

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Despite the existence of evidence-based guidelines, strategies and educational material for patients, asthma control remains a problem in the community. The reasons for this are multifactorial and well document and include incorrect diagnosis, co-morbidities, such as allergic rhinitis, smoking, suboptimal medication dosing, and other phenotypes1. In this, inhaler technique is an important medication-related issue. While it is often not the only problem, it appears to consistently be a problem and often co-exists with poor adherence2345678. Despite the complexity of the relationship between adherence, inhaler technique and disease control, improving inhaler technique and ensuring that the most appropriate inhaler is used by the patient, is critical to achieving good disease outcomes9101112.
In order to overcome the issue of inhaler technique and effective drug delivery, device designers work to make innovative devices that will enable the effective delivery of drug to the lung13. However, these innovations are often complex and from the health care providers perspective, it comes down to several more fundamental factors, which also include inhaler technique.
Technical Characteristics of the Device
The key to using inhaler devices to deliver medication in respiratory diseases is to ensure that medication is delivered effectively to the lungs, i.e., that drug delivery from the inhaler devices results in drug deposition in the lower airways. Deposition of drug into the lungs is directly correlated with the clinical effects of the drug1415 and therefore is an important feature of device design.
While it is accepted that optimal inhaler use is more than just selecting the inhaler, it is important for health care professionals to understand the key technical features of devices. It is often within these technical features that device designers and manufacturers build innovation and sophisticated technology. These technical features are often promoted as the key difference between the different inhalers and certainly do impact on the specific way in which an inhaler is to be used.
There are a range of technical characteristics that are important when it comes to the design of inhalers; however, aerosol velocity, aerosol duration, particle size, and internal device resistance are most commonly noted16171819. Below is a discussion of these features as they relate to patient use and potential considerations.
1. Aerosol velocity and aerosol duration
Aerosol velocity relates to the velocity of the aerosol as it leaves the inhaler i.e. how quickly the aerosol comes out of the device; while aerosol duration relates to the length of time it takes for a dose of the aerosol to be released from the inhaler. Both aerosol velocity and aerosol duration are related to pressured metered dose inhalers (pMDI) as they relate to a device in which aerosol is released from the device and the speed and duration of this research can not be controlled by the user (i.e., it is independent of inspiratory flow of the user). In practical terms, both aerosol velocity and aerosol duration have implications with regards to the patient's ability to coordinate inspiration and actuation of their pMDI, and subsequently to the amount of drug deposited either into the airways or into the orophargyneal cavity20.
With regards to aerosol velocity, the concept is that the faster the aerosol velocity, the more critical the co-ordination of inspiration. If a patient actuates too early, i.e., before they start to inspire or if a patient coordinates too late, i.e., after they have almost finished inspiring, suboptimal dose of aerosol will be deposited in the lungs and instead will be deposited in the oropharyngeal cavity.
With regards to aerosol duration, the concept is that the longer it takes for all the drug to be released from the pMDI, the more forgiving the device is in terms of coordinating the inspiration and device actuation, i.e., the longer the aerosol duration, the longer time it takes for all the drug to be released and minimizing the impact of poor coordination.
Both aerosol velocity and aerosol duration become important technical features for device consideration for patients who continue to have trouble coordinating inspiration and device actuation, even following repeated training.
2. Particle size
It is well established that in order for the drug particles released from a device to penetrate into the lungs, they need to be of a particular particle size212223. A highly efficient device is one, which releases a high proportion of drug within the respirable particle size of 1–5 µm242526. That is, an efficient device is one in which has a high fraction of the emitted dose from an inhaler that has the potential to be deposited into the lungs. This is known as the fine particle dose (also the respirable dose). The higher the fine particle dose released from the inhaler, the more efficient the drug as a higher proportion of delivered drug is deposited in the lower airways. Consequently, the more drug deposited in the lower airways, the less deposited higher up in the respiratory tract, including the oropharyngeal cavity16.
3. Internal device resistance
Internal devices resistance is a technical characteristic of dry powder inhalers (DPIs), which relates to the “force” required to be created inside the device, in order for a fine particle dose to be released. This “force” is generated by the inhalation rate used by the patient when using the DPI, together with the resistance (and hence design) inside an inhaler27. Devices with high internal resistance require the patient to inhale more forcefully from the inhaler than devices with low resistance. There is a large difference between inhalers when it comes to internal resistance28 and this impacts on the way in which the different inhalers need to be used.
