

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Neoadjuvant chemotherapy (NAC) followed by surgical cytoreduction is a feasible approach for patients with advanced ovarian cancer. Previous reports of retrospective and non-randomized prospective studies [1234] have demonstrated non-inferior survival with reduced serious morbidity in NAC-treated patients. Overall survival (OS) inversely correlates with residual tumor size or residual disease (RD) after primary debulking surgery (PDS) [5]. Moreover, RD is a significant prognostic factor in NAC-treated patients [6]. There is no significant difference in survival between patients treated with NAC or PDS who underwent complete surgery (no RD). However, compared to PDS, NAC is associated with reduced OS in patients both with stage IIIC and RD with <1.0 cm residual tumor size (RD<1.0 cm) [7]. Onda and Yoshikawa [1] suggested that the definition of optimal debulking in interval debulking surgery (IDS) should be more stringent than in PDS.
Intraoperative surgical assessment with direct visualization and palpation is currently the standard procedure for evaluating RD in patients with ovarian cancer who have undergone PDS or IDS. Determination by visualization and palpation can be influenced by various factors (e.g., the surgeon's experience, adequate evaluation of tumor sites, and surgeon and patient expectations) [891011].
Peritoneal washing cytology (PWC) is an indicator of ovarian surface involvement and peritoneal dissemination in ovarian cancer. Therefore, PWC provides valuable information on staging and prognosis, as shown in clinical guidelines [1213]. The PWC during IDS may overcome the limitations of micrographic evaluation of RD, which can be easily implemented into standard surgical procedures. Although one study by Nagasaka et al. [14] reported that PWC during IDS is associated with progression-free survival (PFS) in patients with advanced ovarian cancer, the efficacy of PWC during IDS and its effects on OS has not yet been determined. Therefore, the aim of this study was to evaluate the efficacy of PWC during IDS in relation to OS.
MATERIALS AND METHODS
1. Patients and study design
This study was conducted in accordance with the Declaration of Helsinki and the Reporting Recommendations for Tumor Marker Prognostic Studies of the National Cancer Institute. The retrospective design was approved by the Institutional Review Board of Kanagawa Cancer Center (Yokohama, Japan; 28-EKI-58). All study participants provided written informed consent. Patients with a diagnosis of primary ovarian cancer who were receiving treatment with NAC at our institution between January 1, 2011 and December 31, 2015 were identified. The median followed-up period for patients was 18.5 (0–67) months.
2. Diagnosis and treatment
An ovarian cancer diagnosis of adenocarcinoma was made by exploratory laparotomy (EL) or peritoneal cytology along with imaging findings and tumor markers. Patients who had received NAC at our institution, but had undergone an EL elsewhere, were included in this study. Patients with co-existing double primary cancers were excluded. Standard chemotherapy was administered as NAC followed by IDS. The chemotherapy regimens were primarily taxane- and platinum-based combinations. The baseline was the date of NAC initiation. The decision to perform IDS was made by the status of primary tumor and metastases as assessed with imaging and/or changes in serum cancer antigen 125 (CA125) levels. The patients who showed complete response or partial response, in accordance with the modified Response Evaluation Criteria In Solid Tumors (RECIST) criteria, after NAC, underwent IDS as they were expected to achieve optimal cytoreductive surgery. Those who presented with a negative conversion or decreasing levels of CA125 in response to NAC were also selected as IDS. Patients who had progressive disease were ineligible for IDS (non-IDS group).
Surgical procedures were performed to achieve optimal cytoreduction. At laparotomy for IDS, free abdominal fluid was aspirated, provided there were ascites in the Douglas' pouch before intraperitoneal observation. In the absence of ascites, peritoneal washing of the Douglas' pouch was performed with 50.0 mL of saline and the fluid was collected for PWC. Direct visualization and palpation of the peritoneum of the colon, intestine, diaphragm, and Douglas' pouch was performed after washing and aspiration. The standard procedure for IDS in patients with ovarian cancer includes a total abdominal hysterectomy, bilateral salpingo-oophorectomy, and omentectomy, with debulking surgery performed to minimize the RD, if metastases were present. Completion of IDS indicates completion of the standard procedure for IDS. Pelvic and para-aortic lymph node dissection was not performed except for 2 patients who were clinically diagnosed with massive swelling of lymph nodes. Optimal cytoreduction was defined as no RD≥1.0 cm in the largest diameter at the completion of IDS.
