

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The mortality rate of acute myocardial infarction (AMI) patients having a complication of cardiogenic shock is still high, despite advances in reperfusion therapy with mechanical circulatory support (MCS).1)2)3)4)5) Because AMI with cardiogenic shock is occasionally accompanied by cardiac arrest, cardiopulmonary resuscitation (CPR) is warranted.4) Extracorporeal membrane oxygenation (ECMO) is an MCS device and is increasingly used for maintaining hemodynamic support in cardiogenic shock, especially during primary percutaneous coronary intervention (PCI).6)7)8)9) CPR is a poor independent predictor of in-hospital mortality in patients with AMI and a complication of cardiogenic shock, despite ECMO support.10) Nevertheless, there were some reports that ECMO-assisted CPR (E-CPR) showed a superior survival benefit over conventional CPR (C-CPR) in patients who experienced in-hospital cardiac arrest.11)12) However, with regard to ECMO-assisted primary PCI procedure performed to treat AMI patients having a complication of cardiogenic shock, there is no available data on the relationship between clinical outcome and CPR time. Therefore, here, we investigated the clinical outcomes of and impact of CPR time on patients with AMI complicated with cardiogenic shock and who were treated by ECMO-assisted primary PCI.
METHODS
Study population
In this study, 82 patients from the Dankook University Hospital ECMO registry were analyzed. From July 2008 to March 2016, we analyzed 42 patients with AMI with cardiogenic shock who underwent CPR and who were treated using the ECMO system (Figure 1). The major inclusion criteria were AMI with cardiogenic shock patients who underwent CPR and required ECMO support as well as visited catheterization laboratory room to receive primary PCI. Exclusion criteria include unwitnessed cardiac arrest, definite non-cardiogenic arrest, no return of spontaneous circulation (ROSC) after CPR, irreversible organ failure when ECMO is not expected to be beneficial (hepatic failure, late stage of adult respiratory distress syndrome, etc.), and patients eligible for “do-not-resuscitate” status. This study was approved by the Institutional Review Board in Dankook University Hospital (approval number: 2018-05-004).
Definition and data collection
Based on the third universal definition of AMI implemented by a joint task force from the European Society of Cardiology (ESC), American College of Cardiology (ACC) Foundation, American Heart Association (AHA), and the World Heart Federation (WHF) in 2012, AMI was diagnosed. We included the type I AMI by clinical classification.13) Cardiogenic shock was defined by signs of tissue hypoperfusion, such as clammy and cool peripheries, prolonged capillary refill times, altered mental status, oliguria, pulmonary congestion, tachycardia, elevated lactate, or mixed venous saturation of <65%. Hemodynamic criteria for cardiogenic shock included a systolic pressure of <90 mmHg for more than 30 minutes, despite maximal medical treatments for the correction of hypovolemia, hypoxemia, and acidosis. CPR included both intermittent and persistent CPR. Total CPR time was defined as the interval between compression initiation and ROSC. CPR time summed the time of all actions related to CPR. CPR-ECMO time was defined as the interval between CPR initiation and ECMO application. Successful revascularization was defined when residual stenosis was <20% with thrombolysis in myocardial infarction (TIMI) III flow in all intervened lesions. The primary outcome was 30-day in-hospital mortality after primary PCI. To determine the predictors of 30-day in-hospital mortality, we collected clinical, angiographic, procedural, and outcome-related data from hospital medical records.
ECMO management
In this study, Capiox Emergency Bypass System (Capiox EBS™; Terumo Inc., Tokyo, Japan) was used as the ECMO system. This system consisted of an extracorporeal life controller including a back-up battery and a disposable bypass circuit integrated with a heparin-coated membrane oxygenator and a centrifugal pump. The device was implanted onto the femoral artery and vein by percutaneous cannulation using the Seldinger technique. The tip of the arterial cannula was positioned in the common iliac artery and the tip of the venous cannula was placed at the junction of the right atrium and the superior vena cava. Anticoagulation was achieved by administering a bolus injection of unfractionated heparin and maintaining an activated clotting time between 180 and 220 seconds with a continuous intravenous infusion of unfractionated heparin. The initial flow rate of ECMO was 2.2 L/min/m2, which was subsequently regulated to maintain a mean arterial pressure of 65 mmHg. ECMO weaning was considered when the patient was hemodynamically stable and properly oxygenated and when ECMO flow rate was <1 L/min/m2 for 4 hours. Successful weaning was defined as removal of ECMO support without reinsertion or death within 24 hours.
