

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Osteoporosis is a well-known complication of chronic inflammatory airway disease attributed to the systemic inflammatory response to the disease itself as well as due to the use of inhaled corticosteroids (ICSs) to control the disease1. ICSs may lead to osteoporosis as glucocorticoids affect bone metabolism by stimulating osteoclast-mediated bone formation and the metabolism of calcium and sex hormones234. However, some recent studies have emphasized the role of the inflammatory response in chronic inflammatory airway disease in the development of osteoporosis567. Osteoporosis is more common in patients with chronic obstructive pulmonary disease (COPD) than in those with asthma, even when they do not receive long-term corticosteroid treatment. This is explained by the role of inflammatory cytokines, such as tumor necrosis factor (TNF)-α, that stimulate osteoclastic bone resorption5. Compared to patients with asthma, those with COPD have a higher systemic inflammatory response and secrete TNF-α, thereby resulting in more severe osteoporosis7. Asthma-COPD overlap syndrome (ACOS) is a recently categorized disease that has features of both asthma and COPD, but with a poorer outcome8910. However, there have not been many previous studies examining the relationship between osteoporosis and ACOS. Therefore, we compared osteoporosis in patients with ACOS versus those with asthma or COPD.
Materials and Methods
1. Study design
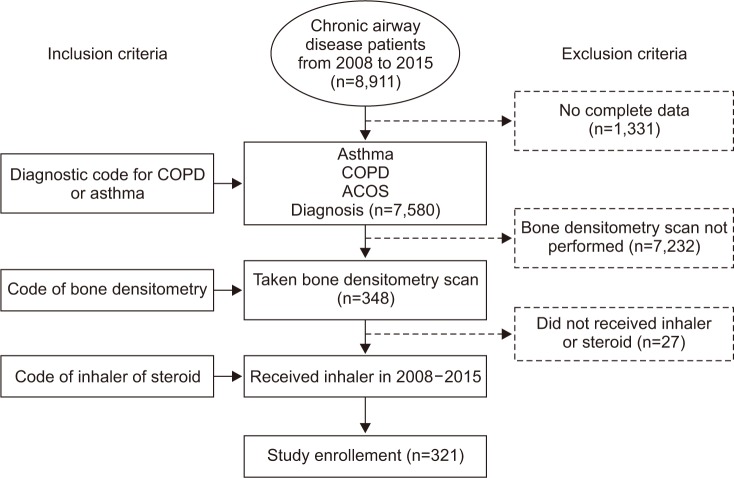
We reviewed the medical records of patients, at Korea University Guro Hospital (Seoul, Korea), who had a chronic inflammatory airway disease (asthma, COPD, or ACOS), over 20 years old, used an inhaler, and had undergone a bone densitometry scan between January 2008 and December 2015 (Figure 1). Our institutional review board approved the study (KUGH15140). Written informed consent was provided by the patients and the study conformed to the tenets of the Declaration of Helsinki. A diagnosis of COPD was made according to the American Thoracic Society and Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines. An asthma diagnosis was made based on the Global Initiative for Asthma (GINA) guidelines. An ACOS diagnosis was made when two major and two minor criteria were met among COPD patients11. The major criteria included a positive bronchodilator test result (increase in predicted forced expiratory volume in the first second [FEV1] of 15% or greater and 400 mL or greater), the presence of eosinophilia in the sputum, and a history of asthma. The minor criteria included a high total IgE level, a history of atopy, and a positive bronchodilator test result (increase in FEV1 12% or greater and 200 mL or greater) on two or more occasions11. A cross-sectional design was used. We then evaluated the prevalence of osteoporosis and compared bone mineral density (BMD) patients with three different types of airway diseases.
