

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The vast majority of malignant gastrointestinal tumors are adenocarcinoma. Gastrointestinal tumors demonstrating both exocrine and neuroendocrine differentiation are rare. Adenocarcinoma with neuroendocrine differentiation is diagnosed when neuroendocrine cells are scattered and intermixed with adenocarcinoma cells. Rarely, gastrointestinal tumors demonstrate both exocrine and neuroendocrine differentiation as a rare case of mixed neuroendocrine-nonneuroendocrine neoplasms (MiNENs). This group of tumors was named mixed adenoneuroendocrine carcinoma (MANEC) in the World Health Organization (WHO) 2010 classification and has been renamed as MiNEN in the WHO 2017 classification. In order to be classified as a MiNEN, a tumor must have at least 30% of a neuroendocrine component and at least 30% of a nonneuroendocrine component [1]. Nonneuroendocrine elements of the neoplasm may be of a different histologic grade and, by definition, both components are malignant. Owing to the complex histology of these tumors, the pathologic classification has been inconsistent in the literature. Typically, MiNENs involve the appendix, but have also been detected in the esophagus, stomach, duodenum, gallbladder, and colon [2]. MiNENs are further classified into 3 groups: 1) high-grade malignant (adenocarcinoma-neuroendocrine carcinoma), 2) intermediate-grade malignant (mixed adenocarcinoma-G1/G2 neuroendocrine tumor), 3) low-grade malignant (adenoma-G1/G2 neuroendocrine tumor). The grading scale for the neuroendocrine component depends on the Ki67 percentage and mitotic indices [1].
There is little clinical data on MiNENs as the disease is rare and has been difficult to characterize. As such, the biological behavior is difficult to predict and prognosis remains speculative [3]. Moreover, there is no published report on the genetic analysis of a trilineage MiNEN tumor. Although MiNEN has become an umbrella diagnosis, the spectrum of cases in the current literature encompasses a wide variety of histologies and phenotypes. Careful consideration should be given to each histologic component of MiNENs. Indeed, some reports suggest that MiNENs have more aggressive phenotypes than solitary neuroendocrine carcinomas or invasive adenocarcinomas [4]. We present the case of a unique patient with MiNEN and an additional squamous differentiation that underwent comprehensive genomic profiling and successful surgical and medical management.
CASE REPORT
A 56-year-old African American female was referred for esophagogastroduodenoscopy (EGD) after complaints of mid-epigastric pain and dark stools for 3 weeks. Her family history was notable for gastric cancer in her maternal grandmother and 4 aunts and breast cancer in her mother and 2 siblings. Social history was negative for tobacco and alcohol use.
EGD revealed a friable, ulcerated mass in the cardia of the stomach. Histologic examination of biopsy tissues revealed ulcerated gastric mucosa with malignant cells in a desmoplastic stroma, compatible with poorly differentiated invasive adenocarcinoma with a neuroendocrine carcinoma component. The patient was then referred to our academic medical center for further evaluation and treatment options. As such, she underwent staging with computed tomography (CT) scans that revealed the absence of metastatic disease in the chest and abdomen. Subsequently, the patient was referred for surgical intervention and she underwent total gastrectomy with Roux-en-Y esophagojejunostomy and D2 lymph node dissection. Final pathologic evaluation revealed a margin-negative 8×8×7 cm MiNEN with 3 histologic components (Fig. 1): large-cell neuroendocrine carcinoma (approximately 55%), squamous cell carcinoma (approximately 35%), and adenocarcinoma (approximately 15%). The 3 components demonstrated a collision tumor pattern, which was highlighted by immunohistochemistry. The neuroendocrine component stained positive for chromogranin and synaptophysin, the squamous cell carcinoma component stained positive for p63, and each component expressed a high proliferation index. The neuroendocrine component was large-cell neuroendocrine carcinoma with necrosis and high mitotic count, corroborated by a high proliferation index (Ki-67) of 80%. The squamous cell carcinoma was moderately differentiated and the adenocarcinoma was low-grade. The final pathologic stage was pT3N0 (37 examined lymph nodes). The tumor was further characterized as HER2-negative with intact nuclear expression of mismatch repair proteins. Additional pathologic findings included moderate chronic atrophic gastritis with diffuse pseudopyloric and intestinal metaplasia and neuroendocrine cell hyperplasia, suggestive of autoimmune gastritis. Representative samples from each histologic subtype were subsequently sent for comprehensive genomic profiling. Analysis of the genomic profile identified relevant genomic alterations from each histologic subtype (Table 1).
