

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Conventional orthodontic treatments using fixed appliances bonded to the labial surface of the teeth are less esthetic which is a drawback of labial orthodontic systems. In contrast, lingual orthodontic systems are more acceptable to adult patients because they do not affect their social life.12
Lingual straight-wire systems have many advantages because arch coordination can be achieved easily by using sliding mechanics.3 However, tooth configuration on the lingual side has many variations and adapting a straight wire to the lingual curves requires composite resin compensation on the base of the brackets.4 In addition, incorrect positioning of brackets in lingual straight-wire systems can cause undesired rotation, tipping, linguoversion/buccoversion, intrusion/extrusion, and torque.5 In lingual orthodontics, several factors including limited access, variable lingual morphology (especially of the anterior maxillary teeth), shorter clinical crown compared to the labial aspects, large labiolingual thickness of the crown, inclination of the lingual surface, and tongue and opposing tooth interferences could influence bracket positioning.6 Owing to the complicated lingual morphology of the anterior teeth, even slight deviations in bracket position can cause large and unpredicted changes in torque and vertical positioning of the teeth.7 Complicated and unpredictable tooth movements in lingual orthodontics are results of bracket positioning and initial tooth positions.8 Therefore, to ensure the least possible error in bracket positioning, it is better to first examine the shortest distance that the wire has from the teeth in any given position for bracket bonding. Furthermore, the compensation needed inside the angulation of the slot to the base has to be estimated to produce similar treatment results. Thus, compensations of composite resin at the base of the brackets should be minimized for insertion of a straight wire in the bracket slots.
In previous studies, lingual brackets were placed at the mid-lingual surface of the teeth.8910 However, in some of the lingual systems, placing brackets in a more gingival position would allow the possibility of using straight wires in lingual orthodontics.1112 Nevertheless, comparisons between these two bracket positions are lacking. Therefore, the current study was conducted to compare the adaptation of a straight wire between brackets positioned at the mid-lingual surface with those placed gingivally by using a three-dimensional (3D) simulation software. The assumption was that the use of similarly designed brackets in both conditions would allow for bracket omission from the study.
MATERIALS AND METHODS
Study samples
This cross-sectional study was performed using OrthoAid, an in-house software designed at Shahid Beheshti University of Medical Sciences, Tehran, Iran. In order to estimate the sample size, a pilot study with 5 samples was performed. A sample size of 35 patients was estimated on the basis of the mean difference in the pilot study, with α = 0.05 and power of 90% (β = 0.9). The inclusion criteria were the presence of all permanent teeth (third molars were ignored), lack of supernumerary teeth, no history of orthodontic treatment, correct upper and lower midlines, proper alignment of teeth with no or less than 1 mm crowding or spacing, no malposition or malformation or rotation of the teeth, no extensive restoration, Class I molar and canine relationship, normal overjet and overbite, no gingival recession, no anterior or posterior crossbite, and no significant intraoral or extraoral asymmetry.
The included subjects were 16 ± 1-year-old adolescents with normal Class I occlusion, whose dental casts were digitized and used in a previous study by the authors.1314 Alginate impressions were taken from each patient and instantly poured with type 4 dental stone. Dental casts were then digitized using a 3D laser scanner (national patent number, 69383; Laser and Plasma Research Institute of Shahid Beheshti University, Tehran, Iran), the diagnostic value of which has been previously demonstrated and confirmed.1516 The resultant mesh files were converted into the conventional *.ply format and imported into the OrthoAid software for further processing. OrthoAid is an in-house non-commercial cast analysis computer software, which has been used in previous studies by the authors.13 Study protocol was approved by ethical committee of Research Institute of Dental Sciences, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran (No. IR.SBMU.RIDS.REC.1394.19).
Placement of reference points
In OrthoAid, the user can select multiple reference points which, in this study, indicate the midpoint of the lingual brackets' base. Therefore, to simplify the method, no brackets were used and only one point for each bracket was applied.
