

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Clinically isolated syndrome (CIS) describes the first clinical neurological episode when a patient has symptoms and signs suggestive of multiple sclerosis (MS). It usually occurs in young adults involving optic nerve, brainstem or spinal cord. CIS is often the first manifestation of MS.1 About two thirds of patients presenting with CIS will have further clinical episodes or new lesions at MRI and convert to relapsing-remitting MS.2
McDonald criteria for MS diagnosis have been revised over the years-McDonald's 2001,3 2005,4 20105-and the new update was formulated in 2017.6 With these amendments, diagnostic procedures have been simplified and earlier diagnosis facilitated.
The 2010 revisions of the McDonald criteria for MS5 have introduced important changes in the clinical approach, with possibility of diagnosis at the first observation. In fact, for the first time, a single MRI examination allowed the diagnosis of MS, if dissemination of lesions in space (DIS) and time (DIT) were demonstrated without a no better explanation. The criteria for DIS were defined by 1 or more lesions in at least 2 of 4 typical areas of the CNS (periventricular, juxtacortical, infratentorial, and spinal cord). DIT was defined by presence of an asymptomatic gadolinium enhancing lesion and a T2 lesion or a new T2 lesion at a follow-up MRI.
The new 2017 revision of McDonald criteria 6 introduces other important changes, with a further simplification for the diagnosis. Aim of the revision is to facilitate earlier diagnosis and to preserve the specificity of the 2010 McDonald criteria reducing the frequency of misdiagnosis. The first important change is the introduction of the presence of oligoclonal bands (OCBs) in cerebrospinal fluid (CSF) to make the diagnosis of MS in a patient with evidence of DIS, allowing for substitution of DIT. The second major change is that either symptomatic or asymptomatic gadolinium enhancing lesions can be considered in determining DIS and DIT. Moreover, cortical lesions can be used in addiction to juxtacortical ones to support DIS.
Go to : 
METHODS
The aim of the paper is to show, through the discussion of typical CIS patients, how the application of the new criteria can change the diagnostic approach with respect to the previous criteria. The patients gave their consent for research.
Go to :
RESULT
Case 1
A 23-year-old woman came to our observation complaining of left side hypoesthesias from the mammillar line and paresthesias in the hands, which lasted about one week. She had no medical history and assumed estroprogestinic therapy.
At entry, neurological examination revealed left hypoesthesia with D5–D6 level, reduction of superficial abdominal reflexes to the left side, brisk deep tendon reflexes, no weakness, no Lhermitte sign and no sphincter dysfunction. Disability was 2, 5 Expanded Disability Status Scale (EDSS) points according to Kurtzke's scale.7
Multimodal evoked potentials were normal. We excluded systemic pathologies and other CNS diseases. Anti-aquaporin-4 (anti-AQP4) and anti-myelin oligodendrocyte glycoprotein (anti-MOG) antibodies resulted negative. CSF examination revealed normal cell count and the presence of OCBs.
Brain MRI showed T2-weighted lesions involving right centrum semiovale and left frontal lobe (Fig. 1A–D). Spinal MRI showed two enhancing lesions at C2 and D1–D2 level (Fig. 1E–H).
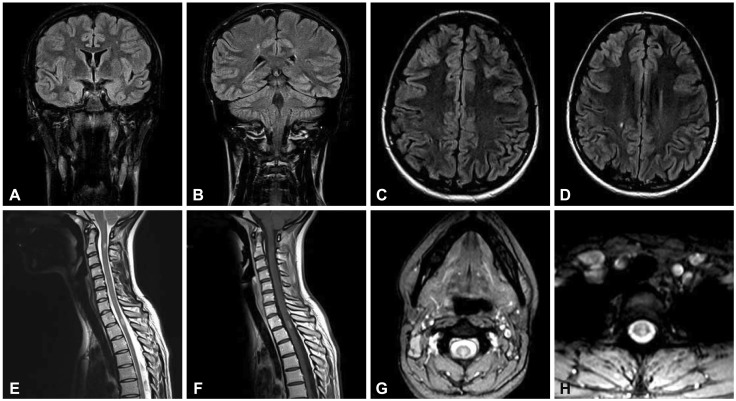 | Fig. 1Brain coronal plane FLAIR-weighted and axial plane T2-weighted scan showing hyperintense lesions in the left frontal lobe (A and C) and in right centrum semiovale (B and D), spinal cord sagittal and axial plane T2-weighted showing hyperintense lesions at C2 (E and G), and D1–D2 level (E and H), with enhancement on T1 post-Gadolinium scan (F).
|
Diagnosis of MS can be made with the new criteria, but not with the 2010 criteria. The criteria for DIS and DIT are now respected, including the enhancing lesions of the spinal cord, although both are symptomatic (C2 for hands paresthesias and D1–D2 for left side hypoesthesia). In fact either symptomatic or asymptomatic gadolinium enhancing lesions can be considered in determining DIS and DIT.
Case 2
A 27-year-old man came to our observation complaining from one week of blurred vision in the left eye with pain during ocular movements. No significant medical event had occurred previously.
At entry, neurological examination showed impaired vision in the left eye with normal pupillary light reflex, brisk deep tendon reflexes. At ophthalmologic investigation, visual acuity was 1/10 in left eye with normal fundus oculi. Disability was 4, 5 EDSS points.
