

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since its first introduction into clinical practice in 1993,1) transradial approach has been increasingly adopted for percutaneous coronary intervention (PCI) over the past two decades. Comparing with traditional transfemoral intervention (TFI), transradial intervention (TRI) has been shown to hold potential advantages of fewer access site-related bleeding and vascular complications and better patients' satisfaction.2)3)4)5)6)7)8) So far the safety and efficacy of TRI has been demonstrated in several specific patient populations, such as the elderly and the obesity.9)10)11)
Due to their high prevalence of coronary artery disease (CAD), women represent another large group of patients who will possibly benefit from PCI.12)13) However, they are often under-represented in clinical studies.14)15) Therefore, the role of TRI in women remains to be further defined. Using data from the Fuwai database, a single-center registry based on the largest heart center in People's Republic of China, we sought to examine the safety and efficacy of TRI in women in China.
METHODS
Study population
Our study population consisted of 5,067 women undergoing PCI at Fuwai Hospital, Beijing, China between 2006 and 2011. TRI was performed in 4,105 patients and 962 patients received TFI. Patients were prospectively followed up for around 1 year after discharge. The Institutional Review Board of Fuwai Hospital, Peking Union Medical College (approval number: 2016-847), approved the study and waived the requirement for informed consent.
Endpoint definition
The primary endpoint was major adverse cardiac events (MACEs) during hospitalization and at 1-year follow-up. It is a composite of cardiac death, myocardial infarction (MI), and target vessel revascularization (TVR). Secondary endpoints included each component of the primary endpoint, major bleeding, and access site complications.
Bleeding events were evaluated according to the Bleeding Academic Research Consortium (BARC) definition16) and major bleeding was defined as a bleeding event with BARC grade ≥3. Access site complications in our study included local hematoma that prolonged hospital stay, mediastinal hematoma, retroperitoneal hematoma, aneurysm, and arteriovenous fistula. Patients' baseline and procedural characteristics were obtained from medical record system and the catheterization laboratory's database. In-hospital outcomes were validated by medical record review. Follow-up was performed by trained staff at Fuwai Hospital via phone visits at 6 months and 1 year after discharge.
Statistical analysis
Continuous variables were expressed as mean±standard deviation and compared using Student's t-test. Categorical variables were described using frequencies and percentages and compared using chi-square test or Fisher's exact test, as appropriate. In-hospital and 1-year outcomes between TRI and TFI groups were analyzed by logistic and Cox regression respectively and were expressed as odds ratio (OR)/hazard ratio (HR) and 95% confidence interval (CI).
Since treatment decisions (TRI or TFI) in real-world practice is not made based on randomization, a 1:1 matched propensity score matching (PSM) was performed to control for potential biases. Propensity scores were calculated from a logistic regression model with access route as the dependent variable. Independent variables included age; prior history of MI, coronary artery bypass grafting (CABG) surgery, PCI, stroke, diabetes mellitus (DM), hypertension, or hyperlipidemia; clinical diagnosis; left ventricle ejection fraction (LVEF) before PCI; hemoglobin level before PCI; creatinine concentration before PCI; use of glycoprotein (GP) IIb/IIIa inhibitors; use of low molecular weight heparin; single-, double-,or triple-vessel lesion; left main disease; lesion type (de novo, intrastent, or restenosis); lesion location (ostial or bifurcation lesion); chronic total occlusion; number of treated lesion; number of stents used; use of drug-eluting stents (DESs). The caliper was set as 0.02. In the end 899 pairs were matched and the C-statistics for the propensity score model was 0.63. Paired t-test for continuous variables and paired χ2 test or Fisher exact test for categorical variables were then performed within the matched patients. Data were analyzed according to intention-to-treat principle (before the potential crossover). All statistical analyses were performed using IBM SPSS Software, version 22.0 (IBM Corp., Armonk, NY, USA) and a 2-sided p<0.05 was considered significant.
RESULTS
Baseline and procedural characteristics of women undergoing TRI and TFI are shown in Tables 1 and 2. Compared with TFI, TRI patients were slightly younger; had lower prevalence of prior MI, CABG, or PCI; higher prevalence of DM; less likely to present with ST-segment elevated MI; and were more likely to have stable angina. They were also more likely to undergo PCI for single or double-vessel lesions and were less likely to receive the procedure for triple-vessel lesions, left main diseases, or ostial lesions. TRI group were also noted to have a shorter average total procedure time. After PSM, all characteristics were well-balanced between TRI and TFI patients.
