

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervical cancer is the fourth most prevalent cancer in women worldwide. In 2012, there were an estimated 530,000 new cases and more than 270,000 deaths, representing 7.5% of all female cancer deaths. More than 85% of morbidity and mortality occur in less developed regions of the world [1]. In developed countries, programs are in place to assertively encourage screening and identify pre-cancerous lesions when they can easily be treated. Therefore, early treatment prevents up to 80% of cervical cancers in these countries. The high mortality rate from cervical cancer globally (52%) could be reduced by providing screening and treatment programs. In developing countries, limited access to effective screening programs means that cervical neoplasia is often identified in an advanced stage with symptoms. Consequently, radical treatment of such late-stage disease is less effective, resulting in a higher rate of mortality from cervical cancer [123]. Due to inadequate investments in screening, diagnosis, and treatment, one-third of the cervical cancer burden worldwide occurs in south Asian countries including Nepal, India, Bangladesh, and Srilanka [4].
In Nepal, the most recent data 2016 indicates that 2,332 women are diagnosed with cervical cancer and 1,367 died from the disease annually with a peak incidence between 45 to 65 years of age [5]. However, in Nepal, there is no population-based national cancer registry. Therefore, available data for the cervical cancer burden may be an underestimation. Moreover, Nepal has seen an increasing incidence of cervical cancer; opposite the trend in developed countries. A study conducted in a cancer hospital from 1999 to 2008 found that among 11,469 cases of all cancer, 29% (n=3,372) cases were cervical cancer and there was a pattern of rising incidence over the 10-year period [6]. Nepal is carrying a massive burden of cervical cancer yet there is no established national cervical cancer screening program [7]. As a result, only a very few women undergo an opportunistic screening test. Educational awareness campaigns and organized rural outreach screening program are needed to boost screening rates for cervical cancer [68].
Women living in rural, mountainous areas are at particular risk of delayed diagnosis of cervical cancer. Often illiterate, they typically marry in early age, have limited access to health care, and rarely undergo cervical cancer screening [9]. In light of the poor health indicators and high-risk behaviors, the purpose of this study was to address the urgent need to assess the burden of cervical neoplasia in a rural district of Nepal. We sought to answer the following questions:
1. What are the socio-demographic and reproductive characteristics of women in rural Nepal?
2. What is the prevalence of cervical cancer among women in rural Nepal?
3. What is the association between the women's socio-demographic and reproductive characteristics and their cytology reports?
MATERIALS AND METHODS
1. Setting and population
The setting was Nepal's Jumla district. Located in mid-western Nepal, Jumla is a remote mountainous district of State 6 with an area of 2,531 km2. Jumla links to Surket and the rest of the country via a poor road with seasonal access. Within Jumla, residents must walk up to 6 to 7 hours to reach to the Hospital of Karnali Academy of Health Sciences (KAHS), the only hospital located in district headquarters and individuals seeking treatment at the Bharatpur Cancer Hospital, Chitwan or in the capital city, Kathmandu, travel a tiresome, hazardous bus journey of 30–36 hours.
According to the national census 2011, the total population of Jumla was 108,921 with 24,403 women age 20 to 64 years [10]. Compared to indicators of the Human Development Index (HDI), the Jumla district ranks among the lowest in Nepal in both relative and absolute terms. The HDI of Nepal is 0.558, whereas that of Jumla is 0.409 [1112]. Moreover, in Jumla, the maternal mortality ratio (400/100,000 live births), female life expectancy at birth (47 years), and literacy rate (41%) are clearly below national figures. Compared with Nepal overall, girls in Jumla tend to marry younger (before age 19) and have more children (total fertility rate is 4.2) [1013].
2. Design, recruitment, and sample
Following ethical review board approval from Nepal Health Research Council (No. 1785), Nepal, a cross-sectional, population-based study was conducted from May 2016 to January 2017. The inclusion criteria were: apparently healthy, married women, 20–65 years of age, with no past history of cervical cancer. Women who sought any kind of gynecologic health care, were pregnant, or wished to not participate were excluded. However, those ineligible women for this study were managed according to the standard protocol.
