

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Dear Editor,
Kerstersia gyiorum is a pathogen that is infrequently reported in humans [1]. This bacterium, first classified in 2003, is a gram-negative coccobacillus belonging to the family Alcaligenaceae, which is isolated from water, soil, animal, and human specimens [23]. Although some cases of K. gyiorum infection have been reported worldwide [45678], none to date have been reported in Korea. We report the first case of chronic otitis media (COM) due to K. gyiorum infection in Korea.
A 51-year-old female patient visited the otolaryngology department of Hanyang University Seoul Hospital with otorrhea in the left ear, which had started several weeks earlier. At the age of 25 and 28 years, she underwent canal wall-down mastoidectomies type III tympanoplasty of the right and left ears, respectively. On the day of admission, ear endoscopy revealed a purulent discharge and crust in the left external ear canal; therefore, the patient received crust removal and cefpodoxime treatment.
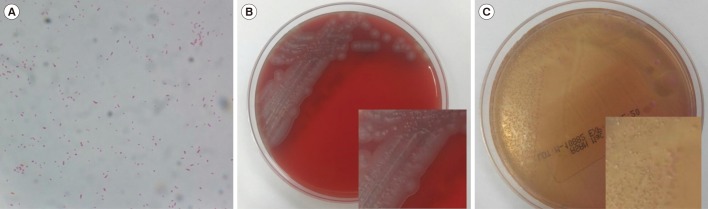
A swab specimen was taken from the patient's ear discharge and analyzed by bacterial culture and Gram staining. Gram staining revealed gram-negative coccobacilli in singles, pairs, and short chains (Fig. 1A). The specimen was inoculated on 5% sheep blood agar and MacConkey agar. After 24 hours, colonies of the organism grew on both sheep blood agar and MacConkey agar at 35℃ under 5% CO2 (Fig. 1B and 1C). The colonies were gray and displayed spreading edges; colony isolates were oxidase negative and catalase positive. Isolates were examined using the MicroScan Walkaway (Beckman Coulter, Brea, CA, USA) and VITEK 2 (bioMérieux, Marcy-I'Etoile, France) automated bacterial identification systems; however, both analyses failed to identify the bacterial species. The species was identified as K. gyiorum by matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS) with a MALDI Biotyper using MALDI-Biotyper software (version 2.3, Bruker Daltonics, Bremen, Germany). 16S ribosomal RNA gene sequencing was performed using primers 27F (5′-AGAGTTTGATCCTGGCTCAG-3′) and 1492R (5′-GGTTACCTTGTTACGACTT-3′) as described previously [1]. We obtained a consensus sequence of 1,394 bp, which was 99.9% identical to K. gyiorum LMG 5906 (GenBank accession number AY131213). The next-nearest match was K. similis LMG 5890 (GenBank accession number AY131212), with 99.4% homology. In addition, gyrB gene sequencing was performed as described previously [4]. The gyrB gene sequence was 98.6% and 96.9% identical to K. gyiorum LMG 5906 (GenBank accession number HE585644) and K. similis LMG 5890 (GenBank accession number HE585647), respectively.
The results of the antimicrobial susceptibility test performed with the MicroScan Walkaway system were assessed according to the Clinical and Laboratory Standards Institute (CLSI) minimum inhibitory concentration (MIC) standards for other non-Enterobacteriaceae [9]. The isolate was susceptible to amikacin (MIC ≤16 µg/mL), aztreonam (≤4 µg/mL), cefepime (≤2 µg/mL), cefotaxime (≤1 µg/mL), ceftazidime (≤1 µg/mL), gentamicin (≤4 µg/mL), imipenem (≤1 µg/mL), levofloxacin (≤2 µg/mL), meropenem (≤1 µg/mL), piperacillin-tazobactam (≤16 µg/mL), piperacillin (≤16 µg/mL), ticarcillin-clavulanate (≤16 µg/mL), tobramycin (≤4 µg/mL), and trimethoprim-sulfamethoxazole (≤2/38 µg/mL) and was resistant to ciprofloxacin (>2 µg/mL).
A week after the initial visit, the antibiotic administered was changed to cefcapene and continued for six days; four weeks later, the patient's ear discharge symptoms were resolved with no other complications.
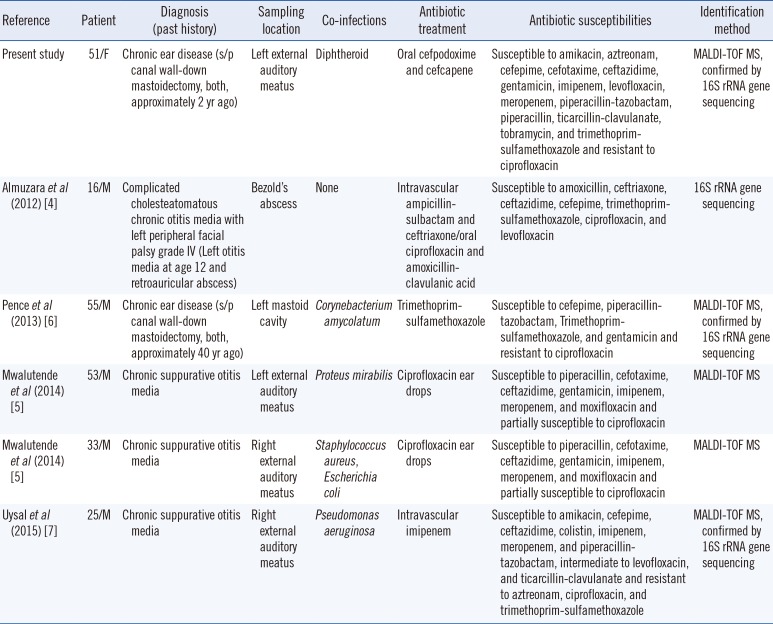
K. gyiorum has been isolated from patients with various diseases [1]. A total of 10 cases of patients infected with K. gyiorum have been recorded, five of which were associated with COM; the features of these cases are shown in Table 1 [4567]. Four of the five patients showed co-infection, which is a common feature of COM [10]; likewise, a diphtheroid was isolated from our patient with K. gyiorum who developed an infection at the site of operation approximately 25 years after undergoing surgery for COM.
It is difficult to distinguish K. gyiorum from other microorganisms using biochemical methods as it has characteristics similar to those of other microorganisms [4]. Additionally, K. gyiorum is not accurately identified by automated bacterial identification methods such as MicroScan Walkaway, Vitek 2, API 20 NE (bioMérieux), and the RapID NF plus assay (Thermo Fisher Scientific, Lenexa, KS, USA) [45678]. MALDI-TOF MS, which has recently been widely used in clinical laboratories, identified K. gyiorum, both in our case and in previously reported cases [5678]. Therefore, MALDI-TOF MS should be used when bacterial species identification is difficult using conventional methods. In addition, the clinician and laboratory should consider the possibility of K. gyiorum infection and the use of MALDI-TOF MS when inaccurate identification of pathogen is suspected in patients with COM.
 XML Download
XML Download