as “an inflammatory disease of the lungs caused by long-term inhalation exposure to noxious substances such as tobacco smoke.” The most important causative factor for COPD is cigarette smoke (current and passive smoking). Furthermore, smoking promotes exacerbation of pulmonary function decline with aging, and the decrease in pulmonary function is greater compared with that in nonsmokers.41 In this study, the CLDN5 level was negatively correlated with lung function, suggesting that smoke affects endothelial TJs, leading to structural damage and deterioration of lung function.
Mild/moderate COPD may result in structural and functional abnormalities of skeletal muscles and reduce endurance, even in the absence of significant muscle wasting.424344 Body composition in mild/moderate COPD is similar to that in healthy subjects, albeit with decreased fat-free mass or a higher fat percentage. In this study, the level of CLDN5 and BMI were decreased in COPD patients than in control subjects, suggesting that a decrease in body mass results in a decrease in blood vessel mass or integrity, leading to a decrease in the CLDN5 level.
In conclusion, these data suggest that CLDN5 may be involved in the pathogenesis of COPD and related with clinical variables for COPD, which could lead to further step for the evaluation for CLDN5 in COPD.
 XML Download
XML Download