

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
As a macro indicator of the healthcare system, increased physical and mental health of students have been highlighted in the national health plan of the Fifth Economic, Social, and Cultural Development Program of Iran [1]. Natural growth is the most important health indicator in childhood and adolescence. Standard growth tables and graphs are used to assess the status of nutrition and growth of children and adolescents both individually and in groups [2].
Currently, in accordance with the national guidelines in Iran, all children should attend health assessment centers before entering school, so that all aspects of their health (including anthropometric indices) can be assessed, and health certificates can be issued for them [3]. In Iran, height-to-age and body mass index (BMI)–to-age indicators are the same as those proposed by the World Health Organization (WHO) in 2007, designed for 5–19-year-old children and adolescents in developing countries [4]. These indicators have been accepted by Iran's Ministry of Health as reference-and documented in students' health certificates.
In Asia, the problem of nutrition transition has been caused by increased urbanization, higher incomes, and the industrialization of societies. The combination of these factors has led to some changes in people's lifestyles and nutrition [5]. Being located in Asia, Iran is no exception and nutrition transition is also gathering momentum in this country. Unfortunately, we are novices in dealing with this issue [6]. Like many countries, nutrition transition has seriously imposed the burden of nutritional problems, such as stunting, overweight, obesity, and wasting concurrently in population groups, especially among children and adolescents [57]. Obesity and overweight in childhood and adolescence increase the risk of various diseases in adulthood including type 2 diabetes, metabolic syndrome, obesity, and cardiovascular diseases [6,8910]. Wasting in childhood and adolescence increases the risk of infectious diseases [1112]. Stunting or short stature in periods of growth also creates many problems such as future obesity and greater risk of cardiovascular diseases [131415].
Generally, the assessment of the trend of anthropometric indices in children and adolescents in each region can significantly help provide effective strategies to improve their growth [16]. The majority of studies conducted on the trend of children's and adolescents' development have focused on obesity and overweight and have mostly indicated the increasing prevalence of obesity and overweight among study groups [1718192021].
The present study aimed to determine the trend of anthropometric indices of students from primary school through high school in the west of Iran.
MATERIALS AND METHODS
Subjects
This longitudinal study was conducted in Kermanshah province which is located in the west of Iran. Sixteen out of 37 high schools were selected randomly using cluster sampling and 50 students were selected from each cluster. In total, 800 students participated in this study and the rest (69) were excluded due to lack of data. The trend of anthropometric indices of students was assessed from primary school (during 2003–2006) through high school (2014).
Assessment of anthropometric measurements
The data were collected using a demographic checklist, information from health certificates, and anthropometric measurements. The demographic variables contained questions on gender, date of birth, date of current assessment, and current weight and height. Other data including age, weight, and height at initial assessment in primary schools were obtained from the students' health certificates which were prepared during 2003–2006 (at 5–8 years of age. Body weight was measured by a scale with 0.5 kg accuracy without shoes and with light clothing. A tape with 0.5 cm accuracy was used to measure height without shoes (Seca stadiometer model 769). BMI was calculated by dividing weight (kg) by height2 (m).
Nutritional data relating to primary and high school stages were entered into a software called AnthroPlus. This software is designed by the WHO to calculate anthropometric indices. Based on the WHO growth standards, AnthroPlus defines nutritional disorders as the following [22]:
1. Obesity or overweight: BMI Z-SCORE for age ≥ +1, or any degree of excess weight
2. Wasting: BMI Z-SCORE for age ≥ −1, or any degree of wasting
3. Stunting: height Z-SCORE for age ≥ −1, or any degree of shortness
Statistical analysis
The data were analyzed by SPSS software (version 16; SPSS Inc., Chicago, IL, USA) and the results are expressed as means ± standard deviation (SD) for quantitative variables and qualitative variables as number and percentage. Lower than or higher than normal students were identified by the Z-score found for both sexes at 2 points in time. The paired t-test was used to compare overall Z-scores at 2 points in time for bothsexes. For all statistical tests, p value less than 0.05 was considered as significant.