Women were openly invited by radio, local newspaper and local health professionals for cervical cancer screening. Group health education sessions were offered to promote awareness of cervical cancer and encourage participation in the screenings. Leaflets and pamphlets about cervical cancer prevention were distributed in the Nepali language. A total of 2,279 women participated in the sessions, then all of them were informed about this study in local Nepali language and 96.09% (n=2,190) women gave informed consent by of signature or thumbprint to participate. Illiterate women and those who were not able to write voluntarily gave their thumbprint as a consent to participate in this study. Prior to the screenings, participants were asked to complete a self-report questionnaire of socio-demographic characteristics and reproductive health.
3. Screening procedure
The screenings consisted of Papanicolaou smear and the visual screening tests provided in 3 mobile screening clinics and the KAHS. The screenings were conducted by 4 female Medical Assistants trained with 2 days of lecture, discussions, and video presentations based on a manual prepared by family health division, Nepal and International Agency for Research on Cancer (IARC) [1415]. Two physicians performed biopsies and managed possible complications and 2 pathologists analyzed the cytology and biopsy specimens. The flow chart of screening is presented in Fig. 1.
Fig. 1
Screening flow chart. Cytology abnormal includes; ASCUS, LSIL, HSIL, and SCC.
ASCUS, atypical squamous cells of undetermined significance; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; VIA, visual inspection with acetic acid; VILI, visual inspection with Lugol's iodine; SCC, squamous cell carcinoma.

The screening tests were carried out in the following order: specimen collection for cytology, visual inspection with acetic acid (VIA) and visual inspection with Lugol's iodine (VILI). Cytology was prepared by spreading the specimen uniformly across the glass slide and fixing it in 95% ethanol. VIA finding was recorded one minute after the application of 5% acetic acid. A second team, blinded with the VIA finding, performed and recorded the VILI finding by applying Lugol's iodine to the cervix. Punch biopsies were obtained from areas on the cervix assessed by VIA and or VILI to be abnormal. Biopsy specimens were fixed in 10% formalin and sent to the pathologist.
4. Definition of a positive result and treatment
Cytology results were reported according to the Bethesda system 2001 [16]. Cytology was considered to be positive at the low-grade squamous intraepithelial lesion (LSIL) threshold. Cytology reports were broadly classified into abnormal and normal. Abnormal cervical cytology included atypical squamous cells of undetermined significance (ASCUS), LSIL, high-grade squamous intraepithelial lesion (HSIL), and squamous cell carcinoma (SCC). Normal cervical cytology included negative for intraepithelial lesion or malignancy (NILM), inflammatory changes and other endometrial shedding. VIA was considered to be positive if definite acetowhite lesions were visualized close to the squamocolumnar junction, or the entire cervix or a growth on the cervix turned acetowhite. VILI was considered to be positive if yellow, iodine non-uptake areas were visualized close to the squamocolumnar junction, or the entire cervix or a growth on the cervix turned yellow [15]. Biopsy was the gold standard for defining final disease status. Biopsy results were reported based on World Health Organization (WHO) Classification of Tumors of Female Reproductive Organs published on 2014 [17]. In case the biopsy was not taken, patients were managed on the basis of cytology. To minimize possible bias, quality control measures were implemented during data collection, sample collection, reporting, and analysis.
Women were treated based on biopsy report. Women with LSIL were given a choice of immediate treatment or follow-up after 6 months. Women with HSIL were recommended for treatment with cryotherapy or loop electrosurgical excisional procedure (LEEP) or cone excision, or hysterectomy. Women with invasive cancers were referred for further management.
5. Statistical analysis
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS version 20.0; IBM Corp., Armonk, NY, USA). Descriptive statistics were used to describe the women's socio-demographic characteristics and reproductive health. Prevalence was determined with percentages and cross-tabulations were used to describe the association of potential risk factors with an abnormal cytology outcome. The χ2 test was used for statistical significance. The p<0.05 was considered as significant. Relative risk (RR) for abnormal cytology was calculated at 95% confidence interval (CI). The association of abnormal cervical cytology with potential risk factors — age, marital age, educational status, number of pregnancies, tobacco smoking, and participant's and husband's sexual behavior, etc. was analyzed using RR and significance test calculation.