Intraoperative complications were defined as urinary tract injury, neural injury, vascular injury, or bowel injury. Perioperative complications included thromboembolic disease, gastrointestinal/urinary anastomotic leaks, ileus, wound infections, wound dehiscence, fever on the third postoperative day or later, cystitis, atelectasis, unplanned return to the operating room, readmission, or death within 30 days of the initial surgery.
3. Statistical analyses
Patient demographic and clinical characteristics were compared using the χ2 test or Student's t-test. Survival curves were plotted using the Kaplan-Meier method and compared using the log-rank test. Multivariate analyses were performed using a Cox proportional hazards model with stepwise selection. OS was measured from the date of NAC initiation to the date of death, with surviving patients censored at the date of last contact. PFS was measured from the date of initial diagnosis to the date of progression or death, whichever occurred first. Patients were followed on a regular basis using physical, serological, or radiological examinations, based on National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology, Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Cancer (version 2, 2013), and came to the hospital at times when they experienced symptoms. Progression of disease was diagnosed by contrast computed tomography (CT) or magnetic resonance imaging (MRI) using modified RECIST criteria (version 1.1). Patients were stratified into PWC-negative, PWC-positive, and non-IDS groups. Patients were also stratified according to serum CA125 levels of < or ≥75.0 IU/mL before IDS. Statistical differences were considered significant when the 2-sided p-value was less than 0.05. All statistical analyses were conducted using Statistical Package for the Social Sciences for Windows, software version 24.0 (IBM Corp., Armonk, NY, USA).
RESULTS
1. Patient demographic and clinical characteristics
In total, 164 patients diagnosed with ovarian cancer were analyzed in this study, including 64 patients who had received NAC. Among them, 17 patients (26.6%) who underwent an EL had biopsy proven ovarian cancer. The remaining 47 patients (73.4%) had cytology showing adenocarcinoma and CT findings consistent with primary ovarian cancer.
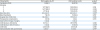
The demographic and clinical characteristics of the patients in the PWC-positive, PWC-negative, and non-IDS groups are summarized in Table 1. Patients treated with NAC had stage III–IV disease. In addition, IDS was performed in 78.1% of NAC-treated patients. Seventeen patients (26.6%) were PWC-negative and 33 patients (51.6%) were PWC-positive. Fourteen patients (21.9%) were in the non-IDS group. Fifty-nine of the 64 ovarian tumors were surface epithelial ovarian cancer. The demographic and clinical characteristics of the 3 groups did not differ significantly, except for histology.
Table 1
Demographic and clinical characteristics of patients with ovarian cancer who had received NAC between 2011 and 2015

2. Surgical parameters and complications
The perioperative parameters and postoperative complications of IDS in the PWC-negative and PWC-positive groups are shown in Table 2. The characteristics of the 2 groups did not differ significantly. Optimal debulking (RD<1.0 cm) was achieved in 72.0% of patients (n=36) and complete cytoreduction (no RD or without macroscopically residual tumors; RD=0) was achieved in 48.0% of patients (n=24). The largest RD was ≥2.0 cm in diameter in 24.0% of patients after IDS (n=12), and this was significantly associated with the PWC-positive group (p<0.05).
Table 2
Perioperative parameters and postoperative complications of IDS following NAC in patients with positive and negative PWC
Data are shown as number (%) or mean±standard error.
CA125, cancer antigen 125; IDS, interval debulking surgery; NAC, neoadjuvant chemotherapy; PWC, peritoneal washing cytology; RD, residual disease.
