

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gastric cancer is one of the most common malignancies and an important cause of cancer-related death worldwide, especially in Eastern Asia [1]. Laparoscopy-assisted distal gastrectomy (LADG) was first introduced for the treatment of early gastric cancer (EGC) in 1994 [2]. The fourth edition of the Japanese Gastric Cancer Association (JGCA) guideline and the clinical practice guideline for gastric cancer of the Korean Academy of Medical Sciences consider LADG as a treatment option for clinical stage I cancer [34]. Recently, totally laparoscopic gastrectomy (TLG) has become a popular procedure for both distal and total gastrectomies for EGC, with several advantages over existing laparoscopy-assisted gastrectomy modalities in terms of improvement in the quality of life of patients, which is the purpose of minimally invasive surgery [5]. However, for advanced gastric cancer (AGC), some concerns still exist regarding the technical adequacy of lymph node dissection (LND), surgical outcomes, tumor implantation at trocar sites, and adverse effects of pneumoperitoneum during laparoscopic gastrectomy (LG), which is also a concern in EGC [6789]. A few retrospective studies have indicated the short-term feasibility of LADG for AGC, and prospective multicenter randomized clinical trials by Korean Laparoscopic Gastrointestinal Surgery Study (KLASS) group, Japanese Laparoscopic Surgery Study Group (JLSSG), and Chinese Laparoscopic Gastrointestinal Surgery Study (CLASS) group are in progress for demonstrating the long-term surgical outcome of LG for AGC [101112131415]. However, reports evaluating the long-term surgical outcomes and roles of pure TLG in AGC are scarce. Here, we report the long-term outcomes of TLG based on the consecutive performance by a single surgeon. We also indirectly evaluated the safety and oncologic feasibility of TLG for AGC by comparing them with those of TLG for EGC. Overall, this study aimed to demonstrate the oncologic feasibility and technical safety of TLG for AGC.
MATERIALS AND METHODS
Patients
From January 2011 to December 2016, 552 patients with pathologically proven gastric adenocarcinoma underwent TLG at our institute by a single surgeon who encountered more than 500 cases of open gastrectomy and 200 cases of LG since 2010. Of 552 patients, 12 who underwent neoadjuvant chemoradiotherapy or those who had a neoplasm of other organs were excluded. Another five patients (2 and 3 in the EGC and AGC groups, respectively) were also excluded because they switched to open conversion. Finally, a total of 535 patients were enrolled in the study and were divided into two groups (EGC [T1, n=375] and AGC (T2–4, n=160]) according to the clinical tumor, node, metastasis (TNM) staging of the seventh edition of the International Union Against Cancer. The clinical stage of each patient was determined by preoperative esophagogastroscopy and computed tomography. Surgical outcomes, including clinicopathological characteristics, number of retrieved lymph nodes, operation time, estimated blood loss, morbidity and mortality within 30 days after surgery, time-to-first oral intake, and length of postoperative hospital stay, were assessed from a prospectively collected database. Postoperative morbidity was classified according to the Clavien-Dindo (CD) classification [16], and complications over CD grade III were regarded as major complications. The study was approved by the Institutional Review Board of the Catholic University of Korea, College of Medicine (HC17RESI0091), and informed consent was obtained from the patients according to the Declaration of Helsinki.
Operating procedure
Five ports were used for TLG. Decisions regarding the extent of resection and lymphadenectomy complied with the JGCA treatment guidelines [3]. In totally laparoscopic distal gastrectomy, both delta-shaped gastroduodenostomy and gastrojejunostomy were performed intracorporeally using linear endostaplers. In totally laparoscopic total gastrectomy (TLTG), Roux-en-Y esophagojejunostomy was performed intracorporeally using linear endoscopic stapling devices. The specimen was retrieved via an umbilical port site extended to 2 cm.
Statistical analysis
Statistical analyses were performed using SPSS 18.0 (SPSS Inc., Chicago, IL, USA). The collected data are expressed as the mean±standard deviation for continuous variables and frequencies with percentages for nominal variables. The χ2 test or Fisher's exact test was used for nominal variables, and the Student's t-test was used for continuous variables. Overall survival (OS) was calculated from the time of the procedure to the date of death or date of the most recent follow-up. Survival curves were estimated using the Kaplan-Meier method. The χ2 tests, Fisher's exact tests, and Student's t-tests were all two sided. Statistical significance was set at P-values of <0.05.
RESULTS
There were no statistically significant differences between the patients from the EGC and AGC groups in terms of basic characteristics (sex, body mass index, and comorbidity), except for age (Table 1, EGC vs. AGC: 61.6±11.4 vs. 63.9±12.8 years, P=0.035). Almost all patients in the AGC group (n=153, 95.0%) underwent D2 LND, while 29.3% (n=110) of patients in the EGC group underwent D1+LND.
Table 1
Patient characteristics
In the EGC group, 55 (14.7%) patients had pathological stages higher than IA, while in the AGC group, 22 (13.8%) patients were diagnosed with stage IA cancer. There were significant differences between the EGC and AGC groups in terms of the operation time (EGC vs. AGC: 155 vs. 174 minutes, P<0.001), intraoperative blood loss (EGC vs. AGC: 58 vs. 99 mL, P<0.001), and total number of retrieved lymph nodes (EGC vs. AGC: 33 vs. 36, P=0.030). However, there was no significant difference in the time-to-first oral intake and postoperative hospital stay between the groups (Table 2).
Table 2
Operative outcomes

