

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vulvar squamous cell carcinoma (VSCC) is a rare malignancy with an incidence of 1–2 per 100,000 women-years [12] in women younger than age 50 years, rising to as much as 13 per 100,000 women-years in women older than 85 years [2]. Traditionally, the surgical treatment for early-stage VSCC was a complete resection of the tumor lesion with at least 2 cm tumor-free margins [3] with or without unilateral or bilateral inguino-femoral lymphadenectomy, depending on tumor size and location [456]. However, in the last decade, there have been efforts to limit the morbidity and psychological effects of radical surgery while maintaining good oncological control. The current consensus is to achieve a surgical margin >1 cm with a histological tumor-free margin ≥8 mm in early-stage VSCC [378910], although there has been growing criticism on the conflicting data available on the role of margin distance on VSCC recurrence and overall survival (OS) [111213141516]. This lack of consensus is clearly demonstrated in the recommendations of German, U.S. and European vulvar cancer treatment guidelines. In Germany, expert consensus of the Deutsche Gesellschaft für Gynäkologie und Geburtshilfe (DGGG) and Deutsche Krebsgesellschaft (DKG) guidelines recommend a minimum tumor-free margin of 3 mm on histological examination [17], whereas in the U.S., the National Comprehensive Cancer Network (NCCN) guidelines recommend tumor-free margins of 1–2 cm in early-stage VSCC [18]. Finally, the European Society of Gynecological Oncology (ESGO) advises to consider narrow margin in aims to preserve key structures such as the clitoris or anus [16].
Most studies in the literature have mixed disease stage cohorts (i.e., positive and negative nodal disease combined in a single cohort), mixed treatment approaches (i.e., lymphadenectomy vs. sentinel lymph node biopsy or both) or may lack long-term follow-up. Thus, they do not provide specific information on the effect of margin distance on long-term survival in early-stage, node negative VSCC. In the only published study of early-stage VSCC, Woelber et al. [15] found no significant impact of tumor-free margin distance on recurrence rate (RR) at the 8-mm margin cut-off, although with a median follow-up of 35.1 months, this study does not provide information on the effects of margin distance on long-term survival in the stage IB/II VSCC subgroup. Therefore, the main aim of this study was to identify a minimum tumor-free margin cut-off that provides long-term oncological safety in early-stage, node negative VSCC patients.
MATERIALS AND METHODS
This was a retrospective cohort study. Clinical records of patients diagnosed with primary invasive, keratinizing VSCC from 1981 to 2014 at St. Anna Hospital, were reviewed. Patients with bowenoid or basaloid squamous cell carcinoma on histology were excluded. Patients with International Federation of Gynecology and Obstetrics (FIGO) (2009) stages IB/II [19], who had a radical total or partial vulvectomy or a wide local excision of the tumor, with negative margins, known histological margin distance, bilateral inguino-femoral lymphadenectomy with negative lymph nodes were included in the analysis. Patients who only had a sentinel lymph node biopsy were excluded from the study. Among the 569 patients treated in our clinic in that period, 114 met the study criteria. All 114 patients underwent bilateral inguino-femoral lymphadenectomy and were operated by the same surgeon. Evaluation of tumor-free margin distance was performed by 2 pathologists on hematoxylin and eosin stained slides. The presence of lichen sclerosus as a peri-tumoral lesion was recorded. The study was approved by the Institutional Review Board of the Sant'Anna Hospital, University of Turin in Italy.
1. Primary and secondary outcomes
The primary aim was to identify the minimum tumor-free margin distance that confers long-term oncological safety in patients diagnosed with early-stage VSCC (FIGO IB/II), treated with vulvectomy plus bilateral lymphadenectomy. For this, a preliminary analysis was performed on tumor-free margin distance and its effect on long-term survival. The secondary outcome was to compare OS, disease-specific survival (DSS) and RR at the minimum margin cut-off, in order to compare survival outcomes to those observed at the recommended 8 mm margin cut-off. For this, the cohort (n=114) was divided into <5 mm and ≥5 mm margins (which corresponds to the minimal margin-distance cut-off found in the preliminary analysis) and later, the same cohort (n=114) was divided into <8 and ≥8 mm, which corresponds to the minimum histologic margin distance recommended in the literature [378910].