*Fisher's exact test or Student's t-test; †p<0.05; ‡Interval between the date of commencing NAC and the date of IDS.
Intraoperative complications were not detected in patients who had undergone IDS. Postoperative complications in the PWC-negative group included a transient abnormality in hepatic function, a urinary tract infection, and an abscess that required surgery in 1 patient each. In the PWC-positive group, 1 patient experienced cholecystitis. Blood loss was significantly lower in the PWC-negative group than in the PWC-positive group (p<0.01).
3. Survival analyses
The median OS of patients in the PWC-negative, PWC-positive, and non-IDS groups was 47, 18, and 5 months, respectively (Fig. 1A). Significant differences were observed between the PWC-negative and PWC-positive (Mantel-Cox log-rank test, p<0.01), PWC-negative and non-IDS (p<0.001), and PWC-positive and non-IDS (p<0.001) groups. The median OS of patients in the IDS (PWC-negative and PWC-positive groups) and non-IDS groups was 27 and 5 months, respectively (p<0.001). The median PFS of patients in the PWC-negative, PWC-positive, and non-IDS groups was 17, 13, and 5 months, respectively (Fig. 1B). Significant differences were observed between the PWC-negative and PWC-positive (p<0.01), PWC-negative and non-IDS (p<0.001), and PWC-positive and non-IDS (p<0.01) groups.
Fig. 1
Kaplan-Meier curves of (A) OS and (B) PFS in patients with ovarian cancer. Kaplan-Meier curves of OS in patients with (C) stage III and (D) stage IV disease.
IDS, interval debulking surgery; NAC, neoadjuvant chemotherapy; OS, overall survival; PFS, progression-free survival; PWC, peritoneal washing cytology.
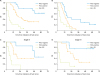
The PWC-positivity in IDS correlated with RD>2.0 cm (p<0.05), but not RD>1.0 cm (p>0.05) or RD=0 (p>0.05). Within the optimal debulking group (RD<1.0 cm), the median OS was 47 and 18 months for PWC-negative and PWC-positive patients, respectively (p<0.05) (Fig. 2A). Within the complete resection group (RD=0), the median OS was 55 and 29 months for PWC-negative and PWC-positive patients, respectively (p<0.05) (Fig. 2B). The median OS of patients with stage III (Fig. 1C) and stage IV (Fig. 1D) disease was 16.5 and 21 months, respectively. This difference was not significantly different. However, within each stage, a significant difference was observed between the PWC-negative, PWC-positive, and non-IDS groups.
Fig. 2
Kaplan-Meier curves of OS according to RD status. (A) <1 and (B) 0 in patients with negative vs. positive PWC.
NAC, neoadjuvant chemotherapy; OS, overall survival; PWC, peritoneal washing cytology; RD, residual disease.
*p<0.05.

The operative time for IDS was not significantly shorter in the PWC-negative group. However, the blood loss volume was significantly lower in this group (p<0.05).
4. Serum CA125 levels
The mean CA125 level pre-IDS (post-NAC) was 23.7 and 267 IU/mL in the PWC-negative and PWC-positive groups (p=0.066, Table 2). The CA125 ratio (pre-NAC / pre-IDS) of PWC-negative and PWC-positive patients was 0.03 and 0.12 (p>0.05, Table 2), respectively. The proportion of patients with ≥75.0 IU/mL pre-IDS serum CA125 level was 0% in the PWC-negative group and 55.3% in the PWC-positive group, respectively (p<0.01, Table 2). The median OS of patients in the <75.0 and ≥75.0 IU/mL pre-IDS serum CA125 groups was 45.3 and 18 months, respectively (p<0.001) (Fig. 3A). Univariate analyses showed associations with OS and PFS in terms of the pre-IDS serum CA125 level (≥75.0 IU/mL) (p=0.001 and p<0.01, respectively). In patients with pre-IDS serum CA125 levels of <75.0 IU/mL, the median OS was 53.5 and 35.5 months for the PWC-negative and PWC-positive groups, respectively (p<0.05) (Fig. 3B).