Overall, no significant difference was observed in the rates of morbidity and mortality 30 days after operation between the groups. In the EGC group, 50 cases (13.4%) of complications and 15 cases (4.0%) of morbidities exceeding CD grade III occurred. In the AGC group, 23 patients (14.3%) experienced short-term complications and 5 (3.1%) experienced major complications. All details of surgery-related major complications and their management are shown in Table 3. Intraluminal gastrojejunostomy bleeding occurred in both the groups and was successfully managed by endoscopic coagulation. In the EGC group, one case of leakage each in patients who underwent gastroduodenostomy and those who underwent esophagojejunostomy were managed by endoscopic stent insertion. Moreover, endoscopic stent insertion was used for the one case of leakage in esophagojejunostomy in the AGC group. One case of esophagojejunostomy stricture was managed by endoscopic dilatation, and one patient underwent Roux-en-Y jejunal bypass surgery owing to obstruction during jejunojejunostomy in the EGC group. Four patients in the EGC group experienced postoperative intraabdominal bleeding. Three of them required re-operation and one was conservatively managed. One patient in the EGC group underwent adhesiolysis because of small-bowel obstruction after TLTG, while 2 patients died within 30 days owing to cardiac arrest with sick sinus syndrome and pneumonia. Multivariate analysis of the risk factors for morbidity after TLG revealed that total gastrectomy and predisposing comorbidities were independent risk factors for postoperative morbidity (Table 4).
Table 3
Operation-related major complications by surgical procedure

Table 4
Univariate and multivariate analyses for morbidity

Adjuvant chemotherapy was administered to 54.3% (n=87) of patients in the AGC group. Most of them (n=85, 53.1%) received S-1 (tegafur, gimeracil, and oteracil). One patient (0.6%) each received FOLFOX (fluorouracil, oxaliplatin, and leucovorin) and cisplatin with S-1. The median follow-up period in the AGC group was 31 (range, 2–74) months. In the AGC group, the 3-year OS rate was 80.5% and the 3-year disease-free survival (DFS) rate was 73.7%. The 3-year overall and DFS rates were 89.0% and 88.4%, respectively, for stage I; 89.4% and 85.7%, respectively, for stage II; and 56.6% and 45.2%, respectively, for stage III (Fig. 1). Advanced T and N stages were risk factors for DFS (Table 5). In total, 29 (18.1%) patients experienced recurrence during the follow-up period. Peritoneal recurrence was the most common and was observed in 13 patients (8.1%). Eight (5.0%), four (2.5%), two (1.3%), one (0.6%), and one (0.6%) patient(s) were diagnosed with recurrence in the liver, lymph node, lung, remnant stomach, and esophagojejunal anastomosis, respectively.
Fig. 1
Kaplan-Meier survival curves of patients with AGC according to different tumor stages. (A) Cumulative OS; (B) Cumulative DFS.
AGC = advanced gastric cancer; OS = overall survival; DFS = disease-free survival.
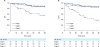
Table 5
Univariate and multivariate analyses for DFS in patients with AGC

