

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The association between neoplastic disease and thromboembolic disorders is well known; this association was first recognized by Trousseau in 1865 and has often been termed Trousseau's syndrome. Venous thromboembolism (VTE), including deep venous thrombosis (DVT) and pulmonary thromboembolism (PE), has been associated with patients with gynecologic malignancies [1]. The reported rate of DVT in gynecologic cancer patients ranges from 11% to 18% and the rate of PE ranges between 1% and 2.6% [2]. Thus, based on previous reports, there is a strong association between thromboembolism and gynecologic malignancies as established from the incidence of DVT and PE.
Ovarian cancer is known to display a particularly strong association with VTE as coagulopathy often occurs in patients with advanced or recurrent ovarian cancers that may result in DVT and/or PE [3]. A population-based study using the Danish Cancer Registry found a strong association between thromboembolic disorders and several cancers including ovarian cancer [4]. In another large-scale study, among 13,031 ovarian cancer patients, a 5.2% incidence of VTE was demonstrated within 24 months of diagnosis using the California Cancer Registry [5]. Similarly, ovarian cancer exhibited the highest incidence of cancer-related VTE, at 120 out of 10,000 patients, based upon Medicare data of hospital discharge diagnoses in the United States [6]. These large-scale or population-based reports likewise establish an underlying coagulopathy associated with ovarian cancer.
Although Trousseau's syndrome due to cerebral infarction is a relatively rare complication of malignant disease, compared to DVT or PE, it has been reported to occur most frequently in patients with lung, prostate, breast and ovarian cancer compared to patients with other malignant disease [4]. However, a review of the literature by Sack et al. [7] found that ovarian cancer represented only 3.8% of reported cases of Trousseau's syndrome associated with cerebral infarction. The majority of these previous reports consisted of small series of case reports and there have been few large series studies on the association of Trousseau's syndrome with cerebral infarction and ovarian cancer. Thus, we undertook the present study to investigate the association between cerebral infarction, especially cerebral ischemic stroke of the cerebral arteries resulting from thrombosis, and specifically ovarian cancer. We analyzed the incidence and association of Trousseau's syndrome associated with cerebral ischemic stroke, resulting from thromboembolism, with various clinical parameters associated with ovarian cancer.
MATERIALS AND METHODS
1. Patients
Between January 2001 to December 2012, 827 consecutive primary epithelial ovarian cancer patients treated at the Departments of Obstetrics and Gynecology of 4 academic medical centers affiliated with the Jikei University were included in the study (Jikei University School of Medicine, Jikei University Katsushika Medical Center, Jikei University Daisan Hospital, and Jikei University Kashiwa Hospital); all patients were histopathologically diagnosed as epithelial ovarian cancer and were treatment-naïve for malignant disease prior to enrollment in the study. All study protocols were approved by the Institutional Review Board of the Jikei University School of Medicine (approval number: 24-166) and all patients provided written informed consent to participate. Initial treatment for malignant disease was performed at the aforementioned academic medical centers. Treatment outcomes of patients were analyzed by review of their medical records for age, histopathological type, International Federation of Gynecology and Obstetrics (FIGO) disease stage and other clinical findings. Median observation duration was 1,428 days; observation was recorded from the date of either initial surgery or administration of first course of neoadjuvant chemotherapy.
2. Diagnosis of cerebral infarction
Enrollment in this study consisted of patients who had experienced a history of cerebral infarction within 1 year prior to commencement of treatment for malignant disease or who presented with cerebral infarction during initial clinical treatment for ovarian cancer; these patients were defined as Trousseau's syndrome for the purpose of this study and included in analysis. Medical records of cerebral infarction were collected from both referring institutions and affiliated institutions; diagnosis at referring institutions was corroborated as fully as possible by both medical records and imaging diagnosis while diagnosis at the aforementioned affiliated academic institutions were confirmed by computed tomography (CT) and magnetic resonance imaging (MRI) examinations and consultation with the attending neurosurgery and/or radiology specialists.
3. Clinical background of patients
Medical records of cerebral infarction patients were collected to evaluate for underlying systemic complications or lifestyle risk factors (smoking history). Medical conditions were defined by the following parameters: hypertension was defined as a systolic pressure greater than 140 mmHg and/or a diastolic pressure greater than 90 mmHg; hyperlipidemia was defined as a low-density lipoprotein (LDL) cholesterol level greater than 140 mg/dL or a triglyceride level greater than 150 mg/dL; and diabetes mellitus was defined as by a fasting blood glucose level greater than 200 mg/dL or HbA1c greater than 6.5% or by the presentation of overt clinical symptoms. Smoking history was corroborated from the patient's medical history.
