

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
With immunocompromising hosts, the elderly, international exchange and economic development, the epidemiology of dermatophytosis has been changing worldwide. The epidemiological data on dermatophytosis in Korea also showed enormous changes. Trichophyton schoenleinii was the most important causative fungus of tinea capitis in Korea in 1950s. However, it has not been found in Korea since 1980s. On the contrary, Trichophyton tonsurans has been found as one of the causative factors of dermatophytosis in Korea since 1990s1. Therefore, it is important to investigate the epidemiological and mycological changes of dermatophytosis for improving the personal health and storing the medical data. Microsporum gypseum is a cosmopolitan geophilic dermatophyte, frequently found in contaminated soil. It usually causes an inflammatory superficial dermatophytosis in the scalp and glabrous skin in humans and rarely develops onychomycosis. However, its prevalence among dermatophyte infections is very low23. Infection with M. gypseum accounts for less than 0.19% of superficial dermatophytosis in Korea4. In addition, there are few reports on the infection due to M. gypseum in the literature. The aim of this study is to add massive data on M. gypseum to the literature and to provide useful information on clinical and mycological characteristics of M. gypseum.
Go to : 
MATERIALS AND METHODS
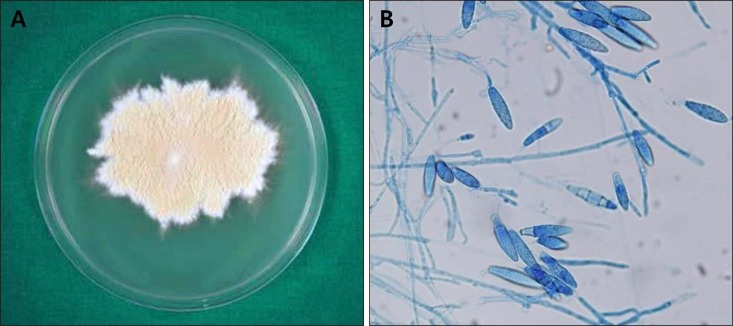
The medical records of 198 cases with M. gypseum infection were retrospectively investigated. This study was approved by Institutional Review Board of Kyungpook National University Hospital (IRB no. 2017-11-001). Most patients included in this investigation had lived in the southeastern area of South Korea. M. gypseum infection was diagnosed at Kyungpook National University Hospital and the Catholic Skin Disease Clinic from 1979 to 2016. The identification of M. gypseum was done with mycological examination using 15% KOH preparation and potato corn meal tween 80 agar culture media. The culture media were kept at 24℃ to 26℃ from 2 to 4 weeks. KOH-positive patients were 171 out of 198 (86.4%) who were culture-positive. M. gypseum grown on the culture media showed brownish, powdery or granular colony (Fig. 1A). Latophenol cotton blue stain showed fusiform symmetrical thin-walled macroconidia with 3 to 6 cells (Fig. 1B).
Go to :
RESULTS
Incidence of M. gypseum
The incidence of M. gypseum infection is very low in South Korea. In addition, Fig. 2 shows a tendency to decrease in the incidence of M. gypseum. However, M. gypseum infection still remains around us until recent years. From 1980s to 2000s, M. gypseum infection was much more frequent in young children (0~9 years old) than any other age group (Table 1). They accounted for 22.6% to 39.7% of all patients with M. gypseum infection. However, the fifties showed the highest incidence in 2010s (25.0%) (Table 1). M. gypseum infection was most common in September in 1980s (21.3%) and in August in 1990s (17.5%) (Table 2). Tinea faciei was the most common clinical type in 1980s (38.8%) (Table 3). Tinea corporis became most common clinical type from 1990s (39.7%) to 2010s (66.7%) (Table 3).