Statistical analysis
Continuous variables were presented as mean±standard deviation or median with interquartile ranges. Continuous variables were compared using Student's t-test or Mann-Whitney U test. Categorical variables were expressed as percentages and compared using the χ2 test or Fisher's exact test. Event-free survival curves were plotted using the Kaplan-Meier method and compared using the log-rank test. The predictive value of CPR time to predict mortality was analyzed using receiver operating characteristic (ROC) curves, in which the best cut-off value corresponded with the value with the greatest accuracy (sensitivity + specificity). Univariate and multivariate Cox proportional hazard regression analysis was conducted to determine the predictors of in-hospital mortality. Covariates that were statistically significant in univariate analysis results and those considered clinically relevant were included in the multivariate models. All statistical analyses were two-tailed, with clinical significance defined at a p value of <0.05. All statistical analyses were conducted using statistical package for social science (SPSS 20.0 for Windows; SPSS Inc., Chicago, IL, USA) software.
RESULTS
Baseline characteristics
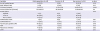
The baseline characteristics for comparison between the survivor group (n=8) and the non-survivor group (n=34) are shown in Table 1. There were no significant differences in demographics or co-morbidities between the 2 groups.
Table 1
Baseline characteristics

Laboratory and procedural findings
The survivor group showed a significantly higher initial pH compared with the non-survivor group. There was no difference in cardiac enzyme levels between the 2 groups. Door-to-balloon time in the survivor group was shorter than that in the non-survivor group (74.63±29.8 vs. 132.09±109.32 minutes, p=0.03, respectively). Most patients had multi-vessel disease, but there was no significant difference between in the number of patients between the 2 groups. The major culprit artery was the left anterior descending artery (LAD). The revascularization rate of only the culprit artery was 64.3%, however, there was no difference in this rate between the 2 groups (Table 2).
Table 2
Laboratory and procedural data

Data expressed as number (%) or mean±standard deviation.
CK-MB = creatine kinase-myocardial band; CTO = chronic total occlusion; LAD = left anterior descending artery; LCA = left coronary artery; LCx = left circumflex artery; LMCA = left main coronary artery; NT-proBNP = N-terminal pro B-type natriuretic peptide; RCA = right coronary artery; tCO2 = total carbon dioxide; TIMI = thrombolysis in myocardial infarction.
CPR- and ECMO-related findings
CPR time was significantly longer in the non-survivor group than in the survivor group (43.06±38.72 vs. 11.25±12.08 minutes, p=0.028, respectively). Out-of-hospital cardiac arrest rate was higher in the non-survivor group than in the survivor group, but this difference was statistically insignificant. There was no patient who were applied ECMO before cardiac arrest in the survivor group. Only 1 patient (3.2%) was applied ECMO before cardiac arrest in non-survivor group. ECMO application before PCI was not significantly different between the 2 groups (3 [37.5%] vs. 8 [26.7%], p=0.55). During CPR, the presenting cardiac rhythm was asystole in 3 patients (7.1%), pulseless electrical activity (PEA) in 14 patients (33.3%), and ventricular tachycardia or fibrillation in 25 patients (33.3%) (Table 3).
Table 3
CPR- and ECMO-related data
Data expressed as number (%) or mean±standard deviation.
CPR = cardiopulmonary resuscitation; CRRT = continuous renal replacement therapy; ECMO = extracorporeal membrane oxygenation; IABP = intra-aortic balloon pumping; PCI = percutaneous coronary intervention; PEA = pulseless electrical activity; ROSC = return of spontaneous circulation; VF = ventricular fibrillation; VT = ventricular tachycardia.
ROC curve analysis
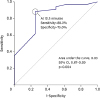
ROC curve analysis was performed to define an optimal cut-off CPR time value to predict in-hospital mortality in patients with AMI and a complication of cardiogenic shock who were treated by ECMO-assisted primary PCI. The area under the curve was 0.83 (95% confidence interval [CI], 0.67–0.99; p=0.004), and the greatest accuracy in the differentiation of mortality outcome was obtained at a cut-off of 12.5 minutes (88.2% sensitivity and 75% specificity; Figure 2). There was no significant difference demographics, laboratory, and procedural findings between CPR ≤12.5 minutes group (n=10) and CPR >12.5 minutes group (n=32) (Supplementary Tables 1, 2, 3).
Clinical outcomes
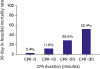
Thirty-day in-hospital mortality rate was observed for a total of 33 (78.6%) in our study. During the follow-up period (128.9±413.8 days), mortality rate was observed for total of 34 (81%). Seventeen (29.3%) patients could be weaned from ECMO. Multivariate analysis revealed that CPR time of >12.5 minutes was an independent predictor of 30-day in-hospital mortality outcome (adjusted hazard ratio, 4.66; 95% CI, 1.06–20.5; p=0.042; Table 4). Mortality rate was 2.4% in patients (n=1) who received CPR for <5 minutes, and they were 11.9%, 28.6%, and 52.4% in patients who received CPR for <15 (n=5), <20 (n=12), and <30 (n=22) minutes, respectively (Figure 3). Kaplan-Meier curves demonstrated that the mortality rate was significantly higher in patients who received CPR for a longer duration of >12.5 minutes (30-day mortality rate: 30% vs. 93.7%, p=0.001; Figure 4).