4. Statistical analysis
Logistic regression analysis was performed for univariate and multivariate analysis with a p-value less than 0.05 considered to be significant. Statistical analysis software incorporated R version 3.3.1 (R Foundation for Statistical Computing, Vienna, Austria; www.r-project.org).
RESULTS
1. Patients characteristics
Eight-hundred twenty-seven patients were included in the study. The mean age was 54 years (range, 14–86 years). Histopathologically, the patients included 225 cases (27.2%) of serous carcinoma, 148 cases (17.9%) of endometrioid carcinoma, 93 cases (11.2%) of mucinous carcinoma, 275 cases (33.3%) clear cell carcinoma (CCC), and 86 cases (10.4%) of other histological subtypes. FIGO stage consisted of 407 cases (49.2%) of stage I disease, 90 cases (10.9%) of stage II disease, 282 cases (34.1%) of stage III disease, and 48 cases (5.8%) of stage IV disease (Table 1). Although the current histological classification of serous adenocarcinoma is classified as either high-grade and low-grade serous type (as defined in the 2014 version of the World Health Organization Classification of Tumors of the Female Reproductive Organs), the cases included in this study included cases from January 2001 to December 2012 and thus these cases were diagnosed under the previous histological classification criteria.
Table 1
Clinical characteristics

Among the 827 patients; 27 patients (3.2%) presented with cerebral infarction during the study period; 14 patients onset prior to treatment (1.7%) and 13 patients onset after start of initial treatment (1.5%). Median age at onset was 59 years (range, 36–86). Histopathologically, the patients consisted of 7 cases (25.9%) of serous carcinoma, 3 cases (11.1%) of endometrioid carcinoma, 2 cases (7.4%) of mucinous carcinoma, 15 cases (55.6%) of CCC, and 0 cases of other histological subtypes. FIGO stage consisted of 11 cases (40.7%) of stage I disease, 2 cases (7.4%) of stage II disease, 13 cases (48.1%) of stage III disease, and 1 case (3.7%) of stage IV disease (Table 1). Among the 7 cases of cerebral infarction that presented with serous carcinoma, 2 cases were grade 2 differentiation, 2 cases were grade 3 differentiation, while the grade of differentiation was not classified in the remaining 3 cases.
2. Risk factors for cerebral infarction
The incidence of systemic complications or lifestyle risk factors were low among the 27 patients that onset with cerebral infarction. Four patients (14.8%) presented with hypertension while 21 patients (77.8%) had normotensive blood pressure. One patient (3.7%) had underlying hyperlipidemia while 24 patients (88.9%) had normal lipid profiles. Similarly, no patients had underlying diabetes mellitus. Twenty-five of the patients (92.6%) were non-smokers. Thus, the overall incidence of systemic medical complications or smoking status was low among the study population (medical records could not be corroborated in 2 patients to assess the aforementioned risk factors; Table 2).
3. Statistical analysis
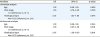
We performed both univariate and multivariate analysis of the onset of Trousseau's syndrome. Statistically significant associations were not demonstrated with age or FIGO stage (stages I–II vs. stages III–IV); however, both of univariate analysis and multivariate analysis demonstrated a statistically significant association with histological subtype (CCC or non-CCC; univariate analysis: p=0.042; odds ratio [OR]=2.22; 95% confidence interval [CI]=1.03–4.86 and multivariate analysis: p=0.016; OR=2.67; 95% CI=1.20–6.00) (Table 3).
Table 3
Association between age, FIGO stage or histological type with cerebral infarction
4. Clinical characteristics of cerebral infarction
Fourteen cases (51.9%) onset with cerebral infarction prior to start of initial treatment for ovarian cancer. Thirteen cases (48.1%) onset with cerebral infarction following start of treatment for ovarian cancer. Among the 13 cases of cerebral infarction, 3 cases occurred during chemotherapy following disease recurrence, while the remainder of the cases occurred after disease recurrence. These included 2 cases of cerebral infarction during the course of treatment for ovarian cancer; 1 case that onset after completion of initial adjuvant chemotherapy but prior to progression of malignant disease, while 1 case onset following progression of malignant disease. There was no association between treatment and occurrence of cerebral infarction. Initial symptoms at onset included 13 cases (48.1%) of hemiplegia, 10 cases of (37.0%) of dysarthria or articulation disorder, 3 cases (11.1%) of gait disturbance, 2 cases (7.4%) of visual field defect, and 7 cases (25.9%) presenting with other symptoms. Localization of the cerebral infarction lesion included 13 cases (48.1%) of the middle cerebral artery, 2 cases (7.4%) localized to the parietal lobe, 1 case (3.7%) localized to the occipital lobe, and 7 cases (25.9%) with multiple cerebral lesions (Table 4). Following anticoagulant therapy, all 14 cases underwent surgery; optimal surgery (residual tumor less than 1 cm in size) was performed in 13 cases while suboptimal surgery (residual tumor greater than 2 cm in size) could only be performed in 1 case.
