

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Most adult patients undergoing orthodontic treatment complain of experiencing various levels of orthodontic post-adjustment pain [1]. In a 1985 survey, focused on the attitudes of patients and parents toward orthodontic treatment, Oliver et al. reported that pain induced by the appliance is the major discouraging factor [2]. Another study reported that 30% of patients wanted to terminate the treatment solely because of the pain they experienced [3]. Furthermore, one of the main aspects of oral health-related quality of life is pain control [4]. Additionally, pain has a negative impact on oral hygiene [5]. It is not possible to predict the incidence and severity of pain experienced by the patient [6]. Ultimately the amount of satisfaction of the patient with the outcome of treatment is affected by the overall amount of pain experienced [7].
The mechanism underlying the pain involved in orthodontic treatments is not fully understood. However, several explanations have been proposed. One explanation suggests that applying orthodontic forces to the teeth causes a release of inflammatory and proinflammatory mediators [8]. One of the key inflammatory mediators are prostaglandins, which act as a mediator for tooth movement but also increase pain and the transmission of pain stimuli [9]. Moreover, development of ischemic areas in the periodontal ligament undergoing sterile necrosis is thought to be related to the pain caused by the orthodontic treatment. There is a direct correlation between the force applied and the amount of pain the patient experiences, as larger forces create larger ischemic areas and therefore more pain [10].
There are two objectives when controlling inflammation: pain relief and halting tissue destruction. Transcutaneous electrical nerve stimulation, vibratory stimulation, low-level laser therapy [111213], using chewing gum or bite wafers [6], application of local/topical anesthesia [14], and oral administration of non-steroidal anti-inflammatory drugs (NSAIDs) [6] are among the methods that have been advocated for reduction of orthodontic pain. However, each of these methods has its disadvantages. For example, there is a possibility of tongue biting and lip burns secondary to the administration of local anesthetic agents, particularly in children; using NSAIDs in high doses may hinder tooth movement; and aside from difficulty experienced in chewing bite wafers or gum, such chewing may bend the orthodontic wires [15].
Naproxen and naproxen sodium are effective non-steroidal, anti-inflammatory analgesics marketed under the brand names Anaporax and Diocodal. It is absorbed in the gastrointestinal tract and metabolized by the liver, and has a plasma half-life of 12–15 hours and it is mainly excreted through urine. It may cause gastrointestinal bleeding, exacerbation of asthma attacks in asthmatic patients, and should be administered cautiously in patients having renal or hepatic disorders [16].
The objective of this study was to evaluate the efficacy of a naproxen patch in decreasing pain after the placement of elastic separators in patients undergoing fixed orthodontic treatment.
Go to : 
METHODS
The study was approved by the Ethics Committee of Dental School of Shahid Beheshti University of Medical Sciences' and registered in the Iranian Registry for Clinical Trials (http://www.irct.ir, identifier: IRCT2014-0203016466N5).
Assuming a type-one error of 0.05 (α = 0.05), a type-two error of 0.2 (β = 0.2), and an effect size of 3.2 (e.s. = 3.2), the total sample size required was calculated to be 29.
Patients aged 14–19 years, who were candidates for fixed orthodontic treatment and needed separator placement for the banding of their first molars, were included in this study. The patients were selected from among those who had been referred to a number of private orthodontic clinics and clinics associated with the Shahid Beheshti University of Medical Sciences during 2014 and 2015. The inclusion criteria were a lack of any systemic diseases, absence of periodontal or endodontic problems, age ranging between 14 and 19 years, tight contact of the first molar with the adjoining teeth, requirement of bilateral placement of elastic separators, absence of spacing, no use of systemic drugs for pain reduction, having antagonist teeth in the opposing arch, and absence of a posterior open bite. The exclusion criteria were detachment of one of the separators, failure to apply the placebo or naproxen patch, not completing the questionnaire, and using systemic analgesic drugs.