2. Topographic classification of vulvar recurrences
The localization of the tumor and local recurrences were recorded. For a precise anatomical localization of the lesion, the vulva was divided into 4 areas delimited by an imaginary horizontal line passing through the superior border of the hymen (i.e., anterior and posterior lesion) and by a vertical line from the clitoris to the anus (i.e., right or left lesion). An ipsi-regional vulvar recurrence was considered to be a vulvar cancerous lesion that developed on the same vulvar area with respect to the location of the primary VSCC. A non ipsi-regional vulvar recurrence was considered to be a vulvar cancerous lesion that developed on a different vulvar area with respect to the location of the initially treated primary VSCC [17]. All patients' records contained a detailed drawing of the tumor's location in relation to the vulvar anatomy, while most patients' files also contained a Polaroid photograph of the vulvar tumor taken at the time of diagnosis.
3. Statistical analysis
Patients' age, body mass index, tumor size, tumor invasion depth, tumor-free margin distance, number of inguino-femoral lymph nodes removed and clinical follow-up data were recorded and compared between groups with unpaired t-test or Mann-Whitney test. Time to VSCC recurrence and corresponding treatment received was also recorded.
In the preliminary analysis, margin distance was treated as a continuous and categorical variable, as previously reported in the literature [15], with aims to identify the minimum margin distance that conferred long-term oncological safety in terms of OS. Once the minimum margin distance was identified (5 mm, see results section and Supplementary Figs. 1, 2, 3, 4, 5, 6, 7, 8, 9) and the patient cohort was divided according to margin distance at the 5 mm and 8 mm cut-off to assess the effect of margin distance on OS, DSS, and RR. OS, DSS, and RR were estimated by the Kaplan-Meier method. Log-rank test was used to compare the survival curves at the < cut-off and ≥ cut-off. In OS, an event was defined as death by advanced vulvar cancer or death by any cause, while in DSS an event was defined as death by vulvar cancer. Patients with no events at the time of their last follow-up were considered censored. The effect of margin status on patient survival was further evaluated with Fisher's exact test. Statistical analysis was performed with GraphPad Prism version 6 (GraphPad Software, La Jolla, CA, USA). Differences were significant at p<0.05.
RESULTS
One hundred and fourteen patients met the study criteria. Mean age of VSCC patients at diagnosis was 68 years (median 69 years, range 35–89 years). Patients underwent either a total radical vulvectomy (n=46) or partial vulvectomy (n=68) plus bilateral inguino-femoral lymphadenectomy with triple incisions (n=114), complete removal of inguino-femoral lymph nodes with sparing of the femoral fascia [20]. All patients had negative lymph nodes on histopathological examination. None of the patients received adjuvant treatment following primary VSCC surgery. Vulvar recurrences were treated surgically, whereas patients who developed metastatic disease received adjuvant treatment. Mean length of follow-up was 89 months (median 80 months, range 5–273 months), whereas 71% of patients in this cohort had periodical clinical follow-up documented for at least 90 months.
From the 114 patients analyzed, 46 (40%) developed vulvar recurrences (3 of which developed concomitant metastatic disease), 18 died of vulvar cancer, 5 died of other malignancies (1 of breast cancer, 2 of ovarian cancer, and 2 of lung cancer) and 7 died of cancer-unrelated causes during the follow-up period. Overall, vulvar RR at 2, 5, and 7 years post-surgery was 4%, 13%, and 31%, respectively. Ipsi-regional recurrences were recorded in 18 out of 46 patients (39%), while non ipsi-regional recurrences were observed in 28 out of 46 patients (61%). Median time from surgery to ipsi-regional or non ipsi-regional recurrences was 17 and 59 months, respectively. Median time from first recurrence to death by VSCC was 17 months (range 1–133 months, n=18). Ipsi-regional recurrences were associated with a significantly higher disease-specific mortality when compared with non ipsi-regional recurrences (hazard ratio [HR]=6.28; 95% confidence interval [CI]=2.04–19.4; p=0.001, log-rank test, Supplementary Fig. 1). Further analysis revealed no association between the presence of peri-tumoral lichen sclerosus lesions reported within the margin of resection (n=59) and VSCC RR (p=0.44, Fisher's exact test).
OS at 2, 5, and 7 years was 95%, 86%, and 78%. DSS was 96%, 90%, and 84% at 2, 5, and 7 years following surgical treatment of the primary tumor. Median survival of patients that died from VSCC was 44 months (range 13–158 months, n=18).