Ethics approval and consent to participate
The study has been done under supervision of Kermanshah University of Medical Science. Written informed consent was obtained from each study participant at the beginning of measurement. Ethical review is not always be required for the secondary use of data collected from human participants.
RESULTS
Anthropometric indices of the study students from primary school to high school
The characteristics of the participants are summarized in Table 1. The sample consisted of 731 participants, 350 (47.9%) of which were female and 381 (52.1%) male students. The mean age of female students was 7.2 ± 0.9 years in the first assessment (primary school) and 15.8 ± 0.7 years in high school. Their mean BMI was 15.4 ± 2.0 kg/m2 in primary school and 21.9 ± 4.4 kg/m2 in high school. The mean age of male students was 7.1 ± 1.1 years in the first assessment (primary school) and 15.4 ± 2.1 years in high school. Their mean BMI was 15.4 ± 2.1 kg/m2 in primary school and 21.4 ± 4.2 kg/m2 in high school (Table 1).

Distribution of height for age index of the study students in comparison with the WHO index
The results showed that distribution of the height for age index of the whole students (n = 731) at the primary school point, did almost exactly match that of the WHO, but slightly shifted to the left side at the high school point. This trend was more evident among girls compared to boys (Figure 1).
 | Figure 1Comparing height for age of students in primary school and high school according to the WHO. p value of height for age for girls in primary school vs. WHO standard was 0.234 and in high school was > 0.001. p value of height for age for boys in primary school vs. WHO standard was 0.126 and in high school was > 0.001. p value of height for age for all students in primary school vs. WHO standard was 0.017 and in high school was > 0.001.WHO, World Health Organization.
|
Changes in students' anthropometric indices Z-score
In students as a whole, mean values of height for age Z-score significantly reduced from primary school to high school, and this downward trend was greater in girls compared to boys (Table 2).
Table 2
The mean (± SD) of anthropometric indices Z-score in study students

![]()
Prevalence of nutrition disorders in the study students
Prevalence of overweight or obesity increased from primary school to high school by 2.5 times, and it was more evident in boys in comparison to girls. On the other hand, prevalence of stunting in the study students increased from primary school to high school by 1.4 times but it was higher in girls than in boys (11% to 13.9% in boys' vs. 16% to 25.2% in girls). Also, the rate of wasting decreased from primary school to high school by two thirds, and it was greater in girls compared to boys (Table 3).
Table 3
Prevalence of nutrition disorders in study students

![]()
Distribution of the BMI for age index of the study students in comparison with the WHO index
When assessed as a whole, the distribution of BMI for age index during primary school years was slightly shifted to the left compared with that of WHO standard, but at high school, it moved to the right side, closer to the distribution of the WHO standard. This trend was much more evident in girls compared to boys (Figure 2).
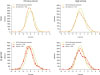 | Figure 2Students' BMI for age according to the WHO. p value of BMI Z-score to age for girls in primary school vs. WHO standard was 0.624 and in high school was > 0.001. p value of BMI Z-score to age for boys in primary school vs. WHO standard was 0.467 and in high school was > 0.001. p value of BMI Z-score to age for all students in primary school vs. WHO standard was 0.205 and in high school was > 0.001.BMI, body mass index; WHO, World Health Organization.
|
DISCUSSION
The results of the present study revealed a significant reduction in mean height for age Z-score, but substantial increases were observed in mean BMI for age Z-score in the study students from primary to high school in the west of Iran. The findings of this study indicate that the nutritional problems of students have increased from primary to high school, the gap with WHO growth standards has increased, and the changes in boys seemed more favorable than those in girls.
The growth charts of the students in the primary school were not significantly different from the WHO charts, whereas significant difference was found in high school students. In this study, prevalence of overweight or obesity increased by 2.5 times from primary school to high school. This increasing trend in obesity is in accordance with those found in the studies conducted in Brazil [17], UK [20], and Cypress [19] in children and adolescents.
