

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acquired demyelinating syndromes in adults include multiphasic diseases such as multiple sclerosis (MS), neuromyelitis optica (NMO), and neuromyelitis optica spectrum disorders (NMOSD), and monophasic diseases such as acute disseminated encephalomyelitis (ADEM). The data reported by a few groups suggest that activated cytokines and nitrosative stress are closely involved in the pathophysiology of different demyelinating disorders via the induction of the neuroinflammatory destruction of neurons.1 However, the activation profile of cytokines varies with the demyelination pattern.
Interleukin-6 (IL-6) is recognized as an important cytokine involved in inflammatory diseases of the central nervous system (CNS). IL-6 is crucial for the activation of immune cells and can act as a neurotrophic factor. IL-6 exerts its cellular effects via two distinct pathways: the first pathway involves the membrane-bound interleukin-6 receptor (IL-6R) that is expressed on microglia and other cells and acts via the β-receptor glycoprotein 130, while the alternative pathway is trans-signaling via a soluble form of the IL-6R capable of binding IL-6. IL-6 can be produced by a wide variety of cells, including macrophages, mast cells, dendritic cells, activated T- and B-cells as well as several types of nonhematopoietic cells, including astrocytes and fibroblasts. In demyelinating lesions, IL-6 is secreted by infiltrating leukocytes, local microglia, and activated astrocytes.2
Matsushita et al.3 reported that IL-6 levels in cerebrospinal fluid (CSF) were higher in MS patients than in controls. However, IL-6 levels were found to be higher in NMOSD patients than in both MS patients and controls4; notably, a higher IL-6 level in the peripheral blood in NMO was associated with the production of anti-aquaporin-4 (AQP4) antibodies,5 which could result from the increased survival of plasmablasts producing AQP4 antibodies.6 Wullschleger et al.7 found that a CSF IL-6 cut-off of 10 pg/mL provided a sensitivity of 96% for excluding MS, and in such cases other inflammatory disorders should be suggested.
Uzava et al.8 reported that a CSF IL-6 cut-off of 7.8 pg/mL produced a sensitivity of 73.17% and a specificity of 76.94%, which can provide a strong additional diagnostic marker for NMOSD among other patients with neurological disorders. The CSF IL-6 levels in these patients were correlated with the length of the spinal-cord lesion and anti-AQP4-antibody positivity, and they decreased after treatment.
IL-6R blockade with the monoclonal antibody tocilizumab has successfully used in NMOSD,9 though other case reports demonstrated MS arising during tocilizumab therapy in rheumatoid arthritis patients10 and MS-like demyelinating disorders were described due to tocilizumab treatment.11 These different responses to IL-6R blockade may be due to different patterns of B-cell activation and prominent IL-6 involvement in NMOSD, which has not been identified in MS so far.12 Thus, how IL-6R blockade influences the progression of demyelination in different demyelinating disorders remains obscure.
Current challenges in the management of patients with demyelinating disorders are related to the lack of biomarkers useful for stratifying their different clinical forms. Previously Kaplin et al.13 suggested that different nitric oxide (NO) expression levels in the brain and spinal cord are associated with specific IL-6 pathways. We previously demonstrated an association between the serum S-nitrosothiols (RSNO) level and spinal-cord injury.14 It therefore seemed reasonable to explore potential associations between RSNO and IL-6 levels in MS and other demyelinating disorders (NMOSD and ADEM) while controlling for neurodegeneration processes using CSF levels of phosphorylated neurofilament heavy chain (pNfh).
This study analyzed relationships between RSNO, and IL-6 CSF level as well as pNfh levels with the aim of accurately evaluating the severity of axonal damage at the moment of sampling and erythropoietin (EPO) levels as a marker of anti-inflammatory defense in patients with demyelinating disorders.
Go to : 
METHODS
Three groups of patients were examined: relapsing-remitting multiple sclerosis (RRMS, n=52), ADEM (n=9), NMOSD with aquaporin-4 immunoglobulin G (AQP4-IgG, typical NMO, n=12), and a control group (n=24).
