

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hemifacial spasm (HFS) is a movement disorder characterized by involuntary, irregular, and recurring contractions of the muscles innervated by the facial nerve.1 HFS mainly results from the compression of ipsilateral facial nerves by cerebral vessels,23 which rarely resolves spontaneously.4 Even though HFS is not a life-threatening disease, it can severely impair the quality of life.56 HFS is directly related to sleep disturbance and difficulty in performing daily activities such as reading and driving.78 Moreover, HFS is associated with various psychologic symptoms including low self-esteem, social embarrassment, social isolation, and depression.67
Despite the wide-ranging impact of HFS, the significance of its clinical features has not been clearly demonstrated. Only a few clinical characteristics of HFS have been reported previously and no consensus has been reached,91011 while various surgical findings including intraoperative severity of indentation or resolution of the lateral spread response were suggested to be related to surgical outcome.10111213 It is particularly notable that the severity of HFS is a clinical barometer that can be easily assessed in a clinic, but there is no consensus on how to evaluate spasm severity. We previously proposed the Samsung Medical Center (SMC, Seoul, Korea) grading system as a tool for evaluating HFS severity, and found that spasm severity was strongly correlated with quality of life.14
With the aim of elucidating the clinical meaning of HFS severity, we used the SMC grading system to evaluate HFS severity and compared clinical features, surgical findings, and outcomes between patients with severe- and mild-spasm.
METHODS
Subjects
This study was approved by the Institutional Review Board of SMC (2016-08-184). We retrospectively reviewed the medical records of patients with primary HFS, who 1) underwent microvascular decompression (MVD) between May 2010 and December 2013 at SMC and 2) were followed up for at least 6 months after MVD (Supplementary Fig. 1 in the online-only Data Supplement). Primary HFS is presumably caused by vascular compression of the ipsilateral facial nerve, and is the most common type among the patients who visited the clinic at SMC for HFS evaluations.1516 Brain magnetic resonance imaging (MRI) was applied to all subjects to evaluate neurovascular compression and to exclude any organic causes of HFS. MVD was considered in all primary HFS patients with neurovascular compression on brain MRI, unless their physical status was worse than American Society of Anesthesiologists class II (normal healthy patients or subjects with mild systemic disease).17 The application of these criteria resulted in 636 patients being recruited for this study.
We divided the enrolled subjects into two groups based on HFS severity as reported previously14: mild-spasm (SMC grade 1 or 2) and severe-spasm (SMC grade 3 or 4). The 636 enrolled subjects were divided into 327 in the mild-spasm group and 309 in the severe-spasm group.
Clinical and surgical data assessment
Demographic and clinical data including age at the time of MVD, disease duration, involved side, and comorbidities were collected. The clinical course of HFS was classified into three types: periocular onset (spasm presenting first in the periocular area), perioral onset (perioral involvement at symptom onset), and hemi onset (hemifacial area at onset).18 We also assessed the presence of HFS-related tinnitus resulting from spasm of the stapedius muscle, which is innervated by facial nerves.