The patches were produced in the Shahid Beheshti University of Medical Sciences' School of Pharmacy. The size of the initial patches was selected based on a former study by Eslamian et al., in which they used benzocaine mucoadhesive patches to reduce pain after separator placement [17]. Initially, a pilot study was performed in order to assess the taste, durability, adhesion properties, and the appropriate way for using this patch. A total of six patients were enrolled in this pilot study and were not included in the main study. These patients were asked to place the patch on the gingival tissue of one of the permanent first molars and hold it there until the patch attached to the gingiva. Subsequently, the patients were instructed to change the patch for a new patch every 8 hours. Moreover, they were asked to mark their pain on a visual analog scale (VAS) scoring form, with numbers ranging from 0 to 100 in 10-point intervals. Based on the information obtained from the pilot study, it was concluded that the naproxen patch should consist of the following: 1) hydroxypropyl methylcellulose (2.5%) and polyvinylpyrrolidone (1%) for tissue adhesion; 2) propylene glycol; 3) dichloromethane and ethanol (2:1 ratio), acting as solvents; 4) aspartame (0.25%) as sweetener; and 5) naproxen (5 mg) (South China Pharmaceutical Company, Shenzhen, China). The placebo patch contained all of these components, except naproxen. Moreover, the patch did not have any systemic effect and acted only locally; the lowest effective concentration of naproxen was determined as being 5%. The final size of the patch was determined as 1.5 × 0.5 cm.
A split-mouth design was chosen for the main study in order to minimize individual differences affecting pain experience; this study design allowed comparison of case and control groups in the same patient.
After obtaining written informed consent from all the patients, the separators (American Orthodontics, Monrovia, CA, USA) were placed on the mesial and distal sides of permanent first molars of the right and left sides of one of the jaws, using a pair of orthodontic separator pliers (Dentaurum, Springen, Germany). Each patient was given a total of 18 patches (nine naproxen patches and nine placebo patches). The patches were divided into two groups (group A and B) for each patient. Each group was randomly assigned to the right- or left-side permanent first molars. Neither the assistant nor the patient knew the contents of the group A and B patches, as we used a double-blind study design. Each group was coded in order to facilitate further investigation. The patients were instructed on how to place the