RESULTS
1. Socio-demographic characteristics
The socio-demographic characteristics of the 2,190 eligible participants are summarized in Table 1. The mean age was 32.78 ± 9.33 years and the average age of marriage was 16.61 ± 3.42. There was 45.25% illiteracy. However, among the literate group, 51% could barely read but not write (informal education). Among the participants, 66% had more than 3 pregnancies.
Table 1
Socio-demographic and reproductive characteristic of participants (n=2,190)

2. Prevalence of cervical cancer
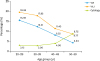
Cytology, VIA, and VILI were done for all eligible participants. Due to 38 unsatisfactory cytology samples and 47 participants who refused the test, there were 2,113 eligible samples with cytology report. A total of 381 biopsies were taken; 10 had an inadequate or autolyzed sample (Table 2). The overall rate of positive results of cytology, VIA, and VILI were 3.69%, 12.45%, and 16.89%, respectively. The positive rate trend of the 3 different tests according to the age group is presented in Fig. 2. The rate of cytology positivity increased with age, with the highest rate (8.76%) in women ages 50–65, but the rate of positivity of VIA and VILI was decreased with increasing age of women.
Table 2
Cytology and biopsy reports

Data shown are number (%).
ASCUS, atypical squamous cells of undetermined significance; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; NILM, negative for intraepithelial lesion or malignancy; SCC, squamous cell carcinoma.
*Excluded from total cytology and biopsy.
Fig. 2
Distribution of screening positive rates of cytology, VIA, and VILI in different age group.
VIA, visual inspection with acetic acid; VILI, visual inspection with Lugol's iodine.
The cytology and biopsy results are presented in Table 2. Women with normal result in cytology were suggested for routine screening test according to the national protocol. The total of 62 cases were biopsy proven positive for cervical neoplasia. Out of 41 LSIL cases, 20 underwent for cryotherapy and 21 opted for follow-up in 6 months. Among 14 HSIL cases, LEEP was done in 8 cases; simple hysterectomy was done in 4 cases where the woman who had already completed her family, and 2 patients refused treatment. The 7 patients with invasive cervical cancer were referred to the cancer center for further management, but 3 of them refused despite repeated counseling and financial aid. Cytology positive but biopsy negative cases were counseled for a repeat test. Two patients with SCC in cytology were referred for further evaluation.
3. Participant characteristics and cytology reports
Table 3 shows the univariate analysis of different variables with cytology outcome. RR of age more than or equal to 46 years had 2.07 (95% CI=1.16–3.68; p=0.013). RR of marital age less than or equal to 19 had 0.50 (95% CI=0.31–0.81; p=0.004). RR of illiterate women had 2.04 (95% CI=1.29–3.20; p<0.001). Similarly, participant's multiple marriages or who had multiple sexual partners (p=0.005) and participant's positive human immunodeficiency virus (HIV) status had a significant association with abnormal cytology result (p<0.001), but past history of sexually transmitted infection (STI) and multiple marriages of participant's husband were not significantly associated.
Table 3
Univariate analysis of different variables with cytology report (n=2,113)
DISCUSSION
To our knowledge, this is the first population-based study conducted in the mid-western mountainous rural district of Nepal to assess the burden of cervical neoplasia on apparently healthy women primarily by conventional cytology and simultaneously by VIA and VILI. Our finding reflects the characteristics of the female population of Jumla where 82.38% of women marry before the age of 19. The results showed 3.69% abnormal cervical cytology among these 2,113 women aged 20–65. The rate of abnormal cytology is slightly higher than other studies conducted in semi-urban or urban regions of Nepal [181920]. Bhatta et al. [21], in a comparison of abnormal cervical cytology among 576 Nepalese and Bhutanese women living in eastern Nepal, found abnormal cervical cytology over 7%; 2 times higher than the present study findings. There was an even higher rate of abnormal cytology (12.4%) in a study conducted by Shakya et al. [7], among 1,162 women in Kavre district of Nepal. These discrepancies may be due to differences in the smear processing method; study setting with different populations; or most importantly, the variability of sensitivity and specificity of cytology itself and limitation of the accuracy of cytology [22]. We tried to minimize possible bias with the application of test gold standard, periodic team conferences, and orientation of involved personnel regarding handling and reporting of samples.