1. Minimum tumor-free margin distance
Preliminary analysis at 8 different tumor-free margin cut-offs (3–10 mm) indicates that 5 mm is the minimum margin distance that confers oncological safety in terms of long-term patient survival. There is a significant decrease in OS at the 3–5 mm margin cut-offs (Supplementary Figs. 2, 3, 4). Furthermore, there is a striking difference in OS at the 5-mm cut-off when comparing the <5 mm and ≥5 mm groups (p=0.002, log-rank test, Supplementary Fig. 4). No difference in long-term OS was evident at the 6–10 mm margin cut-offs (Supplementary Figs. 5, 6, 7, 8, 9).
2. Effect of margin distance in RR and mortality
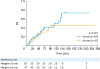
RR did not differ between groups at the 5-mm margin cut-off (Fig. 1), nor was evident at the recommended 8 mm margin cut-off (Fig. 2). The incidence of ipsi-regional recurrence lesions was similar between the <5 mm and ≥5 mm margin groups (41% vs. 38%, respectively). Although disease-specific mortality was high in patients with <5 mm surgical margins who developed ipsi-regional recurrences (4/5 or 80%), formal statistical analysis was not possible due to the small the sample size.
Fig. 1
RR in patients with tumor-free surgical margins <5 mm (n=29) or ≥5 mm (n=85), following surgical treatment for stage IB/II (FIGO 2009) VSCC. Number of patients at risk is provided at the bottom of the figure. Log-rank test was used to compare curves among groups.
FIGO, International Federation of Gynecology and Obstetrics; RR, recurrence rate; VSCC, vulvar squamous cell carcinoma.
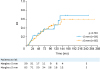
Fig. 2
RR in patients with tumor-free surgical margins <8 mm (n=67) or ≥8 mm (n=47), following surgical treatment for stage IB/II (FIGO 2009) VSCC. Number of patients at risk is provided at the bottom of the figure. Log-rank test was used to compare curves among groups.
FIGO, International Federation of Gynecology and Obstetrics; RR, recurrence rate; VSCC, vulvar squamous cell carcinoma.
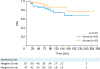
OS was significantly lower in the <5 mm group when compared with the ≥5 mm margin group (p=0.002; HR=2.92; 95% CI=1.25–6.83, log-rank test). Furthermore, 5-year DSS was 88% for the <5 mm margin group and 91% for the ≥5 mm margin group (p=0.033; HR=3.27; 95% CI=1.09–9.79, log-rank test, Fig. 3). Differences in OS and DSS were not evident when the cohort was divided at the 8-mm margin cut-off (Supplementary Fig. 7 and Fig. 4, respectively).
Fig. 3
DSS in patients with tumor-free surgical margins <5 mm (n=29) or ≥5 mm (n=85), following surgical treatment for stage IB/II (FIGO 2009) VSCC. Number of patients at risk is provided at the bottom of the figure. Log-rank test was used to compare survival curves among groups.
CI, confidence interval; DSS, disease-specific survival; FIGO, International Federation of Gynecology and Obstetrics; HR, hazard ratio; VSCC, vulvar squamous cell carcinoma.
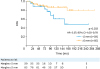
Fig. 4
DSS in patients with tumor-free surgical margins <8 mm (n=67) or ≥8 mm (n=47), following surgical treatment for stage IB/II (FIGO 2009) VSCC. Number of patients at risk is provided at the bottom of the figure. Log-rank test was used to compare survival curves among groups.
DSS, disease-specific survival; FIGO, International Federation of Gynecology and Obstetrics; VSCC, vulvar squamous cell carcinoma.
Patients with histopathological margins <5 mm, who developed at least one local vulvar recurrence had a 7-fold increase in mortality when compared to patients who also developed at least one local vulvar recurrence but had histopathological margins ≥5 mm (p=0.018, odds ratio [OR]=7.14; 95% CI=1.39–35.1, Fisher's exact test). The increased risk of mortality in patients with at least one local vulvar recurrence was not observed between groups at the 8 mm margin cut-off (p>0.99, Fisher's exact test). Clinical and pathological data comparison between groups at the 5 mm cut-off and 8 mm cut-off can be found in Table 1 and Supplementary Table 1, respectively.
Table 1
Clinical and pathological patient data
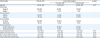
Values are presented as number (%) or median (range).
FIGO, International Federation of Gynecology and Obstetrics.
*Unpaired t-test; †Mann-Whitney test; ‡Refers to the number of lymph nodes resected bilaterally; §Refers to a vulvar cancerous lesion that developed following surgical treatment of the primary tumor.
