

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The worldwide emergence of multidrug-resistant tuberculosis (MDR-TB) and extensively drug-resistant tuberculosis (XDR-TB) threatens global efforts to control tuberculosis12. Isoniazid (INH) and rifampicin (RFP) are the main components of first-line anti-tuberculosis treatment and are effective drugs for the treatment of tuberculosis345. MDR-TB is resistant to INH and RFP, and the emergence of MDR-TB is placing an increasing burden on South Korea456.
Mycobacterium tuberculosis can acquire resistance to RFP through mutations in rpoB, which encodes the β subunit of RNA polymerase789. Mutations in rpoC, which encodes the β′ subunit of RNA polymerase, have also been associated with increased in vitro fitness and were overrepresented in MDR-TB isolates from countries with high MDR-TB burdens1011. One study showed that M. tuberculosis isolates harbouring an rpoB mutation also carried nonsynonymous mutations in rpoC
10.
In this study, we investigated rpoC mutation patterns in drug-resistant and susceptible M. tuberculosis isolates from patients in South Korea to determine the epidemiological relevance of rpoC nonsynonymous mutations in a high-incidence setting of MDR- and XDR-TB.
Materials and methods
1. Mycobacterial isolates and susceptibility testing
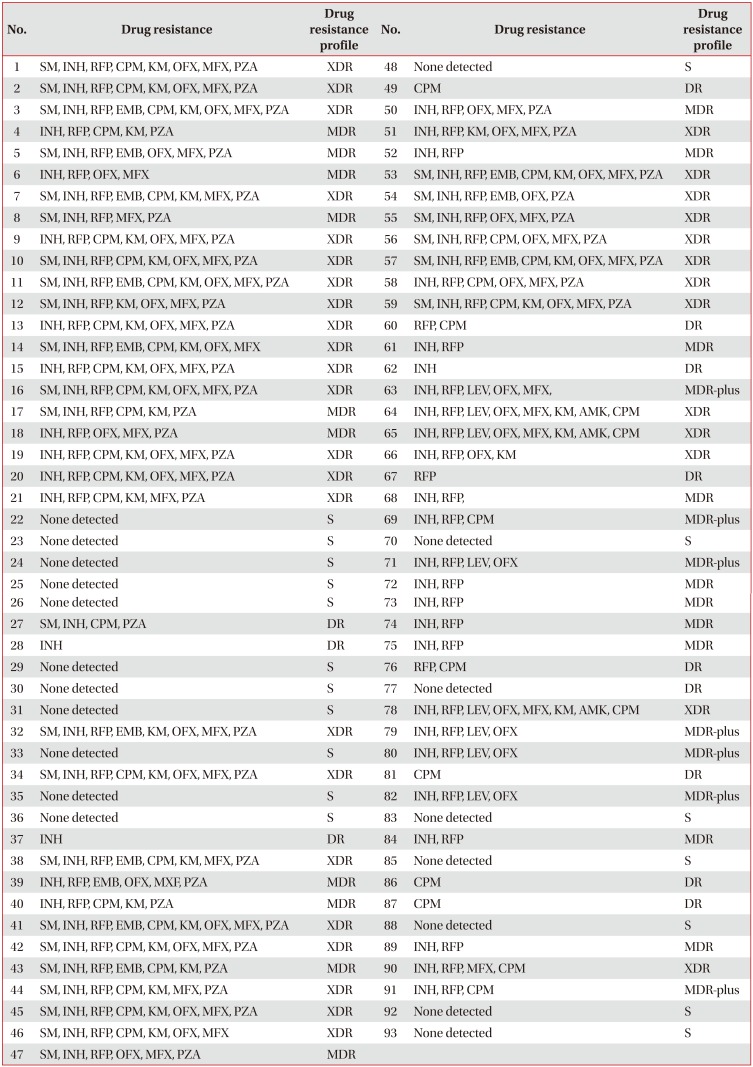
Ninety-three M. tuberculosis isolates with clinically observed drug resistance were collected at National Masan Hospital and Pusan National University College of Medicine in South Korea and were cultured to determine their susceptibility to anti-tubercular agents (Table 1). Each isolate was cultured on Löwenstein-Jensen medium at 37℃ for 3–4 weeks and tested for resistance to critical concentrations of capreomycin (40 µg/mL), ethambutol (2.0 µg/mL), INH (0.2 µg/mL), kanamycin (40 µg/mL), ofloxacin (2 µg/mL), streptomycin (4 µg/mL), pyrazinamide (100 µg/mL, Wayne's pyrazinamidase assay12), and RFP (40 µg/mL). M. tuberculosis H37Rv (American Type Culture Collection [ATCC] 27294) was used as a positive control in all of the experiments. The following drug-resistant profiles were defined: MDR, resistance to both RFP and INH; MDR-plus, resistance to any of the second-line injectable drugs (INH+RFP+Inj.D) or to any fluoroquinolone drugs (INH+RFP+FQ); XDR, extensively drug-resistant; DR, drug resistance other than MDR (including MDR-plus and XDR); and S, susceptibility to all of the drugs. Sixty-six M. tuberculosis isolates were RFP resistant (Table 1).