Two bracket positioning approaches were compared in this study. In the first approach (middle group), the reference points were placed on the mid-lingual surface (mesiodistally and occlusogingivally) of each tooth including the second molars. In the second approach (gingival group), only the reference points on the anterior teeth were repositioned to demonstrate gingival bracket placement. In this approach, the lingual surfaces of the anterior teeth were divided into three equal segments occlusogingivally, and reference points were placed in the line between the middle third and gingival third, while maintaining the positions mesiodistally in the middle. In this study, the digital upper and lower casts were loaded separately and measured independently in the software (Figure 1).
Precise determination of reference points was crucial to the experiment. Therefore, all the points were checked twice by an experienced orthodontist. Moreover, the reference points of 10 dental casts were selected twice by a trained examiner, with a 2-month interval, and intraexaminer reliability was assessed using the intraclass correlation coefficient (ICC) and Dahlberg coefficient.
Polynomial curve
Upon selection of reference points by the user, OrthoAid calculates the closest plane that goes through the points (hypothetical polynomial curve plane). This is calculated using principal component analysis and is based on the fact that the third eigen vector of a set of 3D points represents the normal of their regression plane. The reference points are subsequently projected onto this hypothetical plane and a polynomial curve of a given degree is fit onto their projections on the basis of the least-squares fitting formulation (Figure 2). This polynomial curve represents the lingual straight wire in this study. After evaluating the polynomials of different degrees, we concluded that the polynomial equation of the 4th degree results in the least root mean square (RMS) of distances from the reference points while preserving the arch curvature.
Distances of the reference points to the curve
The OrthoAid software measures both the in-plane and off-plane distances of points to the polynomial curve (Figure 1). The in-plane distance represents the geometrical average distance from the polynomial curve to the projected reference points (bracket points) in the horizontal plane, whereas the off-plane distance represents the perpendicular distance of the bracket points to the hypothetical polynomial plane (Figure 2). The mean distances of the right and left teeth were averaged and considered the distance of that tooth to the polynomial curve.
The software also calculates the in-plane and off-plane RMSs of the distances between the reference points and the fitted polynomial curve (Figure 2). RMS ( ) is the quadratic mean of the absolute values, which in this case is the total distance of the 14 teeth to the polynomial curve. A smaller RMS shows that the polynomial curve, which represents the lingual straight wire, is better adapted to the bracket points.
) is the quadratic mean of the absolute values, which in this case is the total distance of the 14 teeth to the polynomial curve. A smaller RMS shows that the polynomial curve, which represents the lingual straight wire, is better adapted to the bracket points.
) is the quadratic mean of the absolute values, which in this case is the total distance of the 14 teeth to the polynomial curve. A smaller RMS shows that the polynomial curve, which represents the lingual straight wire, is better adapted to the bracket points.In our study, the RMSs for each dental cast were recorded twice, once with all the brackets placed in the middle and again with the anterior brackets placed gingivally.
Polynomial curve plane angulation
The angulation of the hypothetical polynomial curve plane representing the straight-wire plane with the occlusal plane of the cast was calculated for each of the two middle and gingival groups. The occlusal plane was defined as the plane that goes through the tip of the mesiopalatal cusps of the first molars and the incisal edge of the right central incisor for the upper jaw, and the plane that goes through the tip of the mesiobuccal cusps of the first molars and the incisal edge of the right central incisor for the lower jaw. The angulation of wire planes in both groups relative to the occlusal plane was measured in degrees.
Statistical analysis
Normal distribution of data was assessed and proven using the Shapiro-Wilk test (p > 0.05). Moreover, Levene's test showed the equality of variances (p > 0.05). Therefore, the mean RMS and mean angulation of wire planes between the two groups were measured and compared using the paired-samples t-test, with a significance level of 0.05 by using IBM SPSS Statistics for Windows/Macintosh, version 21.0 (IBM Co., Armonk, NY, USA).