In practical terms, this is most directly related to the inspiratory flow that can be generated by the patient, which, in some cases when airway function is severely compromised, may compromise the fine particle fraction delivered into the lungs27. It should be noted that while high resistance inhalers require more forceful inspiration, forceful inspiration through a low resistance inhaler may also be problematic, having implications for drug deposition in the oropharyngeal cavity. Therefore, when it comes to internal resistance of an inhaler, it is important for the patient to follow the instructions issued by the manufacturer.
Use of the Device
While much research and development goes into the design and manufacture of new and novel inhalers, meta-analysis has shown that as long as the patient uses their device correctly, i.e., are able to demonstrate correctly technique as articulated in the manufacturer's instructions, good clinical outcomes can be achieved2930. Therefore, the way in which the patient uses the device is critically important.
It has long been established and continues to be recognized that the inhaler technique of patients using inhaler devices is poor, with a high proportion of patients not being able to demonstrate correct use of their inhaler31. The issue of poor inhaler technique is important and the importance of this issue is reflected, in the fact that inhaler technique is noted over 70 times in the latest global strategies for the management of asthma and chronic obstructive pulmonary disease (COPD)3233. In fact, outside of the process of diagnosis, inhaler technique is noted within the reports across all areas within the management process, whether it be in training a patient on inhaler technique when the device/medication is first prescribed or reviewing inhaler technique over time.
The reason for this focus on inhaler technique is because evidence indicates that poor inhaler technique often co-exists with poor adherence and poor disease control23456. In fact, the CRITIKAL study has identified that specific inhaler technique errors (i.e., “critical” errors) are associated with increased risk of negative asthma outcomes, including poor control and increased exacerbations34. While recent research exploring inhaler technique in patients with chronic obstructive pulmonary disease finds a similar relationship between poor inhaler technique and severe COPD exacerbations35. Further to this, research shows that when inhaler technique is corrected, improvements in asthma control are observed and risk of future exacerbations is reduced9101112.
Improving Inhaler Technique
After decade of recording inhaler technique, it can be said that inhaler technique research has been a field of research in itself. However, from the practical perspective and certainly for health care providers, there are several key principles to consider when attempting to ensure that correct technique is used.
1. Inhaler technique is devices specific
Inhaler technique is device specific, i.e., regardless of device type, device technique is specific for the actual device. For this reasons, patient and health care provider organizations produce device specific checklists and videos and these need to be used to ensure that each device is used correctly. Device-specific resources are easily available on the internet and mostly free of charge. An example of the breadth of resources available in Australia is found on a series of website produced by national organisations such as the National Asthma Council3637 and NPSMedicineWise38.
2. The method of training inhaler technique is important
Although most patients can be taught how to use their inhaler device, the most effective method of training includes a one-on-one physical demonstration with a placebo inhaler394041. This needs to be completed by a health care professional or health educator who is able to use an inhaler correctly and is knowledgeable with regards to some of the common misconceptions regarding different devices42. Research shows that the ability of health care providers to demonstrate correct technique is poor and without training, most devices are not intuitive to use43. There is evidence that utilizing technology to provide patients with feedback on specific errors may also be helpful44.
3. Inhaler technique is not stable
Inhaler technique is not necessarily stable and even though a patient can be taught the skill, inhaler technique education needs to be repeated to ensure that patients maintain correct technique over time. Research, conducted with a range of different inhaler devices, consistently shown that even though a majority of patients can be taught how to use a device (i.e., they are able to learn the skill), up to 50% of patients come back to the health care provider 1 month later, making inhaler technique errors404445. Therefore, inhaler technique needs to be checked and, where appropriate, corrected over time.
4. Inhaler technique and adherence are related
In addition to the fact that poor inhaler technique and poor adherence commonly co-exist2345678, there is evidence that these two constructs may be related in a more fundamental way7. This follows research showing that inhaler technique maintenance is related to patient psychosocial factors, such as motivation46; while further exploration of this motivation provides insights that patients' perceptions of the threat posed by their asthma, their perceived confidence in the strategies suggested for managing their asthma and their confidence in carrying out those strategies are linked to their ability to retain correct inhaler technique over time47. Research further goes to show that recent self-reported adherence, may be a predictor for future inhaler technique maintenance48.
