

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Transverse colon volvulus (TCV) is a rare disease representing 3% of all colonic volvulus [1]. Situs inversus (SI) is also a rare genetic condition in which all visceral organs in the thorax and abdomen are laterally mirrored from their normal position [2]. Gastrostomy can cause various major and minor complications, but intestinal volvulus around the gastrostomy tube has not been reported in more than one case in English literature [34]. Here, we report a case of TCV around the gastrostomy tube in a pediatric patient with SI.
CASE REPORT
An 18-year-old boy with cerebral palsy and scoliokyphosis visited the emergency department with abdominal distension and vomiting for one day. On physical examination, the abdominal distension and hypoactive bowel sound were checked; however, pain or tenderness could not be confirmed due to his underlying cerebral palsy. He had similar symptoms of abdominal distention and vomiting thrice in the last six months. The first two endoscopic decompressions were done at other hospitals and the last time was performed at out institution because sigmoid volvulus was suspected. Fluid resuscitation was initially attempted.
The patient experienced recurrent aspiration pneumonia and seizure one year ago. There was no problem in ingestion until aspiration pneumonia occurred, but, because of increased aspiration tendency during oral feeding, he was under nasogastric tube feeding for 1-year. For long-term management, percutaneous endoscopic gastrostomy (PEG) was planned, and an upper gastrointestinal (UGI) study was done in our institution. On UGI, the right-sided stomach was seen, and associated intestinal malrotation, without volvulus, was found (Fig. 1). Situs anomaly was suspected for the first time since birth during this study, and PEG was performed without complications when he was 17 years old.
The patient's last event was five months before the current problem, and abdominal computed tomography was done at an outside hospital for further evaluation. Beak-like appearance of mid transverse colon and upstream bowel dilatation, involving the proximal transverse colon, ascending colon, and cecum was seen with situs inversus. Then, he moved to our hospital, and on the next morning, endoscopic decompression was performed. His symptoms improved and discharged home.
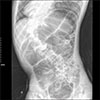
At the time of the current visit, the laboratory values were normal, except for the presence of leukocytosis (13,720/µL) and a C-reactive protein elevation to 1.85 mg/dL. Initial vital signs were stable at the time of the visit to the emergency department. On X-ray imaging, diffuse gaseous distension of colon was seen (Fig. 2), and right-sided stomach gas was also seen, which was identified as SI at the previous visit to Seoul National University Hospital which was mentioned above.
Decompression with rectal tube at emergency department after suspecting sigmoid volvulus was attempted, but passing of gas was barely seen and the follow-up X-ray did not show any improvement. Emergency endoscopic decompression was tried on the same day and suspicious volvulus sites were observed at the anal verge, 20 cm and 50 cm, but it was not clear whether they were correct sites. He was admitted to the ward for close observation, and abdominal distention and vomiting were seen to improve immediately after the procedure. However, abdominal distention became aggravated three days after endoscopic decompression, and he vomited for more than 10 times a day. Our team decided to perform laparoscopic exploration.
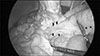
During laparoscopic exploration, adhesion of the transverse colon to the stomach wall of the gastrostomy site was seen and appeared twisted (Fig. 3). Proximal transverse colon was redundant and upstream dilatation from the twisted transverse colon to the ascending colon and the cecum was found with reversed intestinal anatomy, as identified on preoperative images. Sigmoid colon was collapsed and not redundant, so the suspicious sites of endoscopy were not related to the symptoms. Adhesiolysis and fibrous band lysis between the transverse colon and adherent soft tissue was done. Redundant proximal transverse colon was resected via mini-laparotomy site, and end-to-end colocolic anastomosis was performed (Fig. 4). There was no postoperative event, and the patient was discharged without complications.
DISCUSSION
TCV in the pediatric population is a rare condition, representing only about 3% of all reported cases of colonic volvulus [1]. Chronic constipation, mental retardation, and myotonic dystrophy are risk factors for TCV [5]. Abnormal posture in children with cerebral palsy may also be a contributory factor for distention of the colon [6]. Our patient had a related risk factor of scoliokyphosis with cerebral palsy.
SI is also a rare anomaly in which internal viscera are located on the opposite site of the body to the expected location [2]. SI is more associated with bowel twisting due to the abnormal mobility of bowel segments caused by the improper developmental fusion of the mesentery to the posterior abdominal wall, increasing the rate of volvulus in SI rather than in the normal population [278].
Gastrostomy, performed in the percutaneous endoscopic or surgical way, is usually considered a safe procedure, but various minor and major complications can occur. Minor complications like granuloma formation, local wound infection, peristomal leakage, tube dislodgment and gastric outlet obstruction, as well as major complications including bleeding, aspiration pneumonia, necrotizing fasciitis, buried bumper syndrome and internal organ injury have been reported [3].
However, TCV around the gastrostomy tube was reported in only one case in English literature in a 15-year-old boy [4]. Like our patient, he had abdominal distention and vomiting with underlying cerebral palsy. After suspecting sigmoid volvulus, endoscopic decompression was attempted, but failed. Since his vital signs were unstable, he was taken to operating room for exploratory laparotomy. During surgery, a gangrenous, distended transverse colon was found, which had twisted in on itself (closed loop obstruction) and around the gastrostomy tube site to the point where the stomach was adherent to the abdominal wall. Right hemicolectomy with an end-to-end ileocolic anastomosis was performed, and his post-surgical course was uneventful. Unlike sigmoid volvulus, which can be decompressed by colonoscopy, TCV must be managed surgically to prevent recurrence [910].
In our case, TCV was not properly managed by endoscopic decompression. His bowel color change was not observed and there were no evidences of colon ischemia at the time of the exploration. Timely surgical management with detorsion and redundant bowel resection was performed without post-surgical complications.
We report the first case of transverse colonic volvulus around the gastrostomy tube in SI patient. When patients with gastrostomy tube present similar symptoms of abdominal distension and frequent vomiting, suspicion of transverse colonic volvulus is the first step in diagnosis. Fluid resuscitation and timely diagnosis with radiologic imaging is important. Surgical resection of the redundant colon must be done for proper management before proceeding to bowel ischemia.


 XML Download
XML Download