Table 4
Independent predictors for 30-day survival by multivariate Cox regression analysis


DISCUSSION
The following are the main findings of our study. 1) Despite ECMO support, the clinical outcomes of AMI patients having a complication of cardiogenic shock remain poor. 2) Longer CPR time is associated with a poor prognosis of AMI patients treated by ECMO-assisted primary PCI.
The cardiogenic shock complicates 7–10% of AMI cases and is associated with a 70–80% mortality rate.1) Although early primary PCI was performed in these patients, short- and long-term mortality rates were still high at >45%.14)-16) Various types of MCS have been used for overcoming the high mortality of AMI complicated by cardiogenic shock. However, intra-aortic balloon pumping (IABP) did not reduce the 12-month all-cause mortality in IABP-Shock II randomized control trial.5) Recently, the use of ECMO in treating various causes of cardiogenic shock has considerably increased. Sheu et al.17) reported that early ECMO-assisted primary PCI improved 30-day clinical outcomes of AMI patients who experienced a complication of profound cardiogenic shock. Despite this effort, a recent study reported that the 30-day mortality in patients who received a combination of ECMO support and intra-arrest PCI was 71%.6) Consistent with this finding, our data revealed an overall 30-day mortality rate of 74.1%. Although ECMO provided hemodynamic stability, the prognosis of patients remains poor because of cardiogenic shock accompanied by cardiopulmonary collapse that not only may reduce coronary perfusion but also result in multiple organ failure.
Nevertheless, E-CPR resulted in better clinical outcomes than C-CPR in patients with cardiac arrest in previous studies.11)12) Shin et al.12) reported that E-CPR showed a beneficial effect with regard to neurologically intact survival as opposed to C-CPR performed for >10 minutes after an in-hospital witnessed cardiac arrest. Chen et al.11) reported that E-CPR had both short- and long-term survival benefits compared with C-CPR for patients who had an in-hospital cardiac arrest of cardiac origin; longer CPR duration was associated with poor prognosis. Most studies of C-CPR showed that a CPR duration of >20 minutes resulted in a survival rate of <5%.18)19) Some studies reported that the predictive value of E-CPR timing for predicting in-hospital mortality ranged between 30.5 and 60 minutes.20)21) In our study, the greatest accuracy in differentiating mortality outcomes was achieved at an E-CPR time of 12.5 minutes, which was shorter than the cut-off time value reported in other studies. Although other studies included cardiac arrest from other causes, our study was only based on patients who received primary PCI during a cardiac arrest caused by AMI complicated with cardiogenic shock. CPR is frequently performed due to fatal ventricular arrhythmia or PEA occurring during primary PCI in AMI patients who experienced cardiogenic shock. Therefore, this study demonstrated the relationship between CPR duration and clinical outcome in primary PCI.
In previous studies, no standard MCS timing has been established for treating AMI patients with cardiogenic shock. Current research focuses on relatively early hemodynamic support to break the adverse cycle, thereby lowering the need for an increased concentration of inotropes. The recent cVAD/Impella registry revealed that insertion of the new MCS (Impella) before PCI led to a significantly better clinical outcome than the use of inotropes alone or the IABP technique.22) Na et al.23) suggested that the initiation of ECMO support should be considered in selected cardiogenic shock patients with a vasoactive inotropic score of >85. In our study, the rates of ECMO support initiation before cardiac arrest and of PCI were 6.9% and 24.1%, respectively. However, our data revealed no survival benefits of early ECMO insertion. Nevertheless, since subjecting patients with AMI and cardiogenic shock to CPR is directly linked to a fatal prognosis, administration of MCS to such patients as soon as possible is an important treatment option. Considering that the time required by an experienced team for priming ECMO circuits is approximately 15–20 minutes, if CPR is carried out during primary PCI, application of ECMO as soon as possible would facilitate better clinical outcomes. In this regard, the relationship between CPR duration and clinical outcomes presented in our study results indicate a need for early MCS in AMI patients who experienced cardiogenic shock.
This study has several limitations. First, this is a retrospective observational study of a small sample size. Second, we only calculated the CPR time with regard to in-hospital cardiac arrest, and we were unable to estimate the exact CPR time in out-of-hospital cardiac arrest patients. Third, variations in CPR methods and intensities across cases affected the prognosis of patients. However, this study demonstrated that a short duration of CPR was important to improve the survival of patients who had AMI complicated with cardiogenic shock while undergoing PCI.
In conclusion, despite ECMO support, the clinical outcomes of patients with AMI complicated with cardiogenic shock remain poor. A CPR time of >12.5 minutes in-hospital is associated with poor prognosis in such patients receiving ECMO-assisted primary PCI.
 XML Download
XML Download