Fig. 1
Case pathology. (A) MiNEN with large-cell NEC, SCC, and AC in a collision tumor pattern (H&E, 20× magnification). (B) Synaptophysin immunohistochemical stain showing positive staining of the neuroendocrine component (20× magnification). (C) P63 immunohisotochemical stain showing positive staining of the squamous component (20× magnification). (D) Ki-67 immunohisotochemical stain demonstrating an overall high proliferation index (20× magnification; 152×116 mm [144×144 DPI]).
NEC = neuroendocrine carcinoma; SCC = squamous cell carcinoma; AC = adenocarcinoma; H&E = hematoxylin and eosin.
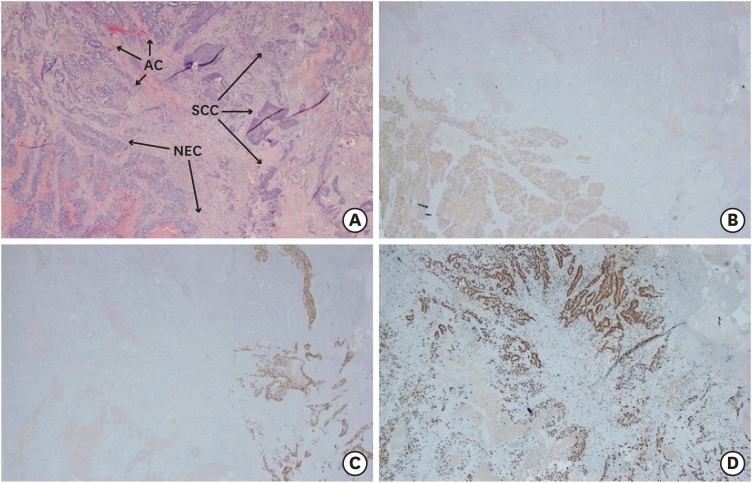
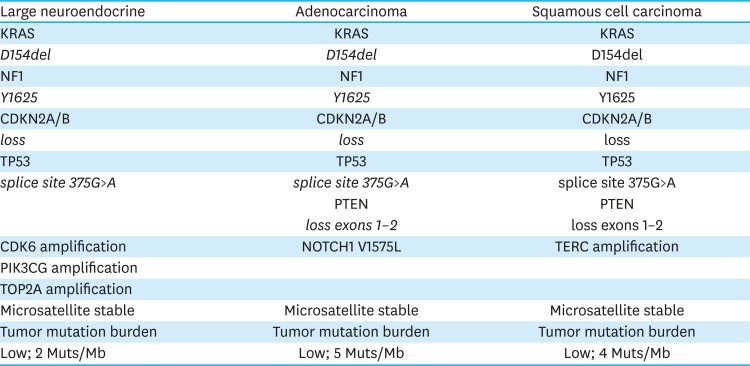
Table 1
Detected mutations in next-generation sequencing analysis by tumor type
The patient's case was discussed in a multidisciplinary tumor conference and the consensus recommendation was to offer 6 months of adjuvant chemotherapy based on the results of the CLASSIC trial [5]. She completed 12 cycles of chemotherapy with 5-fluorouracil, leucovorin, and oxaliplatin (modified FOLFOX 6) and tolerated the treatment except for grade I neuropathy. Surveillance CT imaging following systemic therapy did not reveal recurrent disease and patient is clinically doing well.
Methods for targeted next-generation sequencing (NGS)
Representative samples of each unique histologic component were referred for targeted comprehensive genomic profiling. All samples sent for analysis contained a minimum of 20% nuclei derived from tumor cells as assessed by histopathology. The analysis was performed using a clinical NGS-based assay (FoundationOne; Foundation Medicine Inc., Cambridge, MA, USA). The sequencing method was validated on a hybridization captured, adaptor ligation-based libraries using DNA extracted from ten formalin-fixed paraffin-embedded (FFPE) sections cut at 5 µm [2]. DNA sequencing was performed for 3,769 exons from 236 cancer-related genes and 47 introns from 19 genes commonly rearranged in cancer at an average sequencing depth of 1,153. This method was validated also for the detection of copy number alterations, including amplification and deletions, by a statistical model normalized to exonic coverage and allele frequencies. To maximize mutation-detection sensitivity in heterogeneous specimens, the test was validated to detect base substitutions as well as short insertions and deletions at a 10% mutant allele frequency with 99% sensitivity [6].
