

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The incidence, predictors and prognosis of high-degree (second- and third-degree) atrioventricular block (HAVB) complicating ST-segment elevation myocardial infarction (STEMI) were investigated by several previous studies, which reported that HAVB was associated with increased short-term mortality in patients with anterior or inferior myocardial infarction (MI).1)2)3) However, most trials were carried out in the prethrombolytic or thrombolytic era. To our knowledge, only one study evaluated the incidence, predictors and prognosis of HAVB complicating STEMI in the era of primary percutaneous coronary intervention (PCI). This study enrolled 2073 patients and evaluated the prognostic value of HAVB in STEMI patients treated with primary PCI. Despite improvements in reperfusion strategy, HAVB remains a significant adverse prognostic factor in the era of primary PCI.4) The impact of HAVB complicating STEMI on short-term mortality was prominent regardless of infarct location in the thrombolytic era. In patients with inferior infarction treated with thrombolysis, the increase in mortality was apparent.1)2)3)5)6)7)8) The increase in mortality was more prominent in anterior infarction than inferior infarction. The more extensive infarction area and higher incidence of hemodynamic compromise help to explain the poorer outcome in anterior infarction.1)2) However, although most patients with acute MI are currently treated with PCI, no study has evaluated the differential prognostic impact of HAVB complicating STEMI according to infarct location in the era of primary PCI. Therefore, we investigated the incidence, predictors and prognosis of HAVB in patients with either anterior or inferior infarction who were treated with primary PCI.
Subjects and Methods
Study population
From November 2005 to January 2012, 36580 patients with acute MI were registered in the Korea Acute Myocardial Infarction Registry (KAMIR).The KAMIR is a multi-center observational registry designed to collect the demographic and angiographic features of patients with acute MI and record cardiovascular outcomes. This trial was supported by a research grant from the Korean Society of Cardiology; the protocol of this trial was evaluated and recognized by the ethics committee at each hospital.
STEMI is characterized by symptoms of MI in association with persistent electrocardiographic ST-elevation and subsequent release of biomarkers of myocardial necrosis.9) Diagnostic ST-elevation was defined as new ST-elevation at the J point in at least 2 contiguous leads of ≥2 mm (0.2 mV) in men or ≥1.5 mm (0.15 mV) in women in leads V2-V3 and/or of ≥1 mm (0.1 mV) in other contiguous chest leads or the limb leads.10) New or presumably new left bundle branch block was recognized as a STEMI equivalent.
All STEMI patients in the KAMIR registry treated with primary PCI were included in this study. The exclusion criteria of this study were as follows: 1) non ST-segment elevation myocardial infarction, 2) treatment with thrombolysis, 3) not having undergone primary PCI, 4) missing records about the location of infarct, and 5) lack of significant coronary artery stenosis on angiography and MI due to coronary artery spasm. After excluding these patients, 9354 patients with STEMI on the anterior wall and 7692 patients with STEMI on the posterior wall were enrolled in this analysis. The location of infarction was determined based on the location of ST-segment elevation on electrocardiogram and culprit lesion on angiography.
High-degree atrioventricular (AV) block in this study is defined as second- or third-degree AV block.
Procedure and medication
PCI was performed based on local standard protocol and the selection between pre-dilatation and direct stenting was chosen by the surgeon. For all enrolled patients, primary PCI was done with the intention of recovering blood flow to the target vessel as soon as possible. The diameter and length of stent used was determined based on the characteristics of the lesion on angiography. In cases with significant stenosis in multiple vessels, the selection between staged PCI and one-stage PCI was done according to the treatment team's consensus. Other procedures, such as temporary pacing, intra-aortic balloon pump or extracorporeal membrane oxygenation, were also performed based on the clinical decision of the treatment team.
Anticoagulation agents such as unfractionated low molecular weight heparin or glycoprotein IIb/IIIa inhibitor were administered as directed by the clinician. Medications such as anti-platelet agents, renin-angiotensin system blockers, beta-blockers, statins, or aldosterone antagonists in hospital or at discharge were given based on the clinical status of patients.