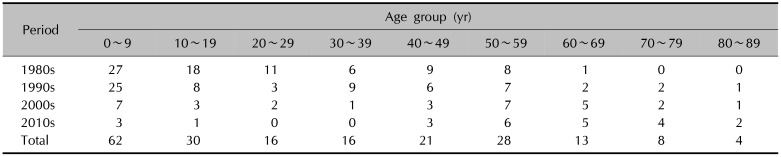



Table 1
Chronological distribution of Microsporum gypseum infection according to age
![]()
Table 2
Chronological distribution of Microsporum gypseum infection according to month
![]()
Table 3
Chronological distribution of Microsporum gypseum infection according to topography
![]()
Sex and age
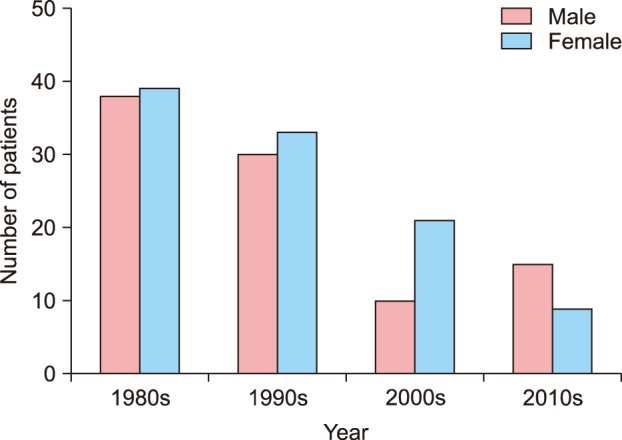
Out of 198 cases, men were 94 cases (47.5%) and women were 104 cases (52.5%) (Table 4). M. gypseum infection was more frequent in women than in men until 2000s (Fig. 3). After then, it was more frequent in men (Fig. 3). Mean age of all patients was 29.83 years old: 24.97 years old in men and 34.22 years old in women. The most common age group with M. gypseum infection were young children (0~9 years old, 31.3%) followed by teenagers (15.2%) and fifties (14.1%) (Table 1). Men were more common than women in the age group of 0 to 19 years old (Fig. 4). On the contrary, women were more common than men in the age group of above 20 years old (Fig. 4). Furthermore, young children (0~9 years old) were most common and the fifties was the next in the incidence of M. gypseum infection in women (Fig. 4).


Seasonal variation
M. gypseum infection occurred most frequently in September (16.7%) and August (16.2%) (Table 2). Tinea faciei was most common in February, tinea corporis in August, and tinea cruris in September (Table 5).
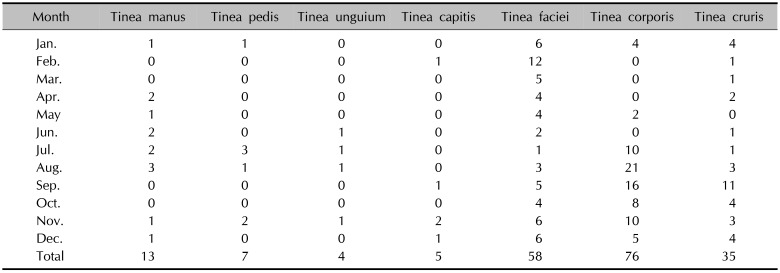
Table 5
Monthly distribution of Microsporum gypseum infection according to topography
![]()
Topographical distribution
M. gypseum usually caused dermatophytosis on the glabrous areas. The most common clinical type of M. gypseum infection was tinea corporis (38.4%), followed by tinea faciei (29.3%), tinea cruris (17.7%) (Table 3). However, the most common M. gypseum infection of men was tinea cruris followed by tinea corporis and tinea faciei (Table 4). In addition, the most common M. gypseum infection of young children (0~9 years old) was tinea faciei (Table 6). Furthermore, the most common M. gypseum infection of teenagers was tinea cruris (Table 6).