patch along the margin of the buccal free-gingiva correctly, and hold it there until the patch attached to the gingiva. They were asked to change the patch every 8 hours for 3 days (the last one was used on the 4th day at 10 am) and mark the level of pain they experienced on a 0- to 100-point VAS scoring form after 2, 6, and 24 hours and on the 2nd, 3rd, and 7th day after placement of the patches. The age and sex of each patient were also recorded.
A statistical analyst extracted the data from the questionnaires. Using the Kolmogorov-Smirnov test, the distribution of the data was evaluated and was found to be normal. Due to the existence of independent factors of time and the side of jaw to which the drug was applied, and non-independent factors of gender and age groups and the normal distribution of the data, a variance analysis parametric test was used. P < 0.05 were considered statistically significant. Pairwise comparisons of time points were made using the Bonferroni method. The differences in the severity of pain between males and females, and between patients younger than 16 old and ≥16 years, were analyzed using multifactorial repeated-measures analysis of variance (ANOVA).
Go to :
RESULTS
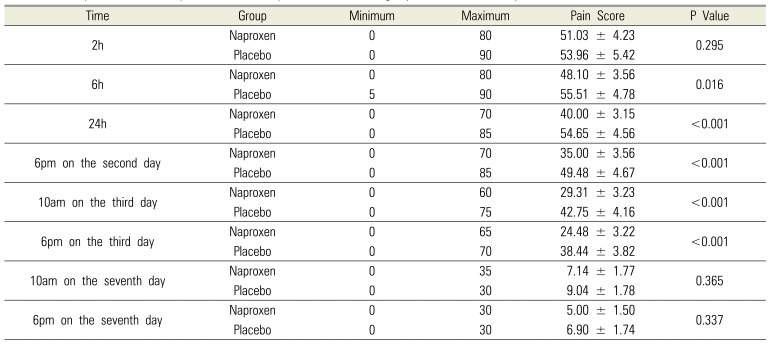
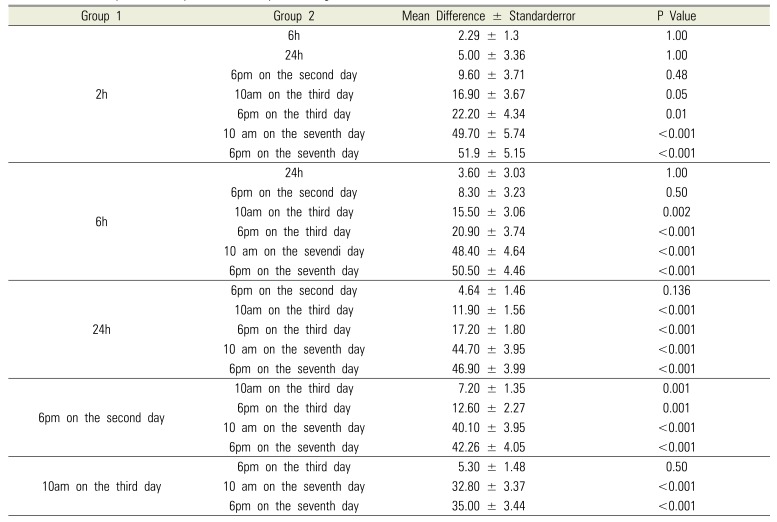
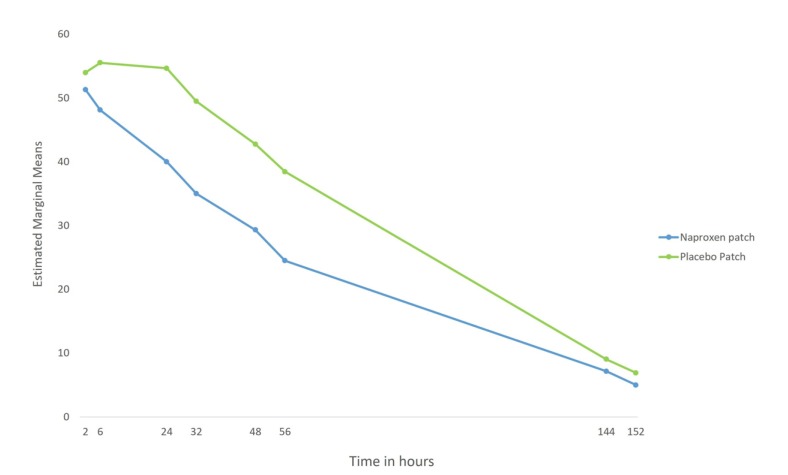
A total of 35 patients participated in this study. Six were excluded as they did not mention experiencing any pain, had not filled out the questionnaires correctly, or used systemic drugs. Of the remaining 29 patients, 21 (72.4%) were female and eight (27.6%) were male. The mean age of the participants was 16.05 ± 1.33 years (ranging from 14 to 19 years). Nineteen patients were 16 years of age or older (≥ 16 years) and 10 patients were under 16 years of age (< 16 years). Variance analysis using a parametric test indicated that the level of pain experienced by the patients decreased over time with use of the naproxen patch (Table 1). The mean VAS scores and the reduction in this score for each method over time is shown in Figs. 1 and 2. Additionally, the Bonferroni method showed that there were significant differences between time points (Table 2). Multifactorial repeated-measures ANOVA was used to analyze the severity of pain between males and females and between age groups, and revealed that the level of pain was not significantly different between males and females (P = 0.059; Fig. 3) or between those aged <16 years or ≥16 years (P = 0.106; Fig. 4).
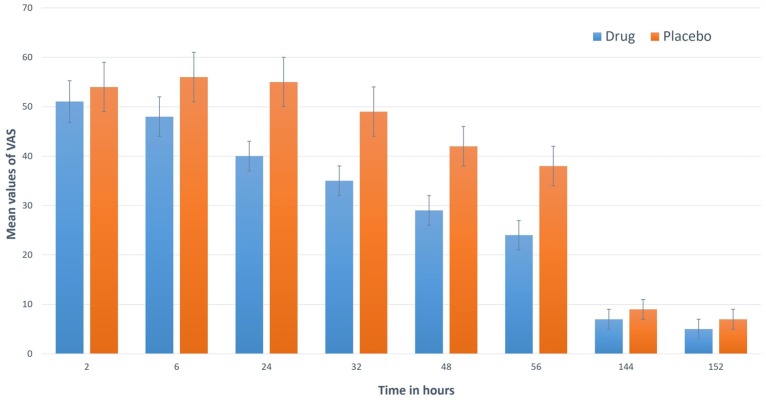 | Fig. 2Mean and standard deviation values of visual analogue scale scores for naproxen and placebo patches.