Study end point and statistical analysis
Because the mechanism and prognosis of HAVB in acute MI were known to be different according to the location of infarction, all analyses were performed for anterior and inferior infarction separately. Incidence, predictors, and in-hospital mortality were evaluated. The cumulative all-cause death for 2 years was compared between patients with HAVB and those without HAVB among in-hospital survivors. Categorical baseline characteristics are presented as counts and percentages and continuous variables are presented as average value±standard deviation. Continuous baseline characteristics were compared and evaluated by Student's t-test and categorical baseline variables were compared by Pearson chi-square test. The hazard ratio (HR) of in-hospital mortality between patients with and without HAVB was calculated using a binary logistic regression model. Multivariate logistic regression analysis was performed to clarify the independent factors which influence the incidence of HAVB in patients with STEMI. The variables available in this analysis were the following: old age (≥65 years), gender, low systolic blood pressure (<90 mmHg), Killip classification on presentation (≥Class II), previous history of hypertension and diabetes mellitus, complexity of culprit lesion (Type C), pre-Thrombolysis In Myocardial Infarction (TIMI) flow (0 or 1), decreased left ventricular ejection fraction (LVEF), and smoking. For in-hospital mortality, the presence of HAVB was also included as a co-variant in the multivariate analysis.
The long-term survival rate of in-hospital survivors was evaluated by a life table scale and compared using the Wilcoxon method. The HR of HAVB in anterior or inferior STEMI was calculated by Cox-regression analysis. HR and 95% confidence interval (CI) were calculated and all tests were two-tailed. p<0.05 was considered significant. All analyses were performed using SPSS Version 21 (SPSS Inc., Chicago, IL, USA).
Results
Incidence and baseline characteristics
The overall incidence of HAVB was 3.2% (546/17046) in patients with STEMI treated with primary PCI. Among the 546 patients, 274 patients had second-degree AV block and 158 patients had third-degree AV block. The severity of AV block in the remaining 114 patients was unspecified.
The incidence rate of HAVB was significantly higher in patients with inferior wall STEMI (510/7692, 6.6%) than in those with anterior wall STEMI (36/9354, 0.3%) (HR: 18.380, 95% CI: 13.090-25.807, p<0.001). Comparisons of demographic and clinical baseline characteristics between patients with and without HAVB in anterior and inferior wall STEMI showed that many baseline variables were different between the two groups being compared (Table 1). Angiographic and procedural characteristics were also different (Table 2).
Table 1
Comparison of clinical baseline characteristics

Data are expressed as mean±standard deviation or number (%). HAVB: high-degree atrioventricular block, IHD: ischemic heart disease, Hx.: history, HTN: hypertension, DM: diabetes mellitus, HL: hyperlipidemia, SBP: systolic blood pressure, DBP: diastolic blood pressure, LVEF: left ventricular ejection fraction, CK-MB: creatinine kinase-MB, HDL-C: high-density lipoprotein cholesterol, LDL-C: low-density lipoprotein cholesterol, Hs CRP: high sensitive C-reactive protein, NT pro BNP: N-terminal pro B type natriuretic peptide, GP: glycoprotein, LMWH: low molecular weight heparin, RAS: renin-angiotensin system
![]()
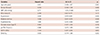
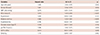
Table 2
Comparison of coronary angiographic and procedural characteristics

Data are expressed as number (%). HAVB: high-degree atrioventricular block, LM: left main, LAD: left anterior descending, LCX: left circumflex, RCA: right coronary artery, TIMI: thrombolysis in myocardial infarction, BMS: bare metal stent, DES: drug eluting stent
![]()
Predictors of high-degree atrioventricular block
To investigate the predictors for HAVB in STEMI patients, we performed multivariate regression analyses. In the analysis of the population with anterior wall STEMI, low systolic blood pressure (<90 mmHg) was independently associated with development of HAVB (Table 3). The analysis of patients with inferior wall infarction showed somewhat different result. In this analysis, old age, female gender, low systolic blood pressure (SBP) (<90 mmHg), Killip classification (II, III, IV), diabetes mellitus, and pre-TIMI flow (0, 1) were independent factors for the development of HAVB (Table 4).
Table 3
Multivariate analysis for predictors of high-degree atrioventricular block in patients with anterior ST-segment elevation myocardial infarction
CI: confidence interval, SBP: systolic blood pressure, TIMI: thrombolysis in myocardial infarction, LVEF: left ventricular ejection fraction
![]()
Table 4
Multivariate analysis for predictors of high-degree atrioventricular block in inferior ST-segment elevation myocardial infarction
CI: confidence interval, SBP: systolic blood pressure, TIMI: thrombolysis in myocardial infarction, LVEF: left ventricular ejection fraction
![]()
In-hospital and long-term mortality
Among 36 patients with HAVB complicating STEMI on the anterior wall, 13 patients died in the hospital and 23 patients were alive at discharge. During the follow-up period, 3 patients died.