RESULTS
Thirty-six patients (72 digital upper and lower dental casts) were included in this study. The mean ICC for bracket placement was 0.998, which indicated an excellent intraexaminer correlation. The mean Dahlberg coefficients for the gingival and middle points were 0.256 mm and 0.330 mm, respectively. These were the mean distances of the tooth with the archwire that should be compensated for by bracket thickness and the composite resin used to bond the brackets.
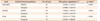
As demonstrated in Table 1, the mean in-plane RMS of the polynomial curve to the bracket distance in the gingival group was significantly lower than that in the middle group (p < 0.001). In contrast, the off-plane RMS was higher in the gingivally positioned brackets in the maxilla than in the middle group (p < 0.001). Comparison of the total off-plane RMS did not show a significant difference between the two groups (p = 0.274). In addition, the angulation of the wire plane relative to the occlusal plane was significantly higher in the gingival group than in the middle group (p < 0.001) (Table 2). As the subjects had normal occlusion, this value could be used to build gingivally positioned brackets that produce the same results as do midlingually positioned brackets. The other option would be to compensate the angulation difference by using a thicker composite resin base for each tooth.
Table 3 shows the mean distance of each tooth to the polynomial curve. In the maxilla, for the middle brackets, the canines had the largest distance to the curve (1.98 mm) followed by the lateral incisors (1.84 mm) and first premolars (1.80 mm), and for the gingival brackets, the lateral incisors had the largest distance (1.68 mm) followed by the canines (1.42 mm) and first premolars (1.30 mm). In the mandible, for the middle brackets, the first molars had the largest distance to the curve (1.76 mm) followed by the canines (1.70 mm) and lateral incisors (1.32 mm), and similarly for the gingival brackets, the first molars had the largest distance (1.76 mm) followed by the canines (1.39 mm) and lateral incisors (1.14 mm). The mean in-plane distances of the canines, first and second premolars, and second molars of both arches as well as the mandibular lateral incisors and the off-plane distances of the mandibular canines and second molars to the curve were significantly smaller in the gingivally positioned brackets than in the mid-lingually positioned brackets (p < 0.05). However, the mean off-plane distances of the maxillary first and second premolars and second molars were larger in the gingival group than in the middle group (p < 0.05).
DISCUSSION
The current study was performed to compare the effects of occlusogingival bracket positioning on the adaptation of a straight wire in lingual orthodontics by using the in-house 3D simulation software OrthoAid. The OrthoAid software, which was also used in previous studies,13 follows mathematical formulations to calculate polynomial curves at the minimum distance to the reference points selected by the user and reports the RMS of the bracket distance to the polynomial, both in and off the polynomial plane. The results showed that the vertical position of the lingual brackets has a significant effect on the bracket distance to the lingual straight wire. Anterior brackets placed more gingivally have less in-plane distance to the straight wire than do brackets placed at the middle of the teeth. Interestingly, measurements of the distance of each tooth to the curve showed that this reduction was significant for the canines, premolars, and second molars of both arches as well as the mandibular lateral incisors. This has two benefits. First, as the wire distance to the lingual brackets decreases, the thickness of the composite resin, probability of bracket debonding, patient discomfort, and interference with the opposing arch teeth decrease.3 Second, as the distance of the bracket to the center of tooth resistance changes, the force vectors and moments applied to the teeth are altered, especially in terms of torque, intrusion, and extrusion.
Torque in orthodontics refers to the buccolingual tipping of the tooth at which crown movement is minimum and root position changes are more extensive. Rectangular arch wires can produce a coupled force in the bracket slot and exert root torque.17 The torque increases as the distance to the center of resistance of the tooth increases.9 Therefore, placement of brackets in more incisal positions could increase the torque and result in crowns with more lingual inclinations. However, one should remember that apart from bracket positions, other factors such as arch wire dimension and material, arch wire torsion relative to the slot of the bracket, and the bracket design also influence the amount of torque.181920 Sifakakis et al.20 showed that Incognito (3M, Maplewood, MN, USA) and STB (Ormco, Orange, CA, USA) lingual brackets produced the highest moment, while self-ligate lingual brackets produced the least amount of moment. In order to understand the best possible position for the bracket slots when using lingual straight wires, we adapted a curve to the lingual surfaces of the teeth to simplify the research question. We did not aim to evaluate the impact of the bracket design and its built-in torque and angulation on the clinical results.