Fifty-two patients visiting the Research Center of Neurology and Bujanov Moscow City Clinical Hospital were selected for inclusion in the study and classified as having definite MS according to the criteria of McDonald15 and revised after new edition of criteria in 2017.16 All patients with RRMS were examined at the time of MS attacks. The exclusion criteria were forms of MS other than RRMS; comorbid neurodegenerative, psychiatric, or somatic pathology; history of alcohol or drug abuse; head trauma; vascular diseases and seizures; signs of severe depression; or receiving methylprednisolone pulse therapy less than 3 months before the study commenced. The application of these exclusion criteria during our screening resulted in the exclusion of 24 patients with MS. All of the MS patients were negative for anti-AQP4 antibodies.
The ADEM group consisted of nine patients with monophasic disease and large multifocal brain magnetic resonance imaging (MRI) lesions, but none of them had spinalcord injury. Since current diagnostic criteria for ADEM have been proposed for children17 but not for adults, ADEM was diagnosed according to the following clinical recommendations18: acute onset of multifocal neurologic symptoms, sometimes with a history of antecedent infection or vaccination, often with rapid deterioration prompting hospitalization, and nonspecific signs that can accompany ADEM include headache, fever, nausea, and vomiting, altered mental status and prominent neurological deficit, monophasic disease course, multiple demyelinating lesions with contrast enhancement, and noncontradictory CSF data. Our ADEM cases were monophasic during 2 years of follow-up.
The typical-NMO group consisted of 12 patients with an anti-AQP4-antibody-positive serum profile and clinical-MRI picture consistent with the criteria of Wingerchuk for NMOSD with AQP4-IgG positivity or typical NMO.19 All patients were examined at the time of acute attacks.
Neurological assessment, MRI of the brain and spinal cord, and sera examinations were performed in all patients. Neurological impairment was assessed by the Kurtzke Expanded Disability Status Scale (EDSS), which was used as an indicator of relapse severity. We did not apply the EDSS to ADEM patients since this tool is not helpful for assessing the degree of CNS damage in these patients.
The patients had not received any previous immunomodulatory or immunosuppressive treatment (it was their first visit to MS diagnostic center after the beginning of the disease) except for methylprednisolone pulse therapy more than 3 months before being included in the study. The clinical characteristics of the patients and the information about previous methylprednisolone treatment are presented in Table 1.
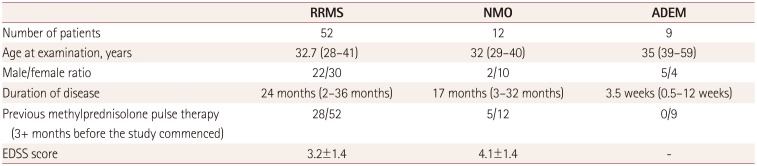
Table 1
Clinical characteristics of patients
![]()
Twenty-four healthy subjects were included in the control group (median age of 34.5 years, age range from 25 to 51 years). There were no significant differences in age or sex between the patient and control groups (p>0.05).
Fasted venous blood and CSF samples were collected from all patients and control subjects after they provided informed consents and before the initiation of treatment. The research protocol was approved by the Local Ethical Committees (IRB No. 5-12). The sera and CSF samples were prepared by centrifugation for 20 minutes at 1,500×g and 4℃. Supernatants were aliquoted into sterile tubes and stored at −70℃. Control CSF was sampled during spinal anesthesia in patients with surgical pathology. Control blood samples were obtained from healthy volunteers. A cell-based AQP4 assay kit (Euroimmune, Luebeck, Germany) was used for anti-AQP4 antibody measurement.
The levels of biomarkers in CSF samples were measured using the following commercially available ELISA kits: pNfh (Encore Biotechnology, Gainesville, FL, USA), and IL-6 and EPO (Vector Best, Novosibirsk, Russia). All procedures were performed according to the manufacturer's protocols. IL-6 was analyzed separately in unheated and heated CSF samples. According to the method described by Brailly et al.20 all CSF samples were heated at 56℃ for 20 minutes for the thermodestruction of soluble IL-6R. Total RSNO levels were assessed fluorometrically using 4, 5-diaminofluorescein (Cayman Chemical Company, Ann Arbor, MI, USA) according to Wink et al.21 Sample measurements were performed in duplicate, while calibration curves were determined in triplicate.