This study was approved by the institutional review board (IRB) at the International Tuberculosis Research Centre, and all subjects signed an informed consent form.
2. Polymerase chain reaction and sequencing of rpoC
The rpoC region (1,730 bp) was amplified by polymerase chain reaction (PCR) using the GeneAmp PCR System 9600 (PerkinElmer, Foster City, CA, USA) with primers 5′-CGAAAACCTCTACCGCGAAC-3′ and 5′-CACGGAAGGAGGACTTGACC-3′10.
Briefly, the PCR parameters were 5 minutes at 95℃, followed by 40 cycles of 45 seconds at 94℃, 45 seconds at 60℃, and 60 seconds at 72℃, with a final extension step at 72℃ for 10 minutes. The PCR products were purified using a QIAEX II Gel Extraction Kit (Qiagen Inc., Mainz, Germany) according to the manufacturer's instructions and sequenced using a BigDye Terminator cycle sequencing kit with AmpliTaq DNA polymerase (Applied Biosystems, Foster City, CA, USA) using primers 5′-CGAAAACCTCTACCGCGAAC-3′ and 5′-CACGGAAGGAGGACTTGACC-3′10. The nucleotide sequences were analyzed using BioEdit software version 5.0.9.1 (Ibis Biosciences, Carlsbad, CA, USA), Chromas version 2.33 (Technelysium, Brisbane, QLD, Australia, http://www.technelysium.com.au/chromas.html), and the Basic Local Alignment Search Tool (BLAST, National Center for Biotechnology Information, Bethesda, MD, USA, http://blast.ncbi.nlm.nih.gov/Blast.cgi). Mutations in the rpoC-encoding regions were defined as any nucleotide changes that led to translational changes in RpoC compared with the RFP-susceptible strain, H37Rv (ATCC 27294).
Results
Ninety-three clinical isolates were included in this study, and all were from South Korean patients. Drug susceptibility testing identified 75 multidrug-resistant isolates: 20 were categorized as MDR-TB, seven were categorized as MDR-plus, 36 were categorized as XDR-TB, and 12 were categorized as DR-TB. Moreover, 66 of the cultured M. tuberculosis isolates were found to be RFP-resistant. Eighteen isolates were categorized as S (Table 1).
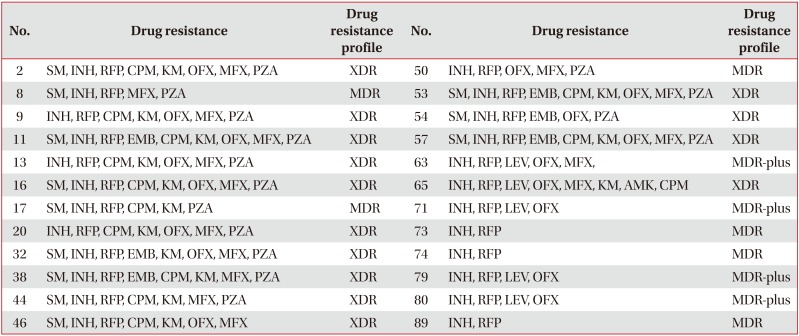
rpoC PCR products were amplified from 93 isolates and sequenced. Fifteen different types of mutations were identified in 24 isolates (24/93, 25.8%), all of which were resistant to both INH and RFP. The rpoC mutation rate of the MDR- and XDR-TB isolates was 37.0% (10/27) and 38.9% (14/36), respectively (Table 2).