DISCUSSION
For EGC, LG has been proven to have acceptable short- and long-term outcomes in many published studies [17–19]. However, the application of LG for AGC remains controversial because of the technical difficulty in performing complete D2 LND, which is the essential procedure for achieving R0 resection. In East Asia, the KLASS group, JLSSG, and CLASS group launched multicenter randomized clinical trials to compare the efficacy of laparoscopic subtotal gastrectomy with open gastrectomy in patients with locally AGC, and their long-term results are still pending [111415]. Recently, TLG has attracted attention in the treatment of EGC owing to its low invasiveness. However, the oncologic adequacy of TLG has not been proven owing to the lack of data; more randomized studies with sufficient follow-up periods are required to validate TLG as a standard treatment option in EGC and even AGC. In this study, we indirectly attempted to prove the technical safety of TLG and the feasibility of D2 LND for AGC by comparing their outcomes with those of EGC. To the best of our knowledge, this it is the first retrospective study that includes the largest amount of data regarding short-term outcomes of TLG for AGC.
The major concern regarding TLG for AGC is the performance of adequate LND up to the level of D2 and concerns about the morbidity following this radical LND. In contrast with EGC, a large primary tumor and multiple bulky positive lymph nodes were observed in our study, and total omentectomy was almost mandatory in AGC. Moreover, caution should be exercised while handling the stomach and lymph nodes in AGC because of the risk of tumor spread. Considering these aspects, the longer operation time and greater blood loss noted in TLG for AGC, compared to those in TLG for EGC, was not unexpected, and the morbidity in patients with AGC might be higher than that in patients with EGC. Although our results confirmed our expectations regarding longer operation times and more blood loss in patients with AGC than in those with EGC, oncologically adequate lymph nodes were harvested without an increase in postoperative morbidity and mortality. In our study, relatively large tumor sizes and multiple positive nodes were observed in the AGC group; however, they were not negative prognostic factors of morbidity. As shown in Table 4, an analysis of risk factors for morbidity according to the number of retrieved lymph nodes suggested that patients whose harvested lymph nodes exceeded 40 had a higher possibility of morbidity in univariate analysis. However, the number of retrieved lymph nodes did not influence morbidity following multivariate analysis.
According to the fourth treatment guidelines of JGCA [3], total omentectomy is a mandatory procedure for the treatment of patients with ≥stage T3 gastric cancer. Our study strictly followed this principle, and bursectomy was selectively performed in patients with clinical stage T4 gastric cancer; 75 (46.9%) patients with AGC underwent total omentectomy. However, currently, bursectomy is not recommended as a standard procedure for AGC [20]. Although it is a time-consuming task, laparoscopic total omentectomy is not impossible for experienced surgeons, and it seems necessary for avoiding possible extranodal expansion of cancer cells to adjacent adipose tissues [21]. Altogether, in addition to not being a negative prognostic factor for morbidity, a reasonably longer operation time seems to be acceptable for AGC.
Regarding morbidity, the incidence of major and minor complications was similar in both groups. Although more lymph nodes were dissected and more intraoperative blood loss occurred in AGC, short-term surgical outcomes including morbidity, time-to-oral intake, and postoperative hospital stay were similar in both groups. This implies that the application of TLG might be safe for AGC, as for EGC, from the perspective of short-term outcomes.
In a recent multicenter randomized study that evaluated the feasibility of LADG for AGC, the 3-year DFS rate was 81.9% in the open gastrectomy group and 80.1%, in the LADG group [22]. Moreover, Sakuramoto et al. [23] reported the survival rates of patients with AGC who received adjuvant S-1 after curative gastrectomy; their 3-year overall and DFS rates were 80.1% and 72.2%, respectively. Our study showed similar results, with 3-year overall and DFS rates of 80.5% and 73.7%, respectively.
TLTG is more challenging for proximal than for distal cancer. First, splenic hilar dissection should be performed as a standard D2 LND for proximal AGC. However, laparoscopic splenic hilar LND is a technically challenging and time-consuming procedure even for skilled surgeons. Therefore, some surgeons prefer splenectomy to splenic hilar LND. Moreover, there are debates regarding the feasibility of laparoscopic spleen-preserving splenic hilar LND and splenectomy [242526]. As there was no definite indication for splenectomy in our study, splenic hilar dissection was mostly performed with spleen preservation. Second, there are technical difficulties associated with intracorporeal esophagojejunostomy. In total, 30 and 16 patients underwent TLTG in the EGC and AGC groups, respectively. Moreover, as shown in Table 3, anastomotic complications were more frequent in total gastrectomy than in subtotal gastrectomy. There was one esophagojejunostomy leakage each in both groups and two esophagojejunostomy strictures in the EGC group. The incidence of anastomosis leakage and stricture was 4.3% each in this study. Inokuchi et al. [27] systematically reviewed the anastomotic complications of various laparoscopic procedures for esophagojejunostomy. The incidence of leakage ranged from 1.1% to 3.2% and the incidence of stenosis ranged from 1.0% to 8.8%. Although the interpretation of our results may be limited because of the relatively small number of patients, our results are similar to these results.
The present study has some limitations in that it was retrospective, and a comparison with open gastrectomy was not performed. In addition, there was an issue of the surgical learning curve of TLG; sufficient experience for TLG could not be achieved in the early study period. In 2011, 21.2% of the patients enrolled in the study had AGC; this percentage gradually increased to 31.2% in 2012 and 38.9% in 2013. Therefore, the acceptable surgical outcomes in patients AGC could be attributed to the extensive experience of the surgeon. Moreover, as detailed information about harvested lymph nodes was not obtained, noncompliance rates of LND could not be assessed; this is an objective and reproducible method to demonstrate short-term oncological outcomes for gastrectomy with LND in patients with gastric cancer [22]. Our results should be carefully considered because the follow-up period seemed insufficient and there was a selection bias in our study. The long-term oncologic feasibility of TLG needs to be clarified by well-designed randomized studies with a reasonable follow-up period.
In conclusion, TLG is safe for AGC, as for EGC, especially for patients without comorbidities, whose tumors are limited to the distal stomach. TLG is also feasible for harvesting perigastric lymph nodes; however, the definite long-term oncologic feasibility of this procedure must be proven in further studies.
 XML Download
XML Download