Statistica 8.0 (StatSoft, Tulsa, OK, USA) and GraphPad Prism 6 for Windows (GraphPad Software Inc., San Diego, CA, USA) were used for statistical analysis. Data are presented as median values with 25th and 75th percentiles. We used the nonparametric Kruskal-Wallis test for multiple comparisons (with a significant p value defined as <0.05) and the nonparametric Mann-Whitney U-test with Bonferroni correction for comparisons of patients with controls. Spearman correlations between biomarker levels and clinical data were calculated, and logistic regression was performed to determine significant associations of biomarker levels with outcomes.
Go to :
RESULTS
IL-6 and EPO levels
The serum IL-6 level appeared to be higher in the MS group, although the difference was not statistically significant (Fig. 1). The CSF IL-6 level before heating was higher in the ADEM and NMOSD with AQP4-IgG groups (2.9±0.8 and 3.1±0.3 pg/mL, respectively; mean±standard deviation) than in controls (0.8±0.2 pg/mL, p<0.05), but not in MS. After applying heating we found that the IL-6 levels had increased in the RRMS, NMO, and ADEM groups (p=0.01). We did not find correlations between serum and CSF IL-6 levels, which is consistent with reports on the intrathecal synthesis of IL-6.22 No correlations were found between IL-6 and RSNO levels, and a selective IL-6 elevation in spinal-cord injury was also not demonstrated. The EPO level was decreased in MS (39.7±4.0 vs. 49.8±9.0 mME/mL, p<0.01). None of the above indices were correlated with either clinical data or the levels of other biomarker (pNFh, IL-6, and RSNO).
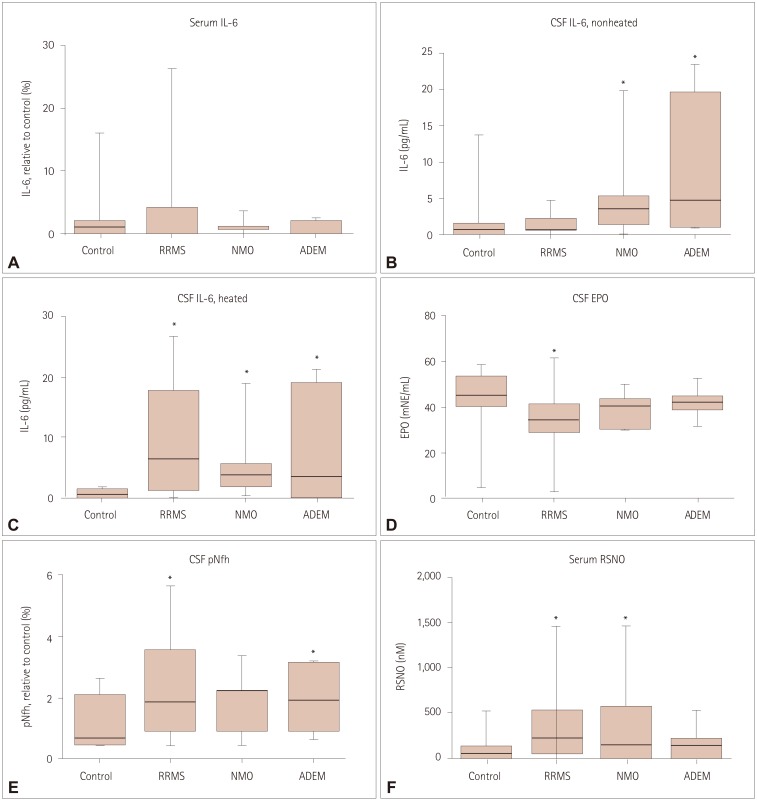 | Fig. 1Cytokines, pNfh, and RSNO levels in patients with different demyelinating disorders. Data are median values with 25th and 75th percentiles. A: Serum IL-6 levels were increased in the MS group. B: CSF IL-6 levels before heating were augmented in ADEM and NMOSD with AQP4-IgG but not in MS. C: CSF IL-6 levels after heating were elevated in the RRMS, NMOSD with AQP4-IgG, and ADEM groups. D: CSF EPO levels were decreased in the MS group. E: CSF pNfh levels were elevated in MS and ADEM patients but not in the NMOSD with AQP4-IgG group. F: Serum RSNO levels were increased in the RRMS and NMOSD with AQP4-IgG groups. *Used for statistically significant results (p<0.05). ADEM: acute disseminated encephalomyelitis, AQP4-IgG: aquaporin-4 immunoglobulin G, CSF: cerebrospinal fluid, EPO: erythropoietin, IL-6: interleukin-6, MS: multiple sclerosis, NMO: neuromyelitis optica, NMOSD: neuromyelitis optica spectrum disorders, pNfh: phosphorylated neurofilament heavy chain, RRMS: relapsingremitting multiple sclerosis, RSNO: S-nitrosothiols.