In the present study, the trend of stunting increased from primary school to high school by 1.4 and the tangible increasing trend was greater in girls than in boys. The results of the present study, which indicated height to age index shifted to the left (compared with the WHO Child Growth Standards) and greater than the expected amount for the students in the 50th percentile are in line with the results obtained in previous studies conducted in this town [23]. There is few research on the trend of stunting, particularly observed in school aged children. A study conducted in the pre-school children in Peru reported a reducing trend of stunting from 1991 to 2011 [24]. Another study performed in children younger than 60 months in 148 developed and developing countries reported a reducing trend of stunting from 1990 to 2010, which indicated that it was still an important health concern in developing countries [25].
In our study, prevalence of wasting and overweight or obesity at high school point was 16.5% and 25.1%, respectively. In a study performed in Zabul, a province in eastern Iran, prevalence of underweight was reported as 18.7% and overweight or obesity as 16.3% [26]. Cultural, climate, and ethnic differences in the study groups seem to cause the differences in the prevalence of underweight between our study and Salehi-Abargouei et al. [26] (Baluch race in Zabul study and Kurd in the present. According to the study conducted in 6 ethnic groups (Fars, Turk, Kurd, Lor, and Arab ethnicities) in Iran, Baluch had the lowest BMI among the ethnicities [27].
The results of our study demonstrated that prevalence of wasting tends to decreasefrom primary school to high school, and was in the acceptable range in both primary and high schools. This result is consistent with the result by Sheikholeslam et al. [28], who reported that prevalence of malnutrition based on the WHO definition is lowest in Iran even among the countries with low prevalence. Hence, it may be asserted that a serious burden of nutrition problems exists among the participants of the current study which is similar to the studies conducted in Mexico [29], Bangladesh [30], India [31], Uruguay [32] and Iran [33]. This burden of nutritional diseases will impose a huge economic burden on the country in future, and will be seen in the form of management and treatment costs due to metabolic syndrome, cardiovascular diseases, and type 2 diabetes [59153435]. The overall findings of this study warn against nutrition transition in the study population, and we are unfortunately novices in dealing with this problem [6].
It seems that proportion of underweight students has slightly decreased because of improvement of primary health services such as vaccination programs, environmental health, public health and the control of infectious diseases [36]. On the other hand, prevalence of overweight and obesity in our study has increased due to the accelerated nutrition transition in Iran, and inappropriate nutritional patterns toward greater consumption of high-energy foods, as well as sedentary lifestyle [56]. Perhaps, the other reasons for the aggravating nutrition problems in Iranian primary and high school children are related to the health care covering age, for example, the initial coverage was the ages from birth to primary school entrance by health centers, the withdrawal of this monitoring was from the age of entering primary school, providing the last child healthcare was at the age of 8 when the child is involved in the school health programs, and the inappropriate quality of schools' screening programs appears to have a substantial share in the incidence of these issues.
As the prevalence of overweight or obesity in the students from primary school to high school has markedly increased prevalence of stunting has also increased in the same period. Therefore, we recommend that the Ministry of Health must seriously educate all age groups for optimal nutrition patterns through the national mass media to deal with these problems. Moreover, the Ministry of Sports and the Youth should take measures to acculturate regular physical activity as part of daily program for all. The Ministry of Health should also review the schools' health screening programs, so that they are performed appropriately and the sports teachers should also be involved in improving the quality of screening. These programs should move toward creating an electronic ID for every Iranian child in a way that all growth monitoring from birth until graduation is recorded in this electronic ID and interventions can be made when necessary.
The strength of the present study is in assessing a fixed population and also the assessment of their anthropometric indices at 2 points in time (primary and high school). This advantage has led to maintaining many of the factors affecting anthropometric indices to a large extent constantly including genetic differences, and parents' occupation and education [373839]. Since BMI is inversely and squarely associated with height, increased trend of obesity and overweight reported in the previous studies may be related to the increase in mild stunting. Considering the few studies on stunting trends worldwide as well as in Iran, further studies need to be carried out on this subject.
CONCLUSION
In the study students, prevalence of overweight or obesity has multiplied, markedly increased from primary school to high school, and that of stunting and underweight have also been increased during that period. Hence, it may be asserted that the study population is faced with nutrition transition, and health system policy-makers should design and implement a precise and effective plan for this situation.
 XML Download
XML Download