Sequence data were evaluated for genetic alterations (GAs) including point mutations, insertions and deletions, copy number alterations, and select gene fusions/rearrangements, as described previously [2]. A custom analysis was conducted as previously described [2]. NGS results were obtained from the patient's FoundationOne reports. Data on specific mutations were analyzed using publicly available tools, including Burrows-Wheeler aligner (http://bio-bwa.sourceforge.net/), Picard (http://broadinstitute.github.io/picard/), cBioPortal (http://www.cbioportal.org/), and TCGA (https://tcga-data.nci.nih.gov/tcga/tcgaHome2.jsp) [13]. The FoundationOne report included analysis of GAs seen in the tumor sample; annotation of the genomic alterations to existing therapies targeting either the GA or the signaling pathway (on the market or in development/trial stage); and suggestions for treatment were based on a review of the literature. The treatments suggested were not prioritized in order of clinical efficacy.
GAs were classified as “actionable” if they could be targeted with established US Food and Drug Administration (FDA)-approved therapies or investigational therapeutics, based on a literature review and a search of the clinical trial registry (http://clinicaltrials.gov/).
DISCUSSION
Little is known about gastric MiNENs and the existing reports are primarily from East Asian countries. Reports of MiNEN with squamous differentiation are exceedingly rare. Low incidence and variable histologic composition of these tumors preclude the creation of treatment guidelines and accurate prognosis [7]. In a recent retrospective report on gastric neuroendocrine neoplasms, 20 MiNENs were identified but none included cancers with squamous cell components. The median overall survival for this cohort was 5 months [8], which is far shorter than the current survival of our patient.
To our knowledge, there are only 5 reported cases of gastric MiNEN with squamous cell differentiation. Each of these cases exhibit a diverse clinical presentation with varied tumor behavior (Table 2) [910111213]. Three of these cases reported the development of liver metastases, all of which consisted only of the neuroendocrine component. This finding may suggest that pathogenesis and progression of these MiNENs depended primarily on the neuroendocrine component. In contrast, Bae et al. [13] reported MiNEN with metastatic disease in a lymph node consisting only of the adenocarcinoma component. In the fifth case report, no pathologic analysis was performed at the metastatic site. Our patient's gastric MiNEN did not exhibit regional or distant metastasis.
Table 2
Published cases of mixed neuroendocrine-nonneuroendocrine neoplasms with squamous cell carcinoma

| Author | Age | Sex | Site of metastasis: features |
|---|---|---|---|
| Shibuya et al. [9] | 54 | Male | Liver: atypical carcinoid |
| Haratake et al. [10] | 82 | Female | None |
| Pericleous et al. [11] | 81 | Male | Liver: neuroendocrine |
| Zhang et al. [12] | 68 | Male | Liver: neuroendocrine |
| Bae et al. [13] | 60 | Female | 14 of 48 regional lymph nodes: adenocarcinoma |
| Our patient | 56 | Female | None |
While the literature on the GAs of MiNEN neoplasms is sparse, treatment approaches have routinely involved surgical resection of the localized tumor followed by cytotoxic chemotherapy [57]. In most instances, patients have been treated for the histology that has the poorest prognosis, which is usually the adenocarcinoma. Adjuvant therapy for gastric cancer includes both systemic chemotherapy or chemoradiotherapy [514]. We based management of our patient on the results of the CLASSIC study, targeting the adenocarcinoma component with 6 months of mFOLFOX6 chemotherapy after surgical resection. Radiation therapy was not offered to our patient due to an absence of disease in the local and regional lymph nodes. This treatment approach is in accordance with the results of the 2015 ARTIST trial, which deemed no survival benefit for chemoradiotherapy in D2 node-negative gastric cancer [15].