For 510 patients with HAVB caused by inferior wall STEMI, 54 patients died in the hospital and 9 patients died after discharge.
In the population with anterior wall infarction, the in-hospital mortality of STEMI patients with HAVB was higher than that of patients without HAVB (HR=9.821, 95% CI: 4.946-19.503, p<0.001). Although the magnitude of the hazard ratio was relatively small, the result was similar in patients with inferior wall STEMI (HR=2.819, 95% CI: 2.076-3.827, p<0.001). In patients with HAVB complicating STEMI, patients with anterior wall infarction showed higher in-hospital mortality than those with inferior wall infarction (HR=4.742, 95% CI: 2.271-9.901, p<0.001) (Fig. 1).
 | Fig. 1Comparison of in-hospital mortality between patients with and without HAVB in anterior and inferior STEMI. HAVB: high-degree atrioventricular block, STEMI: ST-segment elevation myocardial infarction, HR: hazard ratio.
|
Among in-hospital survivors, long-term cumulative all-cause mortality was compared between patients with and without HAVB in anterior or inferior wall STEMI. In the population with anterior wall STEMI, survival analysis showed that patients with HAVB had a higher rate of all-cause death than those without HAVB (HR=5.454, 95% CI: 1.746-17.033, p=0.004). In patients with inferior wall STEMI, there was no significant difference in long-term survival between the two groups (Fig. 2).
 | Fig. 2Comparison of cumulative long-term all-cause survival between patients with and without HAVB in anterior (A) and inferior (B) STEMI among in-hospital survivors. HAVB: high-degree atrioventricular block, STEMI: ST-segment elevation myocardial infarction, HR: hazard ratio, CI: confidence interval.
|
Multivariate analysis
Multivariate logistic regression analysis was carried out in order to clarify the impact of HAVB on in-hospital mortality in STEMI patients.. In the population with anterior wall STEMI, HAVB was significantly associated with increased in-hospital mortality (HR=19.264, 95% CI: 5.804-63.936, p<0.001). Other factors such as old age, low systolic blood pressure, Killip classification, pre-TIMI flow and low LVEF were also associated with in-hospital mortality (Fig. 3). In patients with inferior wall infarction, HAVB was not independently associated with in-hospital mortality (HR=1.104, 95% CI: 0.547-1.985, p=0.901). Old age, low systolic blood pressure, Killip classification, diabetes mellitus, and low LVEF were independently associated with increased in-hospital mortality (Fig. 4).
 | Fig. 3Multivariate logistic regression analysis for in-hospital mortality in patients with anterior STEMI. STEMI: ST-segment elevation myocardial infarction, HAVB: hgh-degree atrioventricular block, LVEF: left ventricular ejection fraction, TIMI: thrombolysis in myocardial infarction, SBP: systolic blood pressure, HR: hazard ratio, CI: confidence interval.
|
 | Fig. 4Multivariate logistic regression analysis for in-hospital mortality in patients with inferior STEMI. STEMI: ST-segment elevation myocardial infarction, HAVB: high-degree atrioventricular block, LVEF: left ventricular ejection fraction, TIMI: thrombolysis in myocardial infarction, SBP: systolic blood pressure, HR: hazard ratio, CI: confidence interval.
|
Discussion
This study revealed that HAVB in patients with inferior wall STEMI is not independently associated with increased in-hospital mortality in the era of primary PCI. Because of improvements in reperfusion strategy and medical devices, the adverse prognostic impact of HAVB in inferior STEMI has been reduced.
Several previous studies revealed that thrombolytic therapy increases the rate of HAVB.5)11) However, Gang et al4) reported that the incidence is reduced in the era of primary PCI; our study agrees with that conclusion by finding a similar rate of HAVB.Other studies reported that the overall incidence of HAVB was 7 to 10 percent in the era of thrombolysis.2)12) These studies reported that HAVB occurred in approximately 3.2% in anterior MI and 9.8% in inferior MI when patients were treated with thrombolysis. However, no previous study examined the incidence of HAVB according to the location of infarct in the era of primary PCI. In our study, the rate of HAVB was 0.3% in anterior MI and 6.6% in inferior MI. Improvements in reperfusion strategy have markedly reduced the incidence of HAVB in patients with anterior wall STEMI. Primary PCI as the standard therapy for STEMI has reduced the risk of extensive necrosis involving the conduction system. On the other hand, the reduction in the incidence of HAVB in inferior infarction was modest in our study.