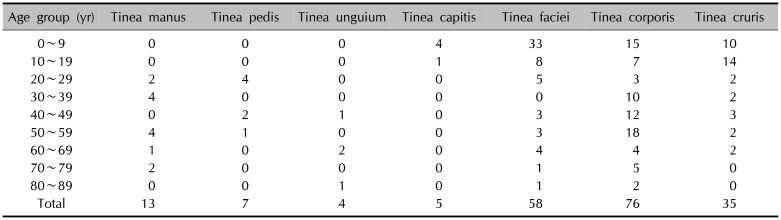
Table 6
Age distribution of Microsporum gypseum infection according to topography
![]()
Go to :
DISCUSSION
M. gypseum has been isolated from infected animal and especially contaminated soil worldwide. This has also been isolated from South Korea since 1966. However, the incidence of M. gypseum infection is very low. Trichophyton rubrum, Trichophyton interdigitale, T. tonsurans and Microsporum canis have become the major species of dermatophytosis globally5. Especially, T. rubrum is the most common dermatophyte, accounting for 80% to 90% of all isolated dermatophytes67. Romano et al.3 reported that the incidence of dermatophytosis caused by M. gypseum in Siena was 6.8% of all dermatophytic infections. They investigated 14 cases of M. gypseum infection between 2004 and 2005. Sei2 also conducted an epidemiological survey of dermatophytosis. The survey showed M. gypseum was isolated from only 3 outpatients out of 36,052 outpatients. Only a few cases with M. gypseum infection have also been reported in South Korea. The first two cases of M. gypseum infection were published by Kim and Suh8 in South Korea in 1976. After then, eight cases was investigated by Jun and Suh9 in 1980. We retrospectively analyzed big data of 198 cases from 1979 to 2016. As reported in Italy and Japan, the annual incidence of M. gypseum infection was very low. Although the incidence of M. gypseum infection showed a decreasing tendency, it still remained around us.
When we began this study, it was expected that middle-aged adults living in rural area were most frequently infected, because they had always been working in the yards or gardens as farmers. On the contrary to our expectation, M. gypseum was most frequently isolated in young children. Especially in 1980s, the incidence of M. gypseum infection in young children was highest. Jun and Suh9 also reported young children was the most common age group of M. gypseum infection. In recent years, young adults were most frequently infected by M. gypseum. Improvement of hygiene and easy accessibility to hospitals might lead the decrease in incidence of M. gypseum infection in young children in recent years. On the other hand, Lee et al.6 reported T. rubrum was most frequently infected in the middle-aged group. It is written in the literature that Trichophyton mentagrophytes was also most frequently infected in the middle-aged group10. However, M. canis infection was usually developed in young children in South Korea11. In addition, this report was published that T. tonsurans infection occurred most frequently in the teenager group11. Furthermore, it was reported that anthropophilic dermatophytes, such as Trichophyton violaceum, T. tonsurans and Microsporum audouinii are causing outbreaks of small epidemics of tinea corporis and tinea capitis in young children and teenagers12. The incidence of M. gypseum infection was higher in women than in men out of our expectation. However, men were higher than women in the young children group.
Although tinea corporis was the most common clinical type of M. gypseum infection, tinea cruris was most common in men. In addition, tinea faciei was the most common clinical type of M. gypseum infection in young children and tinea cruris in teenagers. According to annual incidence, tinea faciei was most common clinical type of M. gypseum infection in 1980s, but tinea corporis became the most common clinical type of M. gypseum infection from 1990 to 2016. Improvement of hygiene, interest in beauty and health, and easy accessibility to hospitals might decrease in incidence of tinea faciei caused by M. gypseum in recent periods. On the other hand, Trichophyton rubum usually causes tinea pedis and tinea unguium5. Trichophyton metagrophytes also usually causes tinea pedis9. M. canis is a major cause of tinea capitis5. T. tonsurans is also an important cause of tinea capitis5.
The incidence of M. gypseum infection was highest in hot season including September and August. Interestingly, the incidence of tinea faciei caused by M. gypseum was highest in February. It is found in the literature that M. canis showed higher incidence in winter than in any other seasons10. T. tonsurans occurs commonly in the spring11. However, T. rubrum and T. mentagrophytes usually develop dermatophytosis in hot season89.
In conclusion, our study, including a lot of patients for a long period, will provide very useful information on dermatophytosis caused by M. gypseum in the field of medical mycology.
Go to :
 XML Download
XML Download