Table 1
Baseline characteristics of women undergoing TRI and TFI
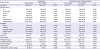
Dara shown are number (%) or mean±SD.
CABG = coronary arterial bypass grafting; DM = diabetes mellitus; GP = glycoprotein; LMWH = low molecular weight heparin; LVEF = left ventricle ejection fraction; MI = myocardial infarction; NSTEMI = non-ST-segment elevation myocardial infarction; PCI = percutaneous coronary intervention; TFI = transfemoral intervention; TRI = transradial intervention; SD = standard deviation; STEMI, ST-segment elevation myocardial infarction.
Table 2
Angiographic and procedural characteristics of women undergoing TRI and TFI
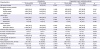
Sixty-nine patients (1.7%) had failed TRI procedure and were converted to TFI. No patients in the TFI group were crossed over to the TRI group. A vascular closure device was used in 388 (40.3%) patients in the TFI group.
Bleeding and complications from PCI are shown in Table 3. The incidence rates for BARC ≥2 (8.5% vs. 18.7%, p<0.001) and BARC ≥3 (0.9% vs. 3.2%, p<0.001) post-PCI bleeding were significantly lower in the TRI group than the TFI group. Both access-site-related (0.6% vs. 2.1%, p<0.001) and non-access-site-related (0.3% vs. 1.1%, p=0.002) major bleeding were less frequently observed among TRI patients. Moreover, TRI group had significantly fewer access site complications (8.9% vs. 19.5%, p<0.001), which was mainly due to a lower rate of local hematoma that prolonged hospitalization (8.7% vs. 18.5%, p<0.001). In propensity score-matched patients, all these differences remained significant (BARC ≥2: 8.5% vs. 18.7%, p<0.001; BARC ≥3: 1.0% vs. 3.4%, p<0.001; and access site complications: 8.8% vs. 19.9%, p<0.001, respectively) (Figure 1).
Table 3
Bleeding and complications of women undergoing TRI and TFI
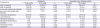
Figure 1
Comparison of bleeding and access site complication between TRI and TFI groups in propensity score-matched patients.
BARC = Bleeding Academic Research Consortium; TFI = transfemoral intervention; TRI = transradial intervention.

In-hospital outcomes are shown in Table 4. The rates of MACE, MI, and TVR were similar in the 2 groups both before and after PSM. Cardiac death was less frequently observed among TRI patients (0.1% vs. 0.5%, p=0.016) but this did not remain significant in propensity score-matched patients. Logistic regression analysis showed that TRI was an independent predictor of reduced in-hospital major bleeding (OR, 0.64; 95% CI, 0.54–0.76; p<0.001) and access site complications (OR, 0.67; 95% CI, 0.61–0.74; p<0.001).
Table 4
In-hospital and 1-year outcomes of women undergoing TRI and TFI
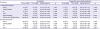
Follow-up work was completed in all patients with a median follow-up time of 361 days (interquartile range [IQR], 354–366 days) and 360 days (IQR, 354–366 days) in TRI and TFI groups respectively. The Kaplan-Meier curves for 1-year outcomes in propensity score-matched patients are shown in Figure 2. Incidence rates of 1-year MACE and its components tended to be lower in TRI group, but this did not reach statistical significance (p>0.05; Table 4).
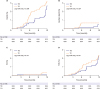
Figure 2
Kaplan-Meier curves for occurrence of MACE (A), cardiac death (B), MI (C), and TVR (D) between TRI and TFI groups of 1-year follow-up in propensity score-matched patients.
MACE = major adverse cardiac event; MI = myocardial infarction; TFI = transfemoral intervention; TRI = transradial intervention; TVR = target vessel revascularization.
DISCUSSION
The present study represents a large cohort of women undergoing PCI in real world clinical practice. We found that TRI was associated with significantly reduced in-hospital major bleeding and access site complications. Although TRI was more likely to be performed in patients with lower risk, such significance persisted after controlling for potential biases using PSM. Our findings demonstrate the safety and efficacy of TRI in women and add evidence to promote more widespread adoption of TRI in female patients.