The surgical findings of the patients were reviewed. The offending vessels and the presence/extent of indentation of the facial nerve root exit zone by compressing vessels were assessed in the surgical field and categorized into three grades: grade 1, no or mild indentation; grade 2, moderate indentation; and grade 3, severe indentation with discoloration. The degree of indentation reflects the severity of intraoperative neurovascular compression.12
Surgical outcomes were assessed at the outpatient clinic at 6 months after surgery. The subjects were divided into two groups based on their surgical outcome: successful (subjects with HFS resolved by at least 90%) and unsuccessful (patients with spasm relief of up to 90%).19
Patients were divided into the following six categories of complications: delayed facial palsy, hearing loss, ear effusion, tinnitus, surgery-related (infection, wound problems, leakage of cerebral spinal fluid, or hemorrhage), and other. Facial palsy with a grade of III or more on the House-Brackmann grading system was regarded as significant.20 Pure-tone audiometry (PTA) and the Speech Discrimination Score (SDS) were evaluated before and after MVD (usually at 3–10 days after surgery).21 A decrease of more than 15 dB from the postoperative bone-conduction average PTA threshold (at 500, 1,000, 2,000, and 3,000 Hz) or a decrease of more than 20% in the SDS relative to the baseline for each patient was defined as hearing loss.2223
Statistical analyses
All data are presented as mean±standard-deviation values. The significance of differences between the mild- and severe-spasm groups was evaluated using the independent Student's t-test or the Mann-Whitney U test for continuous and ordinal variables, while Pearson's chi-square test or Fisher's exact test was used for categorical variables. To identify variables related to HFS severity, multivariate analysis was carried out with a logistic regression model. The mild- and severe-spasm groups were included as the dependent variables, whereas age, involved side, disease duration, clinical course, hypertension (HTN), diabetes mellitus (DM), heart/lung disease, stroke, complications (facial palsy, hearing loss, ear effusion, tinnitus, surgery-related, and other), and outcome were included as controlled variables. The logistic regression results are presented using odds ratios with 95% confidence intervals. Probability values of p<0.05 were considered statistically significant. All statistical analyses were performed using commercially available software (PASW for Windows, version 18.0, SPSS Inc., Chicago, IL, USA).
RESULTS
Comparison of clinical features between the mild- and severe-spasm groups
The demographic and clinical data of the mild- and severe-spasm groups are presented in Table 1. The severe-spasm group was older at the time of MVD and had a longer disease duration than the mild-spasm group. The age at symptom onset did not differ significantly between the mild-spasm group (46.2±11.1 years) and the severe-spasm group (44.7±9.9 years, p=0.073). There was also no significant intergroup difference in any of the other demographic data or HFS clinical features. Of the examined comorbidities, HTN, and DM were more common in the severe-spasm group than in the mild-spasm group.
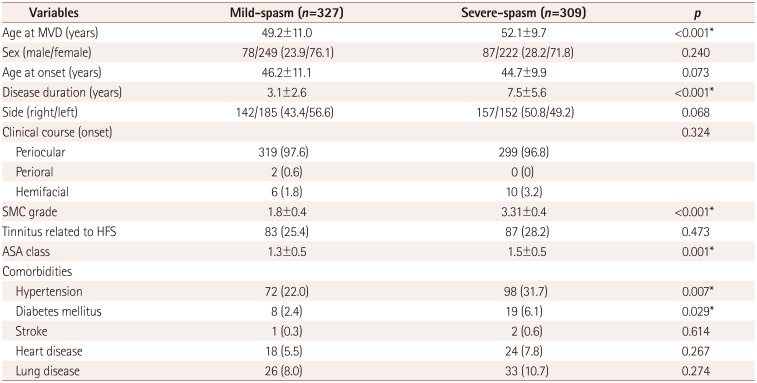
Table 1
Comparison of demographic data between the mild- and severe-spasm groups
![]()
Comparison of surgical findings and outcomes between the mild- and severe-spasm groups
While there was no significant difference in the number of offending vessels, multiple offenders were more common in the severe-spasm group than in the mild-spasm group (Table 2). In addition, indentation was more severe in the severe-spasm group than in the mild-spasm group.
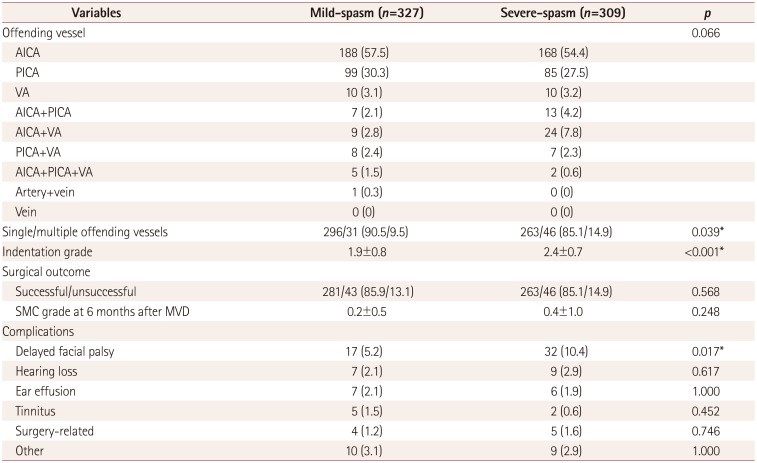
Table 2
Comparison of surgical findings and outcomes between the mild- and severe-spasm groups
![]()
A successful outcome after MVD was reported in 86.9% of the 636 enrolled subjects, with no difference in rate of successful outcome between the mild- and severe-spasm groups. There were more complications in the severe-spasm group (18.1%) than in the mild-spasm group (14.4%), but the difference was not statistically significant. The complication of delayed facial palsy was more common in the severe-spasm group than in the mild-spasm group, while there were no intergroup differences in any of the other complications.