|
CSF pNfh level
The CSF pNfh levels were increased in MS and ADEM patients (p<0.05) but not in the NMOSD with AQP4-IgG group (Fig. 1).
Serum RSNO level
Using multiple comparisons, serum RSNO levels were higher in RRMS patients and NMO groups (p<0.05) (Fig. 1), although this difference did not reach statistical significance in paired comparisons with the control group (p>0.1). It was especially notable that RSNO was not correlated with other biochemical markers, and so did not confirm the hypothesis about IL-6-mediated NO production in spinal-cord lesions.13
Go to :
DISCUSSION
The main differential diagnoses in MS patients include NMOSD and ADEM. Despite having similar demyelinating CNS lesions, these pathologies have different pathogeneses, clinical manifestations, and treatment strategies. NMOSD and ADEM are potentially life-threatening and severely disabling conditions, with NMOSD often requiring immunosuppressive treatment. Additional data related to the role of IL-6 in differentiating between MS and other inflammatory demyelinating disorders have recently been reported.78 IL-6 was suggested to be a key molecule in the complementindependent driver of neuroinflammation and breakdown of the blood–brain barrier in anti-AQP4-antibody-positive disorders, and anti-IL-6 monoclonal antibodies therapy has been tried primarily in NMOSD.911
In the present study we found increased total IL-6 levels in NMOSD with AQP4-IgG and ADEM patients, in accordance with the previous report of Uzawa,8 and additionally in the MS group after the thermodestruction of soluble IL-6R. This method was used to measure total IL-6 in the patients (free and binding with soluble IL-6R), and we can suggest that the level of soluble IL-6R binding with IL-6 is higher in MS than in other demyelinating disorders, which supports previous findings.2324
A high level of soluble IL-6R may result in the involvement of soluble IL-6R-associated pathways in MS, while a membrane-IL-6R-dependent pathway is active in NMOSD and ADEM. However, there have been some contradictory results suggesting that the level of soluble IL-6R is higher in NMOSD.25
We were unable to confirm the hypothesis of IL-6 and NO-mediated spinal-cord-specific damage, which was previously suggested based on in vitro data13; no expected correlations between the RSNO and IL-6 levels were revealed. The EPO level was decreased in MS but not in other patients, which could be associated with the duration of chronic MS pathology being much longer than ADEM, and predominantly involving B-cell pathology in NMOSD.
There are some reports of an association between the IL-6 level and disease severity in NMO patients, which could be related to its ability to enhance the production of Th17 cytokines.1126 pNfh levels are used as clinical markers of progression in ALS patients and have been proposed for use in the disease-free status score in MS additional to the no evidence of disease activity in MS-4 scale.27 We measured pNfh levels in patients with different demyelinating disorders based on suggestions that this index is a general marker of disease severity. The CSF pNfh level was elevated in patients with MS and ADEM, but not in those with NMOSD with AQP4-IgG. The absence of pNFh increase in NMOSD with AQP4-IgG is in accordance with previous results supporting astrocytic pathology and indicating more-prominent glial fibrillary acidic protein elevation in NMOSD.28 Remarkably, we did not find any correlations between inflammatory markers and pNfh levels, which may be due to rapid neuroinflammatory activation in the acute stages of MS and ADEM and slower courses of neurodegeneration.29
Together our results reveal the existence of IL-6 activation in different demyelinating disorders, augmentation of nitrosylation in demyelinating disorders with spinal-cord injury, and signs of neurodegeneration in these patients. However, we did not find any correlations between these biochemical markers and did not confirm the hypothesis about IL-6-mediated NO production in spinal-cord lesions.
Go to :
 XML Download
XML Download