

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prevalence of diabetes is increasing worldwide. The number of people with diabetes reached 422 million in 2014, and diabetes caused 1.5 million deaths in 2012 [1]. Despite tremendous advances in treatment over the last few decades, reducing mortality and morbidity in diabetic patients through adequate blood glucose control remains challenging.
Diabetes is a chronic disease that requires numerous daily self-care-related decisions and behaviors pertaining to food choices, physical activity, and medication use. Diabetes education improves knowledge and skills related to the control of diabetes, which is essential for people with the disease [2]. Diabetes education has been considered an important facet of the clinical management of individuals with diabetes since the 1930s [3]. The American Diabetes Association recommends assessments of diabetes self-management skills and knowledge, and the provision of diabetes education at the time of diagnosis on an, annual basis, and whenever a complication arises or transition in care occurs [2]. Diabetes education has been reported to improve blood glycemic control and reduce diabetic complications [4567]. In addition, diabetes education reduces the hospitalization and re-admission rate of diabetic patients, thereby reducing the economic burden of treatment [89].
In most diabetes educational interventions, diverse educators, such as clinicians, nurses, pharmacists, nutritionists, exercise therapists, and social workers address diabetic patients individually, according to their own specific areas of expertise. Because the conditions of diabetic patients are so diverse, a uniform educational approach based on a single discipline has limitations. Each educator may emphasize the importance of his or her field without knowing what problems the patient has that are relevant to other fields, and patients could be confused due to a lack of understanding of the multilevel problems that they may encounter. In addition, there are invisible barriers in communication among diabetes educators. Therefore, diabetes education is expected to be more effective when integrated education is provided, rather than an individualistic approach.
In this study, we evaluated the effect of a multidisciplinary diabetes educational intervention, provided by a team of clinicians, nurse specialists, pharmacists, and nutritionists, on glycated hemoglobin (HbA1c) levels among diabetes patients.
MATERIALS AND METHODS
1. Patients, materials, and methods
In this matched case-control study, 141 patients hospitalized with type 2 diabetes were recruited at the Department of Endocrinology and Metabolism, Pusan National University Hospital. The protocols and consen t procedures were approved by the Institutional Review Board of Pusan National University Hospital (approval no. 20140223).
We enrolled 40 patients in the education group who were hospitalized between June 2014 and September 2016, diagnosed with type 2 diabetes, aged above 18 years, able to communicate normally, and who agreed to take part in multidisciplinary team care sessions. Patients with cancer or severe illnesses, and those with communication problems, were excluded from the study. The control group consisted of 101 patients who were admitted during the same period and met the same exclusionary criteria as the education group, but did not receive education from the multidisciplinary team. Both education and control groups were admitted for blood glucose control. All of the education group patients had never received a team-based education before agreeing to this study. There was a significant difference in HbA1c level between the education and control groups; therefore, 27 pairs of hospitalized patients were matched using propensity scores. Propensity score matching analysis was performed with support from Department of Biostatistics of Pusan National University Hospital.
The multidisciplinary team consisted of clinicians, nurse specialists, pharmacists, and nutritionists. When a hospitalized patient meeting the inclusion and exclusion criteria, the clinician requested the multidisciplinary team care sessions after obtaining the patient's consent. The multidisciplinary team care sessions were performed once a week, and more than once during the hospital stay. Before the multidisciplinary team care sessions, the clinician, nurse specialist, pharmacist, and nutritionist individually assessed and interviewed the patient. The nurse specialist educated patients on how to properly administer insulin, and patient performance with respect to insulin injections was measured by the Performance Accuracy Questionnaire for Insulin Injection (Supplementary Table 1). The pharmacist educated patients about oral hypoglycemic agents, and medication compliance was measured by the Modified Morisky Scale (Supplementary Table 2). The nutritionist educated patients about the diabetic diet. The nutrition assessment, diagnosis, and intervention were evaluated according to nutritional counseling results (Supplementary Table 3). On the day of the multidisciplinary team care session, all team members convened just before the session to present and discuss the patient's condition. The clinician led the multidisciplinary team care sessions, which were held during the patient's lunch time. After each round of multidisciplinary team care, the team members discussed the patient and wrote a report.
All patient charts were reviewed by the same clinician. HbA1c levels were measured at the time of enrollment, and at 3 and 6 months post-enrollment. HbA1c levels measured at 3 and 6 months included data collected 1 month before and after.
2. Statistical analyses
Statistical analyses were performed using SAS software (ver. 9.3.0; SAS Institute, Cary, NC, USA) and R software (ver. 3.3.2; R Development Core Team, Vienna, Austria). Data are presented as mean ± standard deviation or as median (interquartile range) for skewed variables. Differences between the two groups were analyzed by parametric two-sample t-tests and non-parametric Wilcoxon rank-sum tests. The chi-squared test was applied to analyze categorical variables. The nearest neighbor matching method was used to classify the education group based on the similarity to the control group propensity score. A twotailed P < 0.05 was considered statistically significant.