Multivariate analysis of the relationship between HFS severity and other variables
We performed logistic regression analysis to identify variables associated with HFS severity. The mild- and severe-spasm groups were included as the dependent variables, while age, involved side, disease duration, clinical course, HTN, DM, heart/lung disease, stroke, complications (facial palsy, hearing loss, ear effusion, tinnitus, surgery-related, and other), and outcome were included as controlled variables (Table 3). Severe-spasm was significantly associated with longer disease duration, HTN, multiple offending vessels, severe indentation, and more delayed facial palsy after MVD.

Table 3
Results of a multivariate analysis to identify variables associated with the severe-spasm group
Age, involved side, disease duration, clinical course, comorbidities (hypertension, diabetes mellitus, heart/lung disease, and stroke), complications (delayed facial palsy, hearing loss, ear effusion, tinnitus, surgery-related, and other), and outcome were included as controlled variables.
CI: confidence interval, MVD: microvascular decompression, OR: odds ratio.
![]()
DISCUSSION
This is the first study to investigate the clinical implications of HFS severity in patients with HFS. Although many previous studies have examined predictors of the prognosis of HFS after MVD, they predominantly investigated intraoperative findings rather than clinical features.10111213 Unlike previous studies, we focused on the clinical characteristics of HFS. Our reasoning was that the treatment modality should be decided based on both clinical features and intraoperative findings. Our patients with severe HFS had a longer disease duration and more-severe indentation, and were also more likely to have multiple offending vessels and HTN. A particularly interesting finding was that among the surgical complications examined, delayed facial palsy was related to spasm severity whereas the rate of successful outcomes was not.
HFS severity has previously been shown to be independently related to quality of life,24 but the role of spasm severity in patients with HFS has not been investigated. Only one study found that severe HFS was related to headaches in patients with HFS.25 Since HFS can present with various clinical characteristics, such as clonic or tonic spasms, differences in the involved area or fluctuations therein could make it difficult to assess all spasms on a single grading scale. Moreover, there is currently no consensus on how to evaluate HFS severity. A previous study suggested using the SMC grade as a measure of HFS severity, and found this to be strongly correlated with the quality of life in patients with HFS.14 Additionally, higher SMC grade was associated with longer disease duration, which is in accordance with our results. However, none of the previous studies directly evaluated the relationships between spasm severity and surgical findings, outcomes, and complications.
We found that HTN and DM were more common in the severe-spasm group than in the mild-spasm group. Moreover, HTN was significantly associated with severe-spasm in the regression analysis. Similarly, when we compared clinical features between elderly patients with HFS and younger patients in a previous study, the elderly patients with HFS showed more severe-spasms and were more likely to have HTN and DM.18 Considering that the age at MVD was not associated with spasm severity in the multivariate analysis performed in the present study, the severity of HFS might not be directly related to age, but rather to other conditions such as HTN or disease duration. Previous studies have also focused on the association between vascular dolichoectasia and HFS, concluding that dolichoectasia is usually associated with HTN.2627 However, conflicting results have been obtained regarding the relationship between HFS and HTN,282930 and no study has focused on HTN and spasm severity in patients with HFS. Future studies investigating the association between HTN and HFS pathophysiology will help to elucidate this relationship. Regarding DM, there have been only a few reported cases supporting the possibility of a relationship between hyperglycemia and HFS,3132 and DM was not associated with spasm severity in the multivariate analysis in the present study; caution is therefore required when interpreting these results.