Fig. 3
Kaplan-Meier curves of OS according to serum CA125 levels. (A) <75 vs. ≥75 IU/mL before IDS and (B) <75 IU/mL before IDS in patients with positive vs. negative PWC.
CA125, cancer antigen 125; IDS, interval debulking surgery; NAC, neoadjuvant chemotherapy; OS, overall survival; PWC, peritoneal washing cytology; RD, residual disease.
*p<0.05.

5. Multivariate analysis
In a multivariate Cox regression model, in patients who had received NAC; PWC-negative, and histology (serous adenocarcinoma) were identified as independent favorable predictors of OS. PWC-negative was also identified as an independent favorable predictor of PFS. The hazard ratios for these variables are shown in Table 3. There were no significant differences in age, clinical stage, CA125 level pre-NAC, histology (clear cell carcinoma), NAC cycles (≤6), and the existence of EL.
Table 3
Multivariate analysis of OS and PFS in patients who had received NAC or undergone IDS
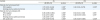
In patients who had undergone IDS; PWC-negative, with RD<1.0 cm, histology (serous adenocarcinoma), and the number of NAC cycles (≤6) were identified as favorable independent predictors of OS. PWC-negative, having an RD<1.0 cm and the number of NAC cycles (≤6) were also identified as independent positive predictors of PFS. The hazard ratios for these variables are also shown in Table 3. There were no significant differences in age, clinical staging, the serum CA125 level pre-NAC or IDS, the ratio of CA125 level, the duration from starting NAC to IDS, the existence of EL, completion of IDS, blood volume in IDS, histology (clear cell carcinoma), RD=0, or RD≥2 cm.
DISCUSSION
In this study, we investigated the prognostic significance of PWC in NAC-treated patients with ovarian cancer. Optimal debulking in IDS after NAC has been reported to be a prognostic factor for patients with ovarian cancer [167].
The PWC-negative patients in IDS exhibited a dramatically improved OS compared to PWC-positive patients in the Kaplan-Meier analysis. The PWC is not only a useful indicator of clinical staging and prognostic information in PDS [12], but it can also serve as an independent predictor of OS for IDS. The multivariate Cox regression analysis in our study supports this hypothesis.
Many studies have demonstrated a higher efficacy of surgery when combined with NAC for IDS [12347151617]. The 5-year survival rate of patients without RD after IDS was comparable to that of patients with minimal RD (RD<2.0 cm) after PDS, however, the 5-year survival rate of patients with minimal RD (RD<2.0 cm) after IDS is worse (0%) [15]. Onda et al. [16] suggested that the definition of optimal debulking in IDS should be no RD, despite the definition in PDS being RD<1.0 cm. This may be explained by the fact that the meaning of RD after PDS and IDS differs, as chemo-resistance may be altered by NAC [16]. In the present study, the median OS of patients in the debulking (RD<2.0 cm) and largest RD (RD≥2.0 cm) groups was 28.5 and 17 months, respectively (p<0.05) (Supplementary Fig. 1A), and the median OS of patients in the optimal debulking (RD<1.0 cm) and non-optimal debulking (RD≥1.0 cm) groups was 28.5 and 17 months, respectively (p<0.05) (Supplementary Fig. 1B), which showed that optimal debulking with RD<1.0 cm was associated with improved OS with statistically significant difference. Whereas, the median OS of patients in the no RD (complete cytoreduction; RD=0) and RD (incomplete cytoreduction; RD>0) groups was 27 and 20 months, respectively (p>0.05) (Supplementary Fig. 1C). This showed that complete cytoreduction did not improve OS because incomplete cytoreduction (RD>0) included optimal debulking with 0<residual tumor size<1 cm; and no significant difference in OS was observed between patients with no RD (RD=0) and those with minimal RD (0<RD<1.0 cm) in our study. The median OS of patients in the no RD (RD=0), RD 0–1, and RD>1.0 cm groups was 27, 31, and 17 months, respectively (Supplementary Fig. 1D). Thus, it is