RESULTS
1. Baseline patient characteristics
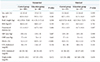
Table 1 summarizes the baseline characteristics of the patients with type 2 diabetes. Sex, age, body mass index, duration of diabetes, systolic blood pressure, diastolic blood pressure, and lipid profiles did not significantly differ between the education group and the control group. HbA1c levels were higher in the education group than in the control group in an unmatched case-control study. Table 2 shows differences in the status of baseline medication between the two groups. There were no patients treated with oral antidiabetic drugs in the education group, and a basal-bolus insulin regimen was more common in the education group than in the control group.
2. Changes in HbA1c level: comparison between the education group and the control group
In the education group, the HbA1c level was significantly reduced, from 10.2 ± 2.0% to 6.3 ± 2.3%, after 3 months of multidisciplinary team-based diabetes education (Fig. 1A). In the control group, the HbA1c level was reduced from 10.0 ± 3.1% to 9.5 ± 4.0% after 3 months. After 3 months, the reduction rate was −35.7 ± 26.1% in the education group and −9.1 ± 20.5% in the control group (Fig. 1B), and there was a significant difference between the two groups (P = 0.013; Table 3).
The HbA1c level in the education group after 6 months was 7.5 ± 1.5%, which was slightly higher th an that after 3 months. The HbA1c level after 6 months in the control group was 9.6 ± 3.0%. The HbA1c level of the education group tended to be lower than that of the control group after 6 months, but the difference in HbA1c level between the two groups after 6 months was not significant (P= 0.106).
DISCUSSION
In this study, patients who received team-based diabetes education had lower HbA1c levels at the 3-month follow-up than the non-educated control group patients. This suggests that a multidisciplinary educational intervention provided by clinicians, nurse specialists, pharmacists, and nutritionists can increase the effectiveness of treatment for diabetic patients.
Previous studies have shown that various forms of diabetes education are associated with lower HbA1c levels in diabetes patients. Steinsbekk et al. [10] reported that group-based diabetic self-management education in adult type 2 diabetes patients reduced the HbA1c level by 0.87% and improved diabetic knowledge and self-management skills. Norris et al. [5] reported that self-management education lowered the HbA1c level by 0.76%. According to a study by Kim et al. [6] done in Korea, the HbA1c level decreased from 7.84% to 6.79% following self-management education. Several previous studies have also reported a reduction in HbA1c of about 1% after diabetes education [11121314]. In this study, 3 months after team-based diabetes education, the HbA1c level decreased from 10.2 ± 2.0% to 6.3 ± 2.3%, a considerable change compared to previous studies. However, this may be due to the effects of increased diabetic medication use.
According to the UK Prospective Diabetes Study (UKPDS), a 1% reduction in the HbA1c level over 10 years reduces the risk of diabetes-related death by 21%, reduces myocardial infarction risk by 14%, and reduces the microvascular complication rate by 36% [15]. Therefore, the decrease in HbA1c level from 10.2 ± 2.0% to 6.3 ± 2.3% after 3 months in this study was very meaningful. However, there was no significant difference in HbA1c between the education group and the control group after 6 months. Norris et al. [5] reported that the initial effects of diabetes education decreased after 6 months. Brown reported that the effects peaked 1 to 6 months after intervention, and decreased to back to the initial level after 6 months [16]. The effects of education decreased with longer follow-up intervals after the intervention in the study by Norris et al. [5]. This trend is common not only among studies of diabetes education, but also in studies of other behavioral interventions for weight loss [171819]. Although diabetes education is effective, the data suggest that the benefit does not persist. For diabetes education to effectively reduce long-term complications, the initial effects of glycemic control must be maintained over the long-term. Therefore, regular and continuous long-term intervention is required.
The limitations of this study were as follows. First, drug treatments were not taken into consideration, although medication changes can affect treatment effectiveness. Second, the patient enrollment rate was low, and follow-up loss was high. Third, we did not investigate changes such as complications other than HbA1c. Fourth, there was no assessment of changes in the method of drug administration, the method of insulin injection, compliance with medication, dietary control, etc. Despite these limitations, this study is meaningful as the first study to paradoxically emphasize the importance of team-based education in the management of type 2 diabetes when considering the clinical situation in Korea where it is not easy for diabetes education to satisfy both patients and medical staff within a limited time.
In this study, the positive effect on glycemic control seen after the team-based diabetes education intervention was presumably due to appropriate administration methods, and improvements in compliance with medications, dietary habits, and insulin use. Multidisciplinary education delivered by clinicians, nurse specialists, pharmacists, and nutritionists can lead to proper glycemic control and, ultimately, a reduction in diabetes complications and mortality. Continuous follow-up and education on the various factors influencing glycemic control are required for sustained effectiveness. However, it is difficult to provide a team-based diabetes education intervention t o all diabetes patients. In practice, patients often receive medication in small primary clinics as well as in large hospitals, and it is rare to encounter diabetes experts other than doctors at these primary clinics. Previous studies reported variously that only 26.2% and 39.4% of diabetes patients received diabetes education [2021]. The effectiveness of diabetes education has already been shown in multiple studies; thus, it is necessary to find ways to overcome the limitations associated with practical application of diabetes education.
In conclusion, this study showed that team-based diabetes education, involving clinicians, nurse specialists, pharmacists, and nutritionists, improved glycemic control in diabetes patients. Further research is needed to determine whether the long-term effects of team-based diabetes education lead to long-term maintenance of target HbA1c levels and thus reduce the rate of diabetic complications.



 XML Download
XML Download