When we compared surgical findings between the mild- and severe-spasm groups, we found that severe indentation and multiple offending vessels were associated with severe spasms. Although the surgical outcomes did not differ between the severe- and mild-spasm groups in our study, the degree of indentation and multiple offenders could be important because many previous studies have found these surgical findings to be associated with surgical outcome.11121333 Moreover, indentation has been reported to be associated with delayed facial palsy and disease duration,34 and we also found that HFS severity was independently related to disease duration, indentation degree, multiple offending vessels, and delayed facial palsy. Based on our results, spasm severity could be regarded as a biomarker of the degree of pathologic compression in patients with HFS.
Another particularly interesting finding of the present study was that the severe-spasm group was independently associated with delayed facial palsy. Although the etiology of delayed facial palsy has not been clearly elucidated, it has been shown to be associated with a higher degree of indentation and longer disease duration.34 Considering that severe indentation with longer disease duration could aggravate demyelination of the facial nerve, more time would be needed to repair the damage after the offending vessel is removed.34 Additionally, more delayed facial palsy has been reported in HFS patients with multiple offending vessels, although this difference was not significant.34 That study suggested that the presence of multiple offenders hinders surgery, resulting in a greater risk of facial nerve damage. However, we found that severe-spasm was independently associated with multiple offenders and delayed facial palsy, indicating that there might be direct relationships between severe-spasm, multiple offending vessels, and delayed facial palsy. Various other risk factors for delayed facial palsy after MVD have also been suggested,353637 and so further studies are required to elucidate the pathophysiology of delayed facial palsy after MVD.
Besides delayed facial palsy, spasm severity was not associated with any other complication or surgical outcome in our study, in contrast to previous studies finding indentation and multiple offending vessels to be associated with surgical outcome.11121333 This discrepancy can be attributed to the effects of various factors including age, disease duration, comorbidities, and psychologic status on surgical outcomes and complications.918 Although we observed that facial palsy was delayed in the severe-spasm group, the complication rate was still low and so MVD could be an effective treatment option for patients with HFS. Since treatment modalities are selected and complications are predicted based on clinical or laboratory findings, rather than on intraoperative findings, more studies focusing on the clinical features of HFS—like the present study—are important for providing doctors with the best information possible for making appropriate decisions.
MVD was performed in 626 patients with primary HFS in this study, of whom 554 (85.5%) reported complete relief or minimal symptoms. The rate of successful outcomes in the present study was slightly lower than those in our previous studies.121338 However, considering the delayed cure after MVD and the relatively short follow-up period (6 months after MVD) in this study, our results are comparable with those of previous studies. Furthermore, we used different tools to evaluate the surgical outcomes compared to previous studies due to the lack of a consensus on how to assess surgical outcomes. The complication rates in the current study were similar to those in a previous study.38
This study was subject to some limitations. First, we only enrolled patients with HFS who underwent MVD and were followed up for at least 6 months. Considering that the cure was delayed after MVD, the improvements might have been greater and the complication rate lower if we had used a longer follow-up period.13 However, since we wanted to focus on the clinical characteristics of HFS in as many subjects as possible, we assessed surgical outcomes and complications for only 6 months after MVD. Second, the severe-spasm group was older than the mild-spasm group. As we reported previously, elderly patients may exhibit specific characteristics for HFS.18 However, a previous study found no difference in the prevalence of delayed facial palsy between elderly and younger patients with HFS. Moreover, to minimize possible confounding effects of age or comorbidities, we used multivariate logistic regression analysis in this study. Third, recall bias might have been present in the clinical history because most of the collected data were self-reported and the overall disease duration was 5.2±4.9 years.
In conclusion, although MVD is an effective treatment option for patients with severe HFS as well as for patients with mild-spasm, surgeons should carefully monitor patients with severe HFS due to the greater risk of delayed facial palsy. In addition, spasm severity could be used as a marker of pathologic compression in patients with HFS who need MVD.
 XML Download
XML Download