Visual evoked potentials (VEP) showed increased latency (134 ms) and decreased amplitude of the left P100 wave; motor evoked potentials proved increased latency and decreased amplitude with wave dispersion and increased central conduction time at right lower limb; sensory and auditory evoked potentials were normal. Other CNS diseases were excluded, in particular neuromyelitis optica spectrum disorders (NMOSD) with negativity of anti-AQP4 and anti-MOG antibodies. OCBs were detected in the CSF that presented normal cell count.
Brain MRI showed multiple focal T2-weighted periventricular, cortical-juxtacortical, and infratentorial lesions and in left optic nerve (Fig. 2A–C and E). Spinal cord MRI showed multiple T2-weighted hyperintensity (Fig. 2D). None of these lesions presented enhancement (Fig. 2F–H).
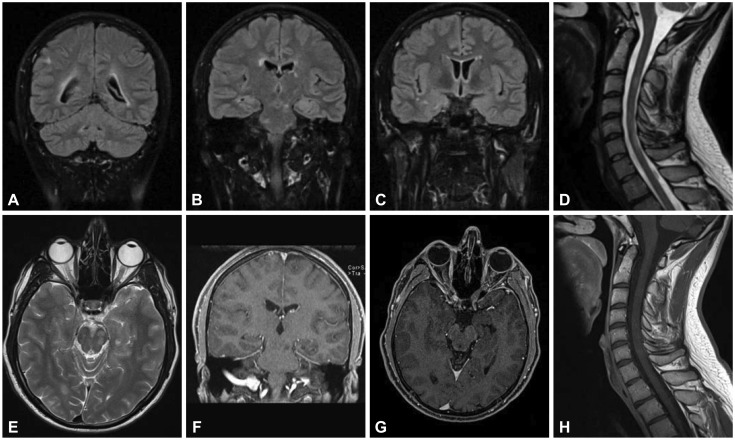 | Fig. 2Brain coronal plane FLAIR-weighted scan showing hyperintense juxtacortical (A), periventricular and infratentorial lesions (B and C) without enhancement on T1 post-Gadolinium scan (F and G), axial plane T2-weighted scan showing slight signal hyperintensity in left optic nerve (E), spinal cord sagittal plane T2-weighted showing hyperintense lesions at multiple levels (D) without enhancement on T1 post-Gadolinium scan (H).
|
Also in this case, diagnosis of MS can be made with the new criteria, but not with the 2010 criteria. Other diseases were excluded and the criteria for DIS but not for DIT are respected. The diagnosis of MS is possible because the presence of OCBs allows for substitution of DIT.
Case 3
A 24-year-old-woman came to our observation about ten days after acute onset of blurred vision in the right eye associated with slight pain with ocular movements. Her past medical history was silent.
At entry, neurological examination was normal, except for impaired vision in the right eye with normal pupillary light reflex. Ophthalmologic investigation revealed visual acuity 2/10 in the right eye and optic disc with shallow nasal margin. Disability was 3 EDSS points.
VEP showed increased latency (140 ms) and decreased amplitude of the right P100 wave. Optical coherence tomography (OCT) proved a slight thinning of the right retinal nerve. We excluded other CNS, autoimmune diseases and acute ischemic optic neuropathy. Anti-AQP4 and anti-MOG antibodies resulted negative. CSF examination revealed normal cell count and the presence of OCBs.
Brain MRI showed a T2-weighted lesion in the left peritrigonal white matter and slight hyperintensity in the right optic nerve (Fig. 3A and B). No enhancing lesions were detected. Spinal cord MRI showed normal findings.
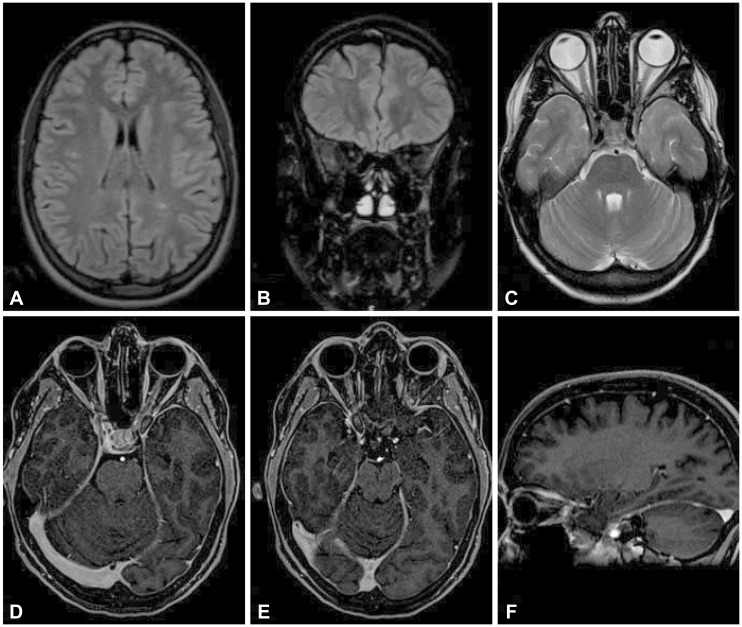 | Fig. 3Brain axial plane FLAIR-weighted scan showing hyperintensity of the left peritrigonal white matter (A) and coronal and axial plane FLAIR-weighted scan showing slight hyperintensity in the right optic nerve (B and C) without clear enhancement