DISCUSSION
Surgery is the cornerstone of treatment for primary VSCC [21222324] and for the treatment of loco-regional vulvar recurrences [212325], while VSCC prognosis is mainly determined by disease stage, lymph node status, age and tumor-related features [21]. Current data in the literature regarding a minimum oncologically safe margin distance, are contradictory [21]. In the case of early-stage, node-negative VSCC, there is limited knowledge on prognostic factors for recurrence and long-term survival. In this study, we show that tumor-free margin distance is clinically relevant from a treatment point of view, with a significant effect on prognosis. The data indicate that a histological margin of 5 mm is the minimum distance required to ensure oncological safety and long-term survival in patients with lymph node-negative, FIGO stage IB/II VSCC. Our data also indicate that margin distance has no significant impact on RR, in agreement with previous reports in the literature [11131526]. However, there is clear evidence that margin distance <5 mm has a significant impact on long-term survival, increasing VSCC mortality by a 3-fold, when compared with the ≥5 mm margin group. The median survival of patients that developed recurrences and died from vulvar cancer was 44 months, which illustrates the importance of long-term follow-up in VSCC patients.
It is commonly thought that node-negative VSCC has a good prognosis, with 5-year survival rates ranging from 70%–96% [242527]. In our study of 114 FIGO (2009) [19] stage IB/II VSCC patients, 5-year OS was 86% for the whole cohort, in agreement with the literature. However, survival changed dramatically when the sample was divided into groups according to tumor-free minimum margin distance <5 mm or ≥5 mm. Thus, the data indicate that surgical treatment of early-stage, node negative VSCC is not always curative and highlights the importance of surgical margins where approximately 1 in 4 patients with histological margins <5 mm will eventually die from VSCC.
Time from treatment to recurrence and the prognosis of a vulvar recurrences is influenced by the location of the local vulvar recurrence and not by the presence of lichen sclerosus within the surgical margin. Classification of recurrences was a difficult task, as there is no current consensus in the literature with regards to the definition of local VSCC recurrence or a ‘de novo’ tumor when considering: 1) the time elapsed from surgical treatment and 2) the location of the new lesion (i.e., adjacent to surgical scar vs. remote lesion vs. skin bridge lesion) [21]. Maggino et al. [28] defined a recurrence as a malignant lesion that develops at least 6 months following VSCC treatment with curative intent, while Preti et al. [29] defined it as a malignant lesion that develops 1 month following VSCC treatment. Most authors agree the majority of recurrences develop by 2 years following surgery while recurrences that develop after 2 years following primary treatment could be defined as ‘de novo’ tumors [325].
In our cohort, recurrence patterns differed significantly according to the location of the lesion with respects to the primary VSCC. Patients who present with ipsi-regional vulvar recurrences tend to develop earlier and more aggressive lesions when compared with the non ipsi-regional recurrence group. This observation was previously described by Rouzier et al. [30] in a cohort of 215 VSCC patients, although the study included different criteria of loco-regional distance from primary VSCC site, patients with mix stages, positive lymph nodes and positive margins.
The lack of difference in RR between margin groups at the 5-mm margin cut-off results puzzling in the face of such significant effect in survival. A possible explanation is that patients with smaller margin distances develop more aggressive recurrences. The notion of a ‘more aggressive’ recurrence affecting the <5 mm margin group is supported by our findings, as patients in the <5 mm margin group who developed a recurrence were 7 times more likely to die from VSCC when compared with patients who developed local recurrences in the ≥5 mm margin group. This is perhaps associated to the peri-tumoral stromal inflammation left in situ following the surgical removal of the tumor, which in time may contribute to the malignant progression of the remaining tissue [31] and to the development of local and metastatic disease [32].
To the best of our knowledge, this is the first report on the impact of margin distance on long-term survival in early-stage, node-negative VSCC. Although retrospective in nature, this study presents a homogenous patient sample, with similar VSCC prognoses and long-term clinical surveillance; a single surgeon performing all procedures in a single-center with a systematic and standardized staging of the groin [20] (i.e., total, bilateral lymphadenectomy) with histological confirmation of a negative node status. Thus, we believe this study provides robust evidence of the effect of margin distance on the long-term survival of patients with lymph node-negative, FIGO stage IB/II VSCC.
In conclusion, long-term patient survival in early-stage, lymph node negative VSCC is significantly affected by tumor-free margin distance at the 5-mm cut-off. Patients treated for early-stage VSCC with margins <5 mm have a significantly higher mortality than patients with larger tumor-free margin distance and should therefore be offered further surgical or adjuvant treatment. Future prospective studies are needed to identify optimal adjuvant treatments and to assess their effect on long-term survival in early-stage VSCC.
 XML Download
XML Download