

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ovarian cancer represents the most lethal gynecological cancer in developed countries [1]. Although growing surgical and medical attempts are improving the efficacy of first line treatments, the majority of ovarian cancer patients developed recurrent disease. The gold standard treatment for recurrent ovarian cancer (ROC) is chemotherapy (CT) [2]. However, accumulating data suggested that in selected patients secondary cytoreductive surgery (SCS) might be a valuable treatment modality. Although mature evidence is lacking, several investigations highlighted that SCS might improve outcome of patients suffering from platinum-sensitive recurrence [34567]. Moreover, the preliminary results of the ongoing Arbeitsgemeinschaft Gynaëkologische Onkologie Descriptive Evaluation of preoperative Selection of (K)Criteria for Operability in recurrent Ovarian cancer (AGO OVAR DESKTOP) III/ENGOTov20 study (comparing SCS plus CT with CT alone in patients with ROC) suggested that SCS improves platinum-free interval and disease-free survival (DFS) in comparison with CT alone [5].
Patient selection is paramount in order to reduce ineffective surgical attempts that might delay effective treatments such as CT. Several models were built in order to identify patients who deserve SCS [67]. However, from the other point of view, these models could be strict and a beneficial treatment could be denied in patients who do not met inclusion criteria.
Here, we aimed to evaluate if the application of artificial intelligence (AI) might be useful in weight the importance of individual patients' and diseases' variables, thus identifying ROC patients who deserve SCS [8]. In the present paper, using the results achieved by AI we aimed to assess importance of different variables in predicting complete cytoreduction (CC) at SCS. As secondary outcomes we aimed to evaluate whether the application of AI might replace the results achieved by conventional statistical analysis.
MATERIALS AND METHODS
This is a retrospective evaluation of patients undergoing SCS due to platinum-sensitive ROC. The National Cancer Institute (NCI) Institutional Review Board approved this study (approval number: INT/MI/006812). The paper included data from a series of consecutive patients with ROC undergoing SCS at NCI of Milan, from January 1, 2001 through December 31, 2015.
Patients who did not provide consent to use their medical information for research purposes were excluded from the present analysis. While, all the included patients signed written consent for research purpose.
Data were retrospectively retrieved from a computerized surgical database, containing data on every surgical procedure performed for the patients enrolled into the study. The computerized database was maintained prospectively and it is of research quality and has been updated by trained residents and nurses. Data included in the present study were already presented into a recently published paper evaluating predictors of CC in patients undergoing SCS for ROC [9]
Patients' records were screened in order to identify baseline patients' and diseases' characteristics. Inclusion criteria were: 1) age ≥18 years; 2) histologically-proven recurrence of invasive epithelial ovarian, primary peritoneal and Fallopian tube cancer (i.e., ROC); and 3) execution of SCS. Exclusion criteria were: 1) consent withdrawn; 2) absence of gross disease at the time of SCS; and 3) performance status (PS) not allowing surgical treatment. Central pathology review was performed in all cases, before having SCS.
Details about our surgical protocol are reported elsewhere [9]. Generally, SCS was offered to patients with recurrent disease with a disease-free interval (DFI) longer than 6 months. DFI was the time between the end of platinum-based adjuvant CT and the diagnosis of recurrence. Although no specific guidelines are available for the section to SCS, the surgical attempts were offered after the evaluation of the parameters included in both the AGO OVAR and Memorial Sloan Kettering (MSK) criteria: 1) no residual disease (RD) at first surgery; 2) good PS; 3) absence of ascites; 4) site of recurrence; and 5) DFI [3456]. According to the AGO OVAR criteria, ascites was recorded when free fluid was 500 mL or more. The diagnosis of carcinomatosis included the presence of diffuse peritoneal spread of the disease, into multiple anatomical sites. Since the primary goal of SCS is achieve CC, the primary outcome measure of our research is to identify factors associated with CC. Additionally, as secondary endpoints, we aimed to weight the importance of those factors in influencing survival outcomes.
The innovation of the present paper is based on the use of AI (artificial neuronal network [ANN] analysis). ANN was used in order to weight the importance of associated variables, thus predicting the effect of each variable on achieving CC and survival outcomes. This analysis is a system of interconnections based on simple mathematical model associated with learning algorithms. ANN comprised a 4-layer (1 input layer, 2 hidden layers, and 1 output layer) feed-forward analysis. To develop the ANN, cases were randomly assigned to the training group (80%) or to the testing group (20%) through a generator of random numbers. The back propagation of the error was applied as a learning rule using the online training method. Synaptic weights were updated after each training data record. Detailed description of ANN is reported elsewhere [810].
Basic descriptive statistics were used. Kaplan-Meier and Cox proportional hazard models were used appropriately in order to evaluate the impact of the predicting variables on survival outcomes. Hazard ratio (HR) and 95% confidence intervals (CIs) were calculated for each comparison. Univariate and multivariate analysis were performed when appropriate. All covariates with a p-value less than 0.10, based on univariate analysis were included in the multivariate model. Statistical analyses were performed using the GraphPad Prism version 6.0 for Mac (GraphPad Software, San Diego, CA, USA) and IBM-Microsoft SPSS version 22.0 for Mac (IBM Corp., Armonk, NY, USA). All p-values were 2-sided. The p-values <0.05 were considered statistically significant.