Transradial approach has become the primary approach for PCI in China.17) Due to advantages in safety, efficacy, and patients' satisfaction, it has been widely adopted in clinical practice.2)3)4)5)6)7)8) However, most of the evidences came from studies conducted in both genders, in which women are often under-represented.14)15) As for women themselves, they are at higher risk of adverse events after CADs and PCI.13) Performing TRI in women is considered more technically demanding because of smaller caliber radial arteries than men and increased rate of vasospasms, which could lead to procedure failure and worse outcomes.18) Thus, it is reasonable to believe that women may respond to treatment strategies differently than men, and the safety and efficacy of TRI in women should be evaluated separately. However, only a few studies have compared TRI with TFI in female patients so far.18)19)20)21)
Bleeding has been recognized as a strong predictor of worst outcomes after PCI.22) Several bleeding avoidance strategies have been suggested to improve safety of the procedure, including pharmacological, technological, and procedural approaches.23) As one of the major procedural approaches, TRI has been shown to reduce bleeding by both randomized3)5)6) and observational8)19)24)25) studies. Since radial arteries are superficial and readily compressible, TRI is also believed to reduce bleeding in women.26) The Radial Vs femorAL access for coronary intervention (RIVAL) trial is the largest randomized TRI versus TFI study up to date.3) Results of its subgroup analysis of women demonstrated that radial access was effective in reducing bleeding complications.18 The Study of Access Site for Enhancement of PCI (SAFE-PCI) for Women trial21) represents the first randomized trial of TRI versus TFI performed solely in women. Although the trial was terminated early due to lower than expected rates of endpoint events, there was still a trend of fewer bleeding in women undergoing TRI. Other observational retrospective analyses also came up with similar results, suggesting that women undergoing TRI was less likely to suffer from major BARC bleeding events.19)20) Consistent with previous studies, we found that TRI was associated with reduced major post-PCI bleeding (OR, 0.64; 95% CI, 0.54–0.76; p<0.001). Our findings support the safety of TRI and suggest that its wider adoption could lead to improved outcomes in women.
Lower risk of access site complications is considered another major benefit of TRI.4) However, as stated above, most of the studies supporting this idea were conducted in whole populations, a large proportion of which were men. Previous analyses have shown that the rates of access site vascular complications were higher in women than in men.3)18) Randomized studies, including the SAFE-PCI trial and gender-specific sub-analysis of the RIVAL trial, suggested that safety of catheterization was improved by transradial approach in women, with significantly fewer access site vascular complications.18)21) As for observational data, the retrospective study by Kedev et al.20) also reported that TRI was associated with less vascular complications than traditional TFI. Our study demonstrated that TRI group had significantly fewer access site complications both before and after PSM adjustments (all patients: 8.9% vs. 19.5%, p<0.001; propensity score-matched patients: 8.8% vs. 19.9%, p<0.001). Transradial approach was also identified as an independent predictor of reduced access site complications (OR, 0.67; 95% CI, 0.61–0.74; p<0.001). Thus, TRI seems to be effective in reducing access site complications in women.
Several limitations of this study should also be acknowledged. First of all, it was a retrospective observational analysis, which was limited by its nonrandomized nature. Although a 1:1 matched PSM was performed to control for potential biases, this was still not an acceptable substitute for randomization. Second, since our study was based on retrospective data, it is possible that the incidence rates of events were underestimated. This could explain the low rate of MACE in our study. Third, the potential advantages of TRI in women are likely to depend on operator's experience.27) Researchers from both the RIVAL trial and SAFE-PCI trial have suggested that TRI was shown to be superior to TFI only if performed by experienced operators and therefore its advantages might not be applicable to those who are novice in transradial approach.3)18)21) Moreover, our study only include data from a single center where TRI dominates. Importantly, operators' experience and training with transradial approach may differ from site to site. Thus, the generalizability of our findings to other less-experienced centers remains to be further defined.
In conclusion, in this large propensity score-based single center comparison of TRI versus TFI in women, TRI showed advantages of safety and feasibility over TFI, with significant reduction in major post-PCI bleeding and access site complications. A widespread adoption of TRI in women has the potential to improve outcomes in treatment of CADs.
 XML Download
XML Download