GLOBOCAN 2012 estimates that peak incidence of cervical cancer occurs between 45–65 years and is 54–75 cases per 100,000 women per annum [1]. But because of lower life expectancy of women in Jumla, the total population of 45 to 64 years' women is just 6,584 (6% of the whole population) [10], this could be the reason why the rate of cervical neoplasia seems lower than might be expected. In this study, 6.89% of the women were aged 50–65 years, which is comparable and representative of the same age group of total women's population in Jumla.
Positive rates of VIA and VILI were much higher than the cytology with the higher positive rate seen in younger women. In the 20–29 year's age group, VIA and VILI was 15.59% and 19.59% and in 50–65 year's age group was 4.41% and 8.76% respectively. This result is similar to the findings of previous studies [2324]. The high positive VIA and VILI in sexually active age group might be explained by the inflammatory cause or lower positive rate among elderly women may be due to the difficult visibility of squamocolumnar junction.
The potential high-risk behaviors for cervical neoplasia are early marriage (i.e., early sexual contact), high parity or childbirth, low literacy rate, tobacco smoking, participant's or husband's risky sexual behavior, the high prevalence of sexually transmitted disease, and malnutrition. All of these factors exist in Jumla. The prevalence of most of these characteristics is relatively higher than the findings reported by other similar studies conducted in different parts of the country [72021]. This might be due to high illiteracy, poverty, lack of health awareness, and lack of women empowerment. In univariate analysis, illiterate women appear to be at higher risk for cervical neoplasia than the literate group (RR=2.041; 95% CI=1.299–3.204; p<0.001). Similarly, other variables such as age over 45 years, multiple marriages or multiple sexual partners, and positive HIV status group are significantly associated with abnormal cytology. Though only 0.32% (n=7) participants reported HIV positive status, 4 had abnormal cytology which is less in absolute number but statistically significant. This result is consistent with a previous study [25]. Multiparity/multiple pregnancies, smoking and husband's multiple marriages or multiple sexual partners were weakly associated but not statistically significant. These findings are somewhat similar to the previous report which states that number of childbirth increases the risk of cervical neoplasia in the presence of persistent high-risk human papillomavirus (HPV) infection but not with the number of pregnancy, contraceptive use or sexual behavior [526]. The RR in between early marriage and abnormal cytology is less than one (RR=0.506; 95% CI=0.315–0.814; p=0.005), and statistically significant. Louie et al. [27] mentioned that women who initiate first sexual intercourse and pregnancy at a younger age are at higher risk for cervical cancer which is clearly in contrast to our present findings. Early sexual debut may be the risk factor for HPV infection but not necessarily abnormal cytology. Cytology seems to be abnormal in relatively older age especially in case of persistent high-risk HPV infection, whereas HPV is more prevalent in younger one.
There were some major strong points of this study. It was the first study among the relatively large population in the extremely remote region to identify the burden of cervical neoplasia and more than 96% of participants accepted the screening tests. However, there were some limitations in this study as well, it took 4–6 weeks to provide the cytology and biopsy report. The specimens were transferred to Kathmandu for reporting due to the unavailability of pathologist and infrastructure in Jumla, which caused some delay and follow-up loss. Despite our strong willingness, we were unable to use colposcopy due to some logistics reasons such as electricity issue, transportation problem and limited budget. Limitation of sensitivity and specificity of screening tests exist in this study. Longitudinal studies are difficult to conduct in this setting since difficult topography, lack of health awareness and women empowerment and attrition problem all exists.
In summary, based on cytology reports, we found 3.69% prevalence of cervical neoplasia among women in a rural region of mid-western, Nepal. Because of the difficult geographic location and socio-economic conditions in this poor resource setting, visual tests, VIA and VILI, can be a very good alternative cervical cancer screening test. A “screen and treat” approach would be more attractive but further research is needed to make these tests more effective, accessible and acceptable.
 XML Download
XML Download