RESULTS
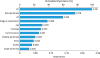
Overall, 199 patients, had SCS due to the diagnosis of ROC. Five patients were excluded since they did not provide consent to use their medical information for research purposes, thus leaving 194 (97.4%) patients available for the analysis. Fig. 1 shows the flow of patients into the study design. Baseline patients' characteristics are reported in Table 1. In our population, 161 (82.9%) patients had CC at the time of SCS. Using ANN, we observed that the 3 main factors driving the ability of achieve CC included: DFI (importance: 0.231), retroperitoneal recurrence only (importance: 0.178), RD at primary surgical treatment (importance: 0.138) and International Federation of Gynecology and Obstetrics (FIGO) stage at presentation (importance: 0.088). Fig. 2 displays the results of ANN and the importance of various predicting factors.

Table 1
Baseline patients' characteristics (n=194)
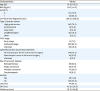
Fig. 2
Importance of factors predicting for CC.
CC, complete cytoreduction; DFI, disease-free interval; ECOG, Eastern Cooperative Oncology Group; RD, residual disease.
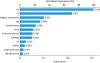
Looking at connections between covariates and overall survival (OS), we observed that DFI is the most important variable influencing OS (importance: 0.306). Other important variables included: CC (importance: 0.217), and FIGO stage at presentation (importance: 0.100). Fig. 3 shows the results of ANN related to the connections between predictive variables and OS. Patients having CC experienced a median OS of 40.5 vs. 23.0 months for patients having incomplete resection, respectively (p<0.001, log-rank test). Although it did not reach statistical significance, patients with early stage disease at presentation (FIGO stage I–II) experienced better survival than patients with advanced stage (FIGO stage III–IV) of disease: median OS 59.7 vs. 33.0 months, respectively (p=0.120, log-rank test).
DISCUSSION
The present study investigated how the adoption of AI might be useful to identify characteristics that might choose to undergo SCS due to ROC. We observed that among our population DFI is the main factor predicting for CC at SCS. Another important factor for the outcome of SCS is site of recurrence. In particular, our data underlined that the presence of retroperitoneal disease alone is associated with an increased ability to achieve CC in comparison to the presence of peritoneal disease. Interestingly, the presence of single peritoneal, multiple peritoneal nodules and carcinomatosis had a limited impact on the ability to achieve CC, thus highlighting that the presence of carcinomatosis should not be considered a contraindication for SCS. CC is the main variable influencing patients' survival, followed by DFI, and FIGO stage at presentation. Site of recurrence (peritoneal vs. retroperitoneal) had no impact on survival outcomes.
Accumulating data support that in patients with ROC, the execution of SCS is related to important improvement in survival outcomes when CC is achieved. Therefore, patients' selection is paramount in identifying patients who deserve surgical attempts. As aforementioned, few investigators tried to build model useful in patients' selection [1112131415].
The AGO OVAR DESKTOP I and II studies evaluated the importance of achieving CC at the time of SCS and proposed positive predictors in order to enrich a population in whom SCS has a high probability for CC [345]. These criteria included: 1) absence of RD at first surgery; 2) good PS; and 3) absence of ascites (<500 mL). Similarly, the “MSK criteria” represent a useful tool in predicting CC [67]. These criteria are based on the site of recurrence (i.e., single, multiple, and carcinomatosis) and DFI [67]. However, the available model might be too strict thus prohibiting a beneficial treatment in patients who do not meet these criteria. Recently, our study group published a combined score using the variables included in both the 2 most reliable models (i.e., the AGO OVAR and MSK criteria) [9]. Adopting our nomogram, we were able to predict the probability to achieve CC based on the AGO OVAR (RD at primary surgery, PS, and presence of ascites) and MSK (DFI and site of recurrence) criteria [9]. Other investigators included in their models the evaluation of serum markers levels (i.e., CA-125 and HE4) and other characteristics of the disease at presentation such as FIGO stage and histology [1112].
Although level A evidence supporting the role of SCS in ROC is not still available, preliminary data of the OVAR DESKTOP III/ENGOTov20 study suggested that SCS is a valuable option for ROC patients, since it improves DFS. Other trials are ongoing, including the SOC 1 trial [16]. While, the SOCceR trial was spotted prematurely in August 2015 due to the lagging of inclusion [17].
In the present study, adopting ANN we observed that DFI is the main factor impacting the ability to obtain CC. In contrast with other group, we observed that site of recurrence is an important factor in predicting CC. In particular, both the AGO OVAR and MSK criteria did not focused on the presence of retroperitoneal localization. In our experience, we observed a great difference between retroperitoneal and peritoneal recurrences. Moreover, we also observed that also FIGO stage at presentation is an important factor that might have to be taken into account when we manage patients with ROC. The presence of ascites and carcinomatosis had per se a limited impact on the ability to achieve CC.
The adoption of ANN represents the main novelty of the present investigation. The utilization of AI provides more insight in identifying variables for predicting CC and OS. Although our study confirmed data observed in other studies [67], ANN weighted how a variable impact on outcomes. However, the inherent biases of the single-center retrospective study design represent the main weaknesses of our study. Moreover, our population included a selected group of ROC patients and it is not fully projectable on the whole group of ovarian cancer patients presenting with recurrent disease.
SCS represents a valuable therapeutic option for a selected group of ovarian cancer presenting with platinum-sensitive recurrence [131415]. Patients selection is the key point for SCS. In the present paper, we observed that applying AI helped to weight the importance of various predicting variables. Through AI we estimated that DFI and the presence of retroperitoneal recurrence are the main factors enabling to predict CC and OS. Additionally, CC is strictly related to oncologic outcomes. Further innovative methods are needed to provide an improvement in patients' selection.
 XML Download
XML Download