2. Methods
BMD measurements of the femoral neck, total femur (which includes the femoral neck, trochanter, and intertrochanter area), and lumbar spine (L1–4) were conducted using dual-energy X-ray absorptiometry (DXA; Hologic Discovery A, Hologic, Bedford, MA, USA). To analyze data, we used BMD measurements or a T-score based on the sex-specific mean for healthy, young asian adults, which was provided by the manufacturer. A T-score (the lowest T-score of the three measured locations; lumbar, total femur, and femur neck) that was 2.5 standard deviations (SDs) below the average value was indicative of osteoporosis, in accordance with the World Health Organization criteria. We evaluated the following variables in patients with asthma, COPD, or ACOS: age, sex, body mass index (BMI), smoking history (over 10 pack-year current or ex-smoker was considered to have smoking history), T-score, BMD (g/cm2), predicted FEV1% and bronchodilator response (BDR; %) at the time of BMD taken, COPD Assessment Test (CAT) score, Asthma Control Test score, serum total IgE (IU/mL), sputum eosinophil (%) and type of inhaler and medications used for airway disease.
3. Statistical analysis
Clinical data are presented as the mean±SD, depending on the distribution. ANCOVA was used to compare age and sex adjusted means. Student's t test and ANOVA with a post-hoc test (using Bonferroni method) were used for analysis of continuous variables, while Fisher exact test was used for categorical variables. BMD and other variables were analyzed using multivariate linear regression. Statistical significance was defined as p<0.05. All statistics were analyzed using SPSS version 20.0 software (IBM Corp., Armonk, NY, USA).
Results
1. Characteristics of patients with and without osteoporosis
Three hundred and twenty-one patients were analyzed: 138 with asthma, 46 with ACOS, and 137 with COPD. Among them, 193 (60.1%) were diagnosed with osteoporosis (53.6% of asthma 65.2% of ACOS, and 65.0% of COPD; p=0.118). Patients with osteoporosis were more likely to be of the female sex, older, with a lower BMI, a lower predicted FEV1, and a higher CAT score. BMI and CAT were different between patients with and without osteoporosis after adjusting for age and sex by ANCOVA (p<0.05).
2. Characteristics of patients according to asthma, COPD, and ACOS
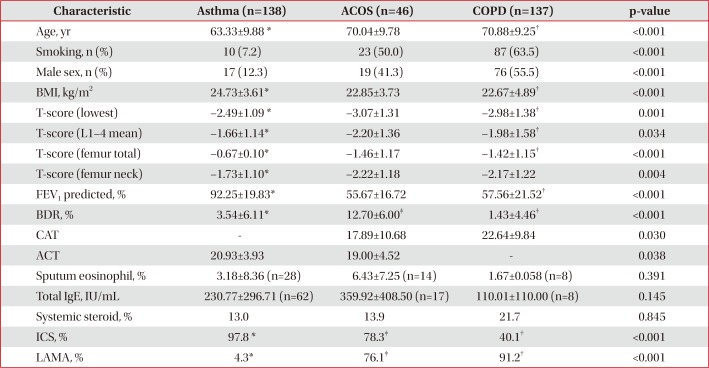
The baseline characteristics of patients based on disease entities are presented in Table 1. ACOS patients were older and leaner than were patients with asthma. The predictive ability (%) of FEV1 for ACOS was lower than for asthma, and BDR (%) of ACOS was the highest among the three disease entities. Furthermore, ACOS patients had worse symptom scores than did those with asthma or COPD.
3. Comparison of BMD among patients with asthma, COPD, and ACOS
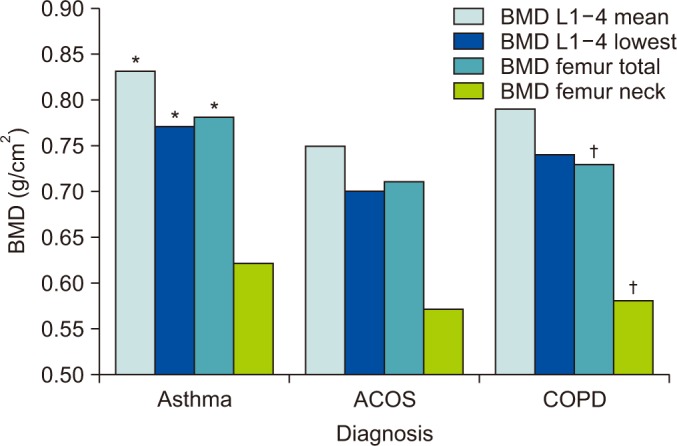
Increased ICS use was seen in patients with asthma rather than in patients with ACOS or COPD. However, patients with ACOS had a lower mean BMD (L1–4 mean, femur) than did patients with asthma regardless of ICS use after adjusting for age, sex, BMI, smoking, and ICS use (ANCOVA, BMD [L1–4 mean] estimated marginal mean±standard error [0.84±0.11 in Asthma, 0.76±0.02 in ACOS, 0.77±0.02 in COPD], p=0.007). BMDs of ACOS and COPD had no significant differences, but ACOS generally had lower T-scores and BMD (L1–4, femur) than did patients with COPD (Table 1, Figure 2).