Table 4
Clinical characteristics of patients that onset with cerebral infarction

DISCUSSION
This is the first large series study, comprising 827 consecutive ovarian cancer patients, to investigate the association of Trousseau's syndrome associated with cerebral infarction and ovarian cancer. We analyzed 27 cases of clinically diagnosed Trousseau's syndrome associated with cerebral infarction that either onset prior to treatment or after start of initial treatment of ovarian cancer. Statistical analysis demonstrated that Trousseau's syndrome occurred with greater incidence among CCC cases compared to non-CCC cases. However, there was no statistical significance with FIGO stage or age and the incidence of Trousseau's syndrome. Among the 27 cases, 13 cases onset after the start of initial treatment. Interestingly, there were 2 cases of recurrence of cerebral infarction during the courses of treatment for malignant disease; however, in both cases, recurrence of cerebral infarction occurred following progression of malignant disease. Conversely, there were no cases of cerebral infarction recurrence among patients that did not demonstrate disease progression of malignant disease.
Previous reports have demonstrated that early onset VTE events, during the courses of treatment for malignant disease, were associated with surgery and chemotherapy; whereas later onset VTE events during treatment for malignant disease were associated with other clinical parameters including older age, prior history of DVT, advanced FIGO disease stage, and presence of residual tumor after initial surgery [5]. In support of these findings, the 2 strongest risk factors associated with development of VTE in large-scale population-based studies were presence of metastatic cancer at the time of diagnosis and the presence of underlying chronic medical comorbidity, as reflected in older age and the presence of 2 or more chronic medical complications [5]. The results from our study did not necessary correspond to the results of these previous studies. Our analysis did not demonstrate an association of Trousseau onset with any treatment-associated risks including various surgical parameters nor with treatment outcomes of malignant disease. Furthermore, our analysis did not support an association with previously reported clinical parameters including advanced age or smoking history, or an association with underlying co-morbidities including hypertension, hyperlipidemia, or diabetes mellitus.
Our analysis, however, demonstrated a statistically significant association of Trousseau's syndrome onset with histological subtype, specifically CCC. This is supported by previous reports in the literature that have found a strong association between thromboembolism and CCC histology. Several published reports have supported the association between clear cell histology and VTE in ovarian cancer [89]. One report has calculated the incidence of VTE in ovarian CCC to be 2.5 times greater than the risk in other histologies [10], while other reports have suggested that symptomatic VTE occurs in 11%–13.7% of patients with CCC of the ovary [911]. Another report has found that VTE in ovarian CCC to be associated with decreased survival [12]. These reports have postulated that patients with clear cell histology display a significantly higher incidence (11%–42%) of VTE compared with those of non-clear cell histology in the immediate postoperative period and during primary chemotherapy. Thus, our findings demonstrate a statistically significant association of Trousseau's syndrome with ovarian CCC histology.
In the present study, the percentage of CCC, among the histological types of ovarian cancer, was the highest at 33%. In Japan, the nation-wide histopathological distribution for ovarian cancer includes, as the most common histological type, serous carcinoma at 33%, followed by CCC at 25% [13]. It should also be noted that in this study, there were a large number of ovarian tumors detected incidentally at health examinations; thus, this is reflected in our data as stage I disease comprising 49.2% of the cases (Table 5). Likewise, the relative percentage of serous carcinoma, which is most often seen in advanced cases, is lower than in other large-scale studies. Although the present study included a larger percentage of CCC and stage I disease compared to a nation-wide registry [13], we believe that the findings of our study are applicable to the overall population of ovarian cancer cases.
Table 5
Clinical characteristics of histpathological types and stage

Our findings in this study demonstrate that Trousseau's syndrome associated with cerebral infarction and ovarian cancer occurs with relatively low incidence. All of our patients presented with neurological symptoms that occurred at distant sites from the malignant ovarian tumor; it was surmised these cerebral infarctions were induced by the hypercoagulability of the malignant ovarian tumor. Our study also found that recurrence of cerebral infarction only occurred following progression of malignant disease and that there was a statistically significant association between Trousseau's syndrome associated with cerebral infarction and with ovarian CCC histology. Thus in summary, although cerebral infarction associated with ovarian cancer occurs with low incidence, it is a severe complication of the disease and must be treated accordingly; further studies are required to elucidate its mechanism of onset.
 XML Download
XML Download