|
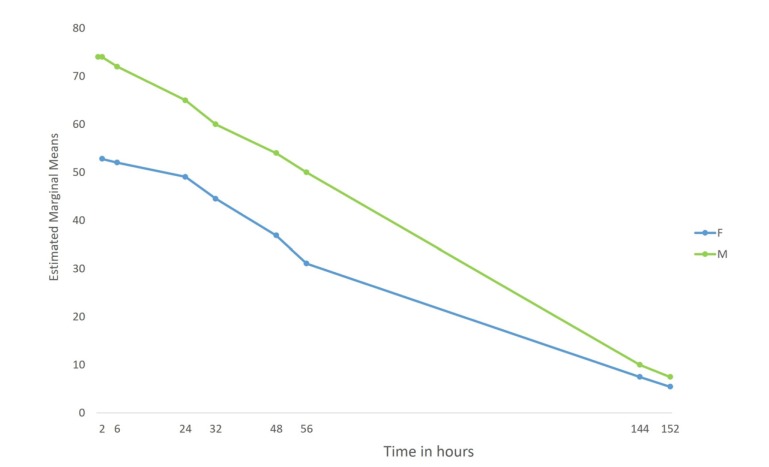
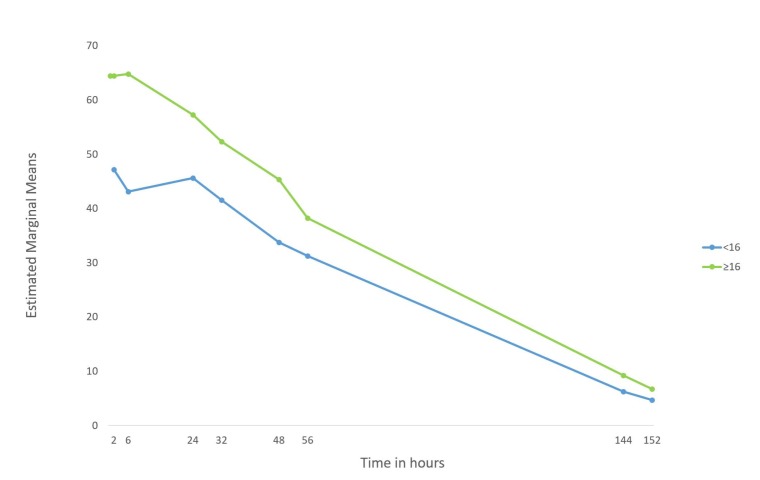
Table 1
Descriptive statistics of pain scores in 29 patients in the two groups at different time points
![]()
Table 2
Results of pairwise comparison of time points using the Bonferroni method
![]()
Go to :
DISCUSSION
This study evaluated the efficacy of a 5% naproxen patch in reducing pain after orthodontic separator placement. The obtained results showed that the naproxen significantly reduced the pain significantly more than the placebo patch (P = 0.004). Neither sex nor age influenced the pain experience. Furthermore, pairwise comparison of the time points showed that there were significant differences between time points; however, these findings were inconsistent. Since perception of pain is subjective, it is difficult to evaluate and compare the level of pain between case and control groups in the presence of confounding factors. Therefore, in order to minimize these confounding factors and the individual differences caused by the diversities in pain perception, this study was structured to have a within-subject, split-mouth design. Previous studies, such as those by Kluemper et al. in 2007 that evaluated the efficacy of a wax containing benzocaine on the relief of pain caused by orthodontic appliances, and by Ngan et al. in 1994 that investigated the anti-inflammatory effect of ibuprofen and aspirin on orthodontic pain reduction, were conducted in parallel groups [914]. This design has several drawbacks. For instance, simultaneous comparison of placebo and drug is not possible in this design. Moreover personal differences may influence the outcome of the study. The split-mouth design was recently used in a study by Eslamian et al., which evaluated the efficacy of 20% benzocaine patches on reduction of post-separation orthodontic pain [17].
A split-mouth design allows simultaneous comparison of the case and control in opposite sides of a jaw, which eliminates confounding factors caused by variations in anatomic forces between jaws in different individuals. Since referral pain does not cross the midline, comparison of pain on opposite sides of a jaw eradicates the effect of referral pain [14].
From a clinical perspective, separator placement is often linked with a great deal of pain; however, this varies greatly between patients and some patients report no pain at all. The main advantage of using separators for orthodontic pain induction is that it facilitates sample matching and eliminates confounding factors, such as unequal forces to the jaws, and therefore increases the similarity between case and control groups. Previous studies, such as those of Eslamian et al. in 2013, Lim et al. in 1995, and Harazaki et al. in 1998, used placement of a separator for pain induction [17181920].