4. Association between BMD and other clinical parameters
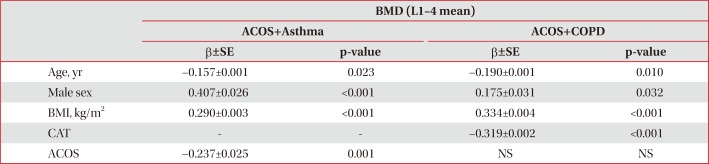
When multivariate linear regression analysis was performed among patients with ACOS and asthma, BMD (L1–4 mean) was negatively associated with age and a diagnosis of ACOS. Meanwhile, BMD was positively associated with male percentage and BMI after adjusting for age, sex, BMI, smoking, ICS use and diagnosis (Table 2). When multivariate linear regression analysis was performed among patients with ACOS and COPD, after adjusting for age, sex, BMI, smoking, ICS use and diagnosis, BMD (L1–4 mean) was negatively associated with age and CAT, while it was positively associated with male percentage and BMI (Table 2). However, BMD (L1–4 mean) was not associated with a diagnosis of ACOS compared to COPD significantly.
5. Associations of ICS use and osteoporosis
One hundred and forty-four patients (44.9%) used fluticasone/salmeterol, 70 (21.8%) used budesonide/formoterol, and 166 (51.7%) used tiotropium. Other inhalers (budesonide, fluticasone, indacaterol, and ciclesonide) were prescribed in less than 5%, so they were excluded in analysis. There were no significant differences in the prevalence of osteoporosis between the type of ICS or other bronchodilating inhalers that were used (fluticasone/salmeterol: hazard ratio [HR], 1.404; p=0.169; budesonide/formoterol: HR, 0.735; p=0.272; tiotropium bromide: HR, 1.533; p=0.068; p=0.492). Moreover, in multivariate linear regression, ICS use was not associated with BMD significantly.
Discussion
In this study, we compared the prevalence of osteoporosis and BMD in patients with asthma, COPD, and ACOS. This study showed that osteoporosis tended to be more prevalent in patients with ACOS than in those with asthma, and BMD (L1–4 mean) was more significantly associated with a diagnosis (ACOS vs. asthma) regardless of ICS use.
This study is to demonstrate the prevalence of osteoporosis among patients with ACOS.
Although the definition and pathogenesis of ACOS remain unclear, there has been a recent emphasis on distinguishing ACOS from asthma or COPD since patients with ACOS present with more exacerbations and have a poorer quality of life and prognosis than do patients with either asthma or COPD8910. Thus, it is necessary to perform further studies regarding the etiology of complications that result in progressive functional decline and poorer overlap syndrome outcomes. Recent clinical trials have shown that increased levels of sputum neutrophil gelatinase-associated lipocalin (NGAL) are significant in patients with ACOS compared to those with COPD12, and that interleukin (IL)-6 is an important inflammatory mediator associated with ACOS among elderly people13. Chronic inflammatory lung disease itself can be a risk factor for osteoporosis, and inflammatory mediators have a pivotal role in osteoporosis. It is well known that IL-6 and TNF-α act as stimulants of osteoclasts that cause bone resorption56. In addition, a recent study demonstrated that NGAL levels may predict a future risk of osteoporotic fracture14. Inflammatory markers that are highly expressed in patients with ACOS, such as NGAL and IL-6, may be attributed to osteoporosis progression. However, proper prevention and treatment can prevent patients from experiencing deteriorating osteoporosis and osteoporosis-related fractures1516. Thus, we recommend active screening for osteoporosis to prevent complications and improve quality of life, especially for patients with ACOS.