The mechanism of conduction disturbance in MI is different according to the location of infarction. HAVB in anterior MI is thought to result from extensive myocardial damage affecting the bundle branch traveling within the interventricular septum. Therefore, HAVB with anterior MI is often preceded by bundle branch block, rendering the escape rhythm unstable.13) Conduction disturbance in inferior MI occurs more frequently, since the atrioventricular node is mainly supplied by the right coronary artery (RCA).14) Occlusion of the RCA increases acetylcholine release from the inferoposterior myocardium and makes the AV node hypersensitive to acetylcholine. HAVB in inferior MI is usually transient and benign, resolving within five to seven days.
Gang et al4) reported that RCA culprit lesion, old age, female gender, hypertension, and diabetes are important factors that contribute to the development of HAVB in all STEMI patients treated with primary PCI. However, because of different mechanisms of conduction disturbance according to location, we thought that the predictors for HAVB may be different in anterior vs. inferior MI. Multivariate analysis in the population with anterior STEMI revealed that low SBP (<90 mmHg) is independently associated with the development of HAVB. In this analysis, old age, gender, hypertension, and diabetes did not have a significant impact on the occurrence of HAVB. The analysis in patients with inferior STEMI showed that old age, gender, diabetes mellitus, low SBP, Killip classification and pre-TIMI flow are independent contributors that increase the rate of HAVB. Thus, we demonstrate that the predictors for development of HAVB are different according to the location of infarction in the era of primary PCI.
The prognostic value of HAVB in MI was demonstrated in several studies which were conducted in prethrombolytic or thrombolytic therapy. These studies reported that HAVB was associated with an increase in short-term mortality in patients with acute MI.1)2)3) Although HAVB in patients with inferior MI is usually transient, the increase in in-hospital mortality was prominent in patients with inferior STEMI in the prethrombolytic and thrombolytic eras.1)2)3)5)6)7)15)16)17)18) Several trials reported that HAVB in patients with anterior wall MI causes a greater increase in in-hospital and 30-day mortality than in patients with inferior wall infarction.1) This increase in mortality was demonstrated in a systemic review of four randomized trials.2) A trial conducted in STEMI patients treated with primary PCI revealed that patients with HAVB had a significantly higher 30-day mortality compared to patients without HAVB. In this study, HAVB independently contributed to an increase in short-term mortality.4) However, this trial analyzed all patients with STEMI and did not divide the patients according to the location of infarct. In our study, patients with HAVB had higher in-hospital mortality than those without HAVB regardless of location of infarction. However, in multivariate analyses, HAVB was not significantly associated with higher in-hospital mortality in patients with STEMI on the inferior wall. In this analysis, old age, diabetes mellitus, pre-TIMI flow, low SBP, and Killip classification were important factors that determined short-term clinical outcome. Because these factors were more frequent in patients with HAVB, these patients had a higher mortality rate than those without HAVB.
The impact of HAVB on long-term mortality was questionable. In the studies conducted in the thrombolytic era, an increase in long-mortality was not apparent in patients with HAVB among 30-day survivors.2)3) Investigations in the era of primary PCI also revealed that the rate of long-term mortality was not different according to the presence of HAVB among in-hospital survivors.4) In our study, HAVB did not have a significant impact on long-term outcome in patients with inferior STEMI. However, although the number of patients analyzed was small, patents with HAVB had higher cumulative long-term mortality compared with patients without HAVB in the population with anterior STEMI. To fully understand the impact of HAVB in patients with anterior STEMI, it is necessary to perform a larger-scaled study.
This study has several limitations. First, a substantial number of records did not include information about the type of HAVB. The types of HAVB in 114 patients were not specified and the subtype of second-degree AV block was omitted in this registry. Second, although many important variables were included in the multivariate analyses, we cannot confirm that optimal adjustment was done in the multivariate logistic regression. Third, although all HAVB cases were documented during hospitalization, the registry had incomplete data on the timing of the development of HAVB. Fourth, the frequency of use of temporary or permanent pacemakers was not recorded.
Conclusion
Because of the development of better reperfusion strategies, the incidence of HAVB has been reduced. As primary PCI became a standard treatment method, the clinical implication of HAVB complicating STEMI changed. In particular, the development of HAVB in patients with inferior STEMI is not independently associated with increased in-hospital mortality in the era of primary PCI. Additionally, the impact of HAVB in patients with STEMI on long-term mortality is different according to the location of infarct.
 XML Download
XML Download