too difficult and subjective to identify microscopic peritoneal lesions, regardless of whether viable cancer cells are present or not. Microscopic lesions may remain due to inflammatory or fibrotic processes after NAC. PWC-positivity strongly correlated with large RD (RD>2.0 cm) in IDS, but did not correlate with minimal or no RD in our study. PWC may be more sensitive than macroscopic examinations to detect microscopic RD (MRD) which includes viable cancer cells, based on the positive association of PWC with reduced OS in patients who have undergone optimal debulking surgery (RD≤1.0 cm) and complete resection (RD=0) (Fig. 2). Therefore, PWC of the Douglas' pouch could be an effective alternative evaluation method that may aid in overcoming the deficiencies in detecting MRD using visualization and palpitation. Interestingly, 13 patients who had undergone complete cytoreduction (39.4%) were PWC-positive. This suggests that residual cancer cells may remain microscopically present in the peritoneum [14]. Four patients with RD 0<residual tumor size<1 cm were PWC-negative. This may be the result of inflammatory or fibrotic processes after NAC treatment or a reduction in cancer cell migration activity. However, additional research is needed to identify the relationship between PWC and the activity of viable cancer cells.
Favorable associations have been detected between survival and the extent of decline in serum CA125 levels after PDS for advanced-stage ovarian cancer [11], and the value of serum CA125 levels of <75.0 IU/mL after the third NAC-cycle is an independent predictor of complete IDS [17]. In our study, pre-IDS serum CA125 levels (≥75.0 IU/mL) were not only a predictive factor of OS and PFS, but also demonstrated a significant association with PWC status (Fig. 3A and Table 2). Among patients with pre-IDS serum CA125 levels of <75.0 IU/mL, the PWC-negative group exhibited a longer survival; the median OS was 53.5 and 35.5 months for the PWC-negative and PWC-positive groups in patients with pre-IDS serum CA125 levels of <75.0 IU/mL, respectively (p<0.05) (Fig. 3B). Therefore, PWC status may be a predictive prognostic factor, along with pre-IDS serum CA125 level, for patients with ovarian cancer.
The median OS of patients with serous adenocarcinoma and clear cell carcinoma was 27 and 14 months, respectively (p<0.001) (Supplementary Fig. 2A), which showed that patients with serous adenocarcinoma exhibited a good prognosis, while those with clear cell carcinoma exhibited a significantly poorer prognosis. Despite PWC-positivity, the median OS was longer in patients with serous adenocarcinoma; the median OS was 36.5 and 19.3 months for patients with serous adenocarcinoma and non-serous adenocarcinoma within the PWC-positive group, respectively (p<0.05) (Supplementary Fig. 2B). All clear cell carcinoma patients were PWC-positive, demonstrating that clear cell carcinoma is chemoresistant [1]. Therefore, NAC may not benefit patients with a chemoresistant histology very well, and another regimen of NAC may be needed especially for patients with clear cell carcinoma.
Within the IDS group (PWC-negative and PWC-positive patients), the median OS was 46 and 16 months for patients who had received ≤6 or >6 cycles of NAC, respectively (p<0.05) (Supplementary Fig. 3). As more cycles are needed to treat patients who are less responsive to NAC, it is feasible that a small number of NAC cycles (n≤6) may be a positive prognostic factor.
The limitations of this study include its retrospective single-center study design. Therefore, a large-scale prospective trial to justify the efficacy of PWC during IDS is warranted.
In conclusion, our study suggests that PWC during IDS may be a prognostic factor for NAC-treated patients with ovarian cancer, specifically for MRD. The PWC may aid in overcoming the difficulty in determining the presence of MRD using visualization and palpation. We propose that PWC should be included in the intraoperative evaluation of IDS.
 XML Download
XML Download