Recent study also demonstrated the higher prevalence of osteoporosis compared to COPD (odds ratio, 1.14; 95% confidence interval, 1.04–1.26)17. Our study also showed that BMD of ACOS had lower trend than that of COPD. Compared to recent study17, our study showed higher prevalence of osteoporosis because we selected patients who did bone densitometry and who are more prone to have lower BMD. However, we more specified ACOS definition and adjusted sex, ICS use, which could be a factors affecting BMD.
The influence of ICS on osteoporosis was difficult to interpretate because this was a retrospective cross-sectional study. Many factors, such as low body mass index, immobility, vitamin D deficiency, and glucocorticoid use, may contribute to the development of osteoporosis among patients with COPD1. Whether the use of ICS leads to osteoporosis remains controversial, but other aspects of the disease may be linked more to the loss of BMD rather than to ICS use. Katsura and Kida7 found that osteoporosis was more common in cases of COPD than in asthma cases, even in the absence of steroid use. In the subgroup analysis of TOwards a Revolution in COPD Health (TORCH) study18, ICS therapy did not have a significant effect on BMD when compared to a placebo treatment. Furthermore, lung volume reduction surgery significantly improved BMD, even in patients requiring oral corticosteroids19, which emphasizes that the disease itself, rather than steroid use, may result in osteoporosis. Systemic inflammation cytokines rather than the use of ICSs play an important role in bone collagen synthesis inhibition and the stimulation of osteoclastic bone resorption in patients with chronic inflammatory airway disease7. This implies that the effects of ICS were less significant than were the effects of diagnosis and systemic inflammation associated with the diseases. Therefore, it is important to control systemic inflammation and disease activity to prevent osteoporosis. Thus, an appropriate use of ICS may reduce acute exacerbations and control inflammation, thereby leading to a reduction in systemic steroid use and a reduction in disease severity in ACOS patients20.
In this study, we also confirmed the risk factors for osteoporosis. BMD was negatively associated with CAT score among patients with ACOS and COPD. These results agree with those of a previous study21. The CAT score reflects pulmonary dysfunction, increased inflammatory load and decreased physical activity22. Patients with severe symptoms have a higher level of systemic inflammation and increased immobility, thereby exacerbating ongoing decreases in body mass and deficiencies in vitamin D, which results in a lower BMD2324252627. CAT might be higher in old age and in people with poor lung function28, but it was significantly associated with BMD even after excluding for other factors, such as age, sex, BMI, smoking, and ICS use. Other than respiratory and physical activity, the CAT score also includes activity limitations at home, confidence in one's ability to leave home, sleep, and level of energy, which was recently revealed to be associated with depression222930, which could be a risk factor for osteoporosis31. Thus, among patients with chronic inflammatory lung disease (especially COPD and ACOS), those with especially severe symptom score should be closely monitored for osteoporosis.
Although our study is strong because we have described the prevalence of osteoporosis in ACOS, it does have several limitations. First, this was a retrospective and cross-sectional study; therefore, there was a possible selection or referral bias. In our institute, we screened for osteoporosis in patients with a low BMI and old age, which is known risk factors of osteoporosis. The patients included in the study may have experienced more osteoporosis risk factors than other patients with chronic inflammatory airway diseases whose BMD scores were not measured. Moreover, fracture data collection was difficult in this study because it was not a longitudinal study, but rather a cross-sectional study. Second, inflammatory cytokine levels were not measured. To confirm the effects of inflammatory cytokines on patients with each disease, further studies focusing on inflammatory cytokines (e.g., TNF-α, IL-6, and NGAL) should be performed. Third, because the diagnostic criteria for ACOS is not yet well defined, ACOS could not be clearly distinguished. However, we used the criteria that Soler-Cataluna et al.11 have suggested to classify patients with ACOS. Although there were fewer patients with ACOS than with asthma or COPD, the results were significant.
In conclusion, our study demonstrates that osteoporosis is more prevalent in patients with ACOS than in those with asthma, and that the diagnosis of ACOS itself, rather than asthma, could be a risk factor for low BMD. Patients with ACOS, particularly aged and lean women, should be more carefully monitored for osteoporosis compared to patients with asthma. A large, well-characterized prospective study should be performed to confirm our findings.
 XML Download
XML Download