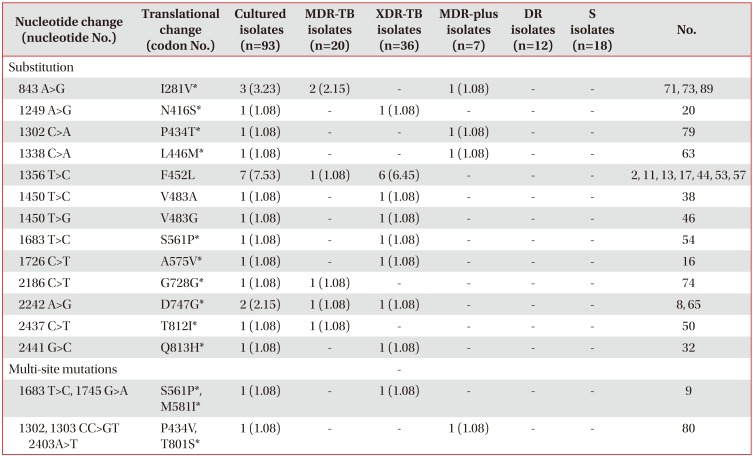
Single mutations (22/24, 91.7%) and multiple mutations (2/24, 8.3%) in the rpoC region were identified, but no deletion nor insertion mutations were detected in any of the isolates. No mutations were identified in the rpoC region of any drug-susceptible strains. A mutation at codon 452 (nt 1356) was the most common mutation (7/24, 29.2%) and a mutation at codon 531 (nt 1594), which is the most frequently mutated nucleotide in rpoB , was also detected in these isolates (Supplementary Table S1)789. Twelve different mutation sites (at codon 281 [nt 843], 416 [nt 1249], 434 [nt 1302], 446 [nt 1338], 561 [nt 1683], 575 [nt 1726], 581 [nt 1745], 728 [nt 2186], 747 [nt 2242], 801 [nt 2403], 812 [nt 2437], and 813 [nt 2441]) are reported for the first time in this study1011; these new mutations are shown in Table 3.
Discussion
RFP is one of the principal first-line drugs used in combination chemotherapy for tuberculosis, and RFP resistance is a valuable surrogate marker of MDR-TB. Over 90% of RFP-resistant clinical M. tuberculosis isolates possess genetic alterations in rpoB28.
rpoC encodes the β′ subunit of RNA polymerase, and Comas et al.11 suggested that the acquisition of particular mutations in rpoC by RFP-resistant M. tuberculosis strains leads to the emergence of MDR strains with high fitness over time. Additionally, de Vos et al.10 showed that nonsynonymous mutations in the rpoC region were prevalent among RFP-resistant isolates in a South African high-burden setting; these mutations were strongly associated with the transmission of RFP-resistant strains.
rpoC mutations have not been studied in South Korea; thus, we investigated the rpoC mutation patterns in drug-resistant and susceptible M. tuberculosis isolates from patients in South Korea. Fifteen different types of mutations were identified, 12 of which were reported for the first time in this study (Table 3)1011. A mutation at codon 452 was the most common mutation (7/24, 29.2%), and a mutation at codon 531, which is the most frequently mutated nucleotide in rpoB, was also detected in these isolates (Supplementary Table S1)789.
Mutations were found only in the MDR-TB isolates and no rpoC mutations were identified in any of the drug-susceptible strains (Tables 2, 3).
Therefore, we suggest that rpoC mutations could be used DNA-based diagnosis for detection of INH and RFP drug resistance; however, more extensive studies on larger collections of isolates are needed.
In summary, 15 different types of mutations were identified. Substitutions in a single nucleotide were the most common mutation found (22/24, 91.7%), and mutations were found only in dual INH- and RFP-resistant isolates in this study.
 XML Download
XML Download