Because the aim of this study was to assess the analgesic efficacy of a certain drug, the patients were selected accordingly. Therefore, the inclusion criteria stipulated application of a certain amount of load to the first molars. In order to achieve this goal, these conditions had to be met: tight contact of first molars with the adjacent teeth, presence of opposing teeth on both sides, occlusal contact of first molars with opposing teeth, and absence of posterior open bite. The minimum age of patients was set at 14 years, because of the greater possibility of such tight contact and better cooperation of the patient.
Since pain perception is a subjective matter, a within-subject design should be applied in order to minimize the effect of confounding factors on pain experience. A few recent studies applied a split-mouth design to evaluate the efficacy of analgesic drugs on orthodontic pain control [1721]. Based on this evidence, it was decided that a split-mouth design should be applied in this study, too. Furthermore, in order for the patients to assess their pain experience and record it over time, a VAS form was given to each patient to record their level of pain. Several previous studies used a VAS form and questionnaires to assess the level of pain experienced by the patients [22232425262728].
Since orthodontic patients usually experience pain locally, local methods of pain control are effective in reducing such pain [10]. Reduction of inflammation by anti-inflammatory drugs results in pain relief for a considerable period of time; moreover, most non-narcotic analgesic drugs have anti-inflammatory effects. These drugs are effective inhibitors of cyclooxygenase-mediated pathways, which involves the main enzymes in the catabolic pathways of arachidonic acid [29]. Naproxen sodium (under the commercial names of Dicodal and Anaprox) is an NSAID inhibiting the formation of leukotrienes and prostaglandins; therefore, it is strongly anti-inflammatory. Possible side effects are gastrointestinal bleeding and escalation of asthmatic attacks in asthmatic patients. It should also be used with caution in patients suffering from kidney or liver diseases [16]. Furthermore, it has been shown that tooth movement could be impaired if high concentrations of NSAIDS are used [30]; however, the patches were used only during the separator placement stage of treatment (3 days) and not for the whole duration of fixed orthodontic treatment, and thus it could not have interfered with tooth movement. It is also important to point out that the amount of naproxen in the patch was 5 mg, which was rather low (overall = 9 × 5 = 45 mg for all patches), and thus it could not have had any significant systemic effects. Based on the results of our pilot study, 5% naproxen was chosen as the lowest effective concentration for the drug patch. Additionally, 8-hour intervals were chosen for replacement and use of the patches, based on a previous study [14] and consultation with pharmacists, in order to minimize the side effects and increase patient cooperation.
The results obtained from this study revealed a significant difference between the two patches after 2, 6, and 24 hours and at the 2nd and 3x day, but not the 7th day after placement of the patches. The highest difference was observed after 24 hours and on day 2 at 6 pm (after 30 hours). After the 2nd day, the pain was reduced, with both of the patches. Furthermore, data analysis showed that the maximum level of pain experienced by the patients was at 6 hours and 24 hours after separator placement. This was in agreement with the study of Ngan et al. in which the pain was recorded at 4 h, 24 h, and day 7 after placement [9]. They concluded that the maximum level of pain occurred at 24 hours after separator placement. In another study, Eslamian et al. recorded the level of pain at 4 h, 6 h, 24 h, 30 h, and on the 3rd and 7th day, and reported that the highest level of pain occurred at 30 hours after separator placement [19].
There was no significant difference in the level of pain experienced between males and females in this study (P = 0.059), which was in agreement with previous studies on this matter [141931]. No significant difference was found between the two age groups (< 16, ≥ 16 years; P = 0.106). This may be due to the close proximity of the age range between these groups. The division of the age range was based on a recent study by Eslamian et al., in which the analgesic efficacy of 5% naproxen gel for pain associated with orthodontic separator placement was assessed [32]. They concluded that there was no difference between the age groups and that naproxen gel was effective for reducing pain caused by separator placement. Another study by Eslamian et al. in 2013 also showed that there was no significant difference between <18 and >18 year age groups [9]. A further study by Eslamian et al. concluded that there was a negative correlation between the level of pain and age [17]. On the other hand, Brown et al. reported that patients in the age range of 14–17 years experienced a greater level of pain than those under 13 years and those over 18 years of age [33]. Scheurer et al. reported a similar result. They concluded that the highest level of pain occurred in the age range of 13–16 years [31].
Based on the significant difference in the level of pain between the case and control groups at all time intervals except the 7th day, it can be concluded that the 5% naproxen patch is efficient for pain reduction in the first few days after separator placement. Moreover, the highest level of pain was recorded at 6 and 24 hours after separator placement and was reduced to its lowest level by the 7th day.
Go to :
 XML Download
XML Download