The MiNEN in our patient harbored multiple alterations in genes that are established drivers of oncogenesis. The pathogenesis of MiNENs has been hypothesized to arise from either multipotent stem cells or arise independently from 2 similar but separate precursors. Kim et al. [16] performed chromosomal analysis of 8 cases of gastric MiNEN and identified that the MiNEN development was likely due to a common glandular precursor that gave rise to a heterogeneous adenocarcinoma with subsequent neuroendocrine differentiation. This model proposes that dual differentiation arises from a single precursor. Our genomic analysis data provides additional support to the hypothesis given genomic alterations in KRAS, NF1, CDKN2A, and TP53 are present in all 3 lineages. However, we noted that additional mutations were identified in the 3 distinct histologic subtypes. Furlan et al. [17] performed allelotyping of 2 gastric and 3 colonic mixed endocrine-exocrine tumors and reported a close genetic relationship between the 2 distinct histologic components, which also supports the hypothesis of a monoclonal mechanism of tumorigenesis.
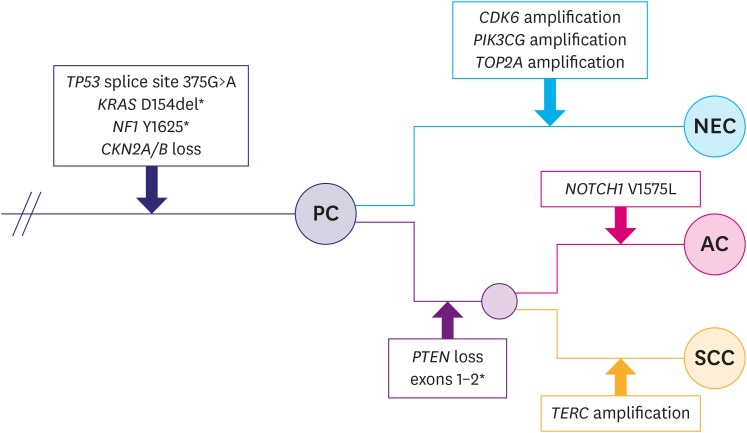
Much of the data attempting to explain the underlying genetic mechanism is hypothetical, but NGS that encompasses hundreds of mutations can help elucidate trends in GAs. Scardoni et al. [18] performed NGS of 6 gastroenteropancreatic MiNEN tumors and found common driver mutations in each of the 2 tumor components. Well-recognized mutations, such as mutations in p53 and KRAS, were present in both the neuroendocrine and adenocarcinoma components. We present a pathway for tumor differentiation based on the mutations discovered in our case (Fig. 2). Evolution of the MiNEN into different histologic subtypes follows a subtype-specific pattern. The neuroendocrine component contained both CDK6 and TOP2A amplification, which are commonly detected in carcinomas of neuroendocrine origin from various organ types [192021], while the squamous component contained an amplification in TERC, which is a common finding in squamous cell carcinoma with different tissues of origin [2223].
Fig. 2
A spatial relationship of the genomic alterations in each histologic component of the gastric MiNEN at our institution.
PC = primary clone; NEC = neuroendocrine carcinoma; AC = adenocarcinoma; SCC = squamous cell carcinoma.
*Mutations with identified treatment options.
The ultimate goal of NGS is to identify mutations to help guide therapy for patients [24]. In our analysis, there was no GA that could be targeted with an FDA-approved therapy for this tumor type. However, the neuroendocrine component did contain a CDK6 amplification, which may be targetable by small molecule CDK4/6 cell cycle inhibitors. In addition, mutations in either NF1 or PTEN have FDA-approved therapies in other tumor types. The neuroendocrine component of our case did not have a PTEN exon loss mutation. Everolimus is an mTOR inhibitor that is FDA approved for neuroendocrine tumors, and either inactivating mutations in PTEN or NF1 have predicted response to mTOR inhibitors in various tumor models [2526]. This continued collection of data from NGS has immense potential for guiding future treatments, but current treatment options are mostly in early stages. However, common mutations are guiding therapies and there are numerous clinical trials underway. Further, our analysis revealed multiple mutations that currently have undetermined significance. Further development of the database of mutations in such tumors will provide potential targets for future treatments.
In conclusion, we report a case of a 56-year-old female with a rare MiNEN tumor consisting large-cell neuroendocrine carcinoma, squamous cell carcinoma, and adenocarcinoma identified in the cardia of the stomach. MiNENs are highly variable in composition and, as such, have been poorly characterized in the literature. This case highlights a rare disease, in which a squamous cell carcinoma developed as a component of a MiNEN. The patient was treated with surgical resection followed by 6 months of adjuvant chemotherapy with FOLFOX and is currently disease-free. Moving forward, genomic analyses will likely play a key role in understanding the histogenesis of MiNEN tumors and will guide therapy.
 XML Download
XML Download