5. Patient preference
When deciding on which inhaler device might best suit a patient, it is important to consider that the factors important to a patient may not necessarily be those important for the health care provider. The concept of a patient using an inhaler because they prefer it is an interesting one. There have been a numbers of studies exploring patient satisfaction and preference, attempting to link these constructs to the patient's ability (or willingness) to use their inhaler4950515253. It should be noted that often the studies reporting patient preference or satisfaction do so as an aside to comparing two or more inhalers on some other aspect of use and then asking patients for their preferences. Invariably, patients report a preference for the new inhaler. It is difficult to interpret the importance of this to the actual use of the inhaler. What is known is that in real-life, patients rarely get a choice of which inhaler they would like to use and often consider the inhaler and the medication contained in it as one entity54.
The Strength and Weakness of Different Devices in Practice
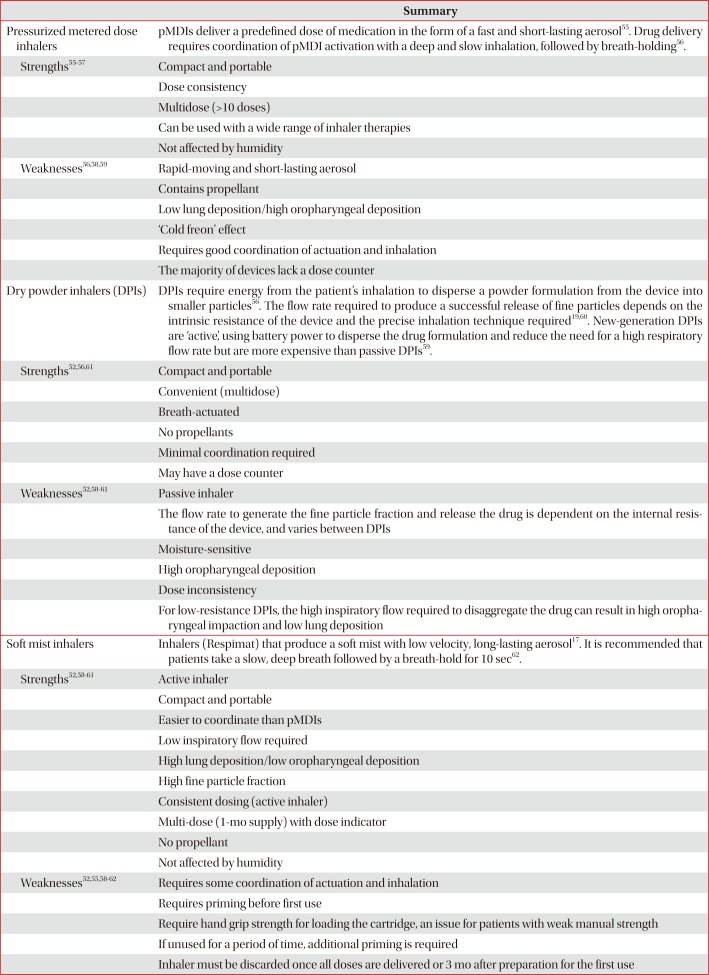
Given the consideration that devices different in how they can be used from a technical perspective, there are therefore considerations that can be made regarding the use of inhalers, and potentially the importance of selecting an inhaler that will suit the patient. Table 1 provides a simple summary of key aspects of the three main devices types and some of the specific factors that may be considered strengths and weaknesses for use. Some of these factors relate to the technical features of the devices, others relate to user aspects, which may impact on the likelihood of the device being used appropriately. Figure 1 provides a guide to a decision-making process, which can be used health care providers by health care professionals to guide selection of devices.
Conclusion
There are a number of factors that could be considered in in selecting a device for a patients; however, it is important to note that ultimately, regardless of the inhaler devices prescribed, unless the patient is able to use the inhaler correctly and as recommended by the health care professional, only sub-optimal disease management will be achieved. Therefore, following the recommendation of any inhaled medication, it is important for health care professionals to effectively train the patient in the use of their inhaler and to regularly follow up with any addition inhaler technique education to ensure that the patient maintains correct inhaler technique over time.

 XML Download
XML Download