Takemoto and Scuzzo12 explained that lingual orthodontics could use straight-wire appliances if brackets are positioned gingivally. In 2003, Wiechmann et al.11 presented a bracket system for lingual orthodontics and claimed that these brackets have more control on the torque as they have a shorter height and more gingival position than do the conventional lingual orthodontic brackets. They also reported that these brackets produced less lever force on the teeth when occluded with the opposing arch.
Apart from the torque, the vertical position of the brackets could cause undesired tooth intrusion or extrusion.21 The current study revealed that the vertical distance of the brackets to the straight-wire in the maxilla increases with the gingival placement of anterior lingual brackets than with their placement at the middle. This vertical discrepancy was significant for maxillary premolars and second molars. However, considering the conventional method for lingual bracket setup in straight-wire lingual orthodontics,3 the brackets would be placed in the correct vertical position without any discrepancy. In straight-wire lingual orthodontics, following ideal setup, all the brackets (virtual or actual) would be attached to the selected full-size straight wire. Then, the wire holding all the brackets moves toward the teeth until they make contact.312222324 The wire keeping all brackets in one plane, which is similar to the hypothetical polynomial plane of this study, prohibits vertical discrepancy between the brackets. Hence, the results of the current study that showed an increased bracket-to-wire vertical distance in the gingival group would not exert an undesired force on the teeth as no vertical discrepancy occurs in straight-wire lingual orthodontics. In addition, the angulation of the wire relative to the occlusal plane also increases. Although this finding might be interpreted as the application of an extrusive force on the anterior teeth with gingival brackets, it is inevitable. Predicting the effect of the extrusive force on the lingual brackets is difficult. Mathematical analysis showed that extrusive lingual force on the incisors with an inclination of −30° to 20° produces a counterclockwise movement while an inclination of more than 20° produces a clockwise rotation.8 In addition, finite element analysis showed that primary orthodontic movement of uncontrolled tipping causes tooth intrusion.9 The amount of extrusion in the gingival brackets might not be much and could be neutralized with primary intrusion during tooth movements.
In order to evaluate the dental arch form and size, previous studies have used polynomial functions101325 or linear measurements.2627 The current study applied polynomial functions as these follow the curvature of the arch and seem more similar to those used in the straight-wire technique.13
Park et al.10 placed lingual brackets in the mid-lingual surface of the teeth and drew lingual arch curves. They revealed that in the maxilla, the polynomial curves have longer distances to the brackets because of the lingual prominence of the canines. Therefore, they concluded that the application of a straight-wire arch in the maxilla is less predictable. In the current study, the bracket-to-polynomial curve distance was slightly larger in the maxilla than in the mandible. Previous studies used 4th and 6th degree polynomial equations to simulate labial orthodontics.282930 Nouri et al.13 adopted 4th degree polynomial equations on the labial surface of the teeth. However, Park et al.10 used 9th degree polynomial equations for lingual orthodontics and reported that this order results in the least distance to the brackets. In the current study, a 4th degree polynomial was used and it produced an arch form that matched the straight-wire system more closely. Hence, a clinically applicable arch form was simulated.
CONCLUSION
Within the limitations of this study, it could be concluded that the gingival placement of lingual brackets on the anterior teeth could decrease the distance between the brackets and the straight wire, especially in the canines, premolars, and second molars of both arches as well as the mandibular lateral incisors. This could cause better adaptation of the straight-wire brackets to the teeth and decrease bracket debonding. However, the vertical distance of the brackets to the anterior teeth and the angulation of the wire plane relative to the occlusal plane increases in the gingivally positioned brackets. Further biomechanical studies should be performed to evaluate the clinical significance of these differences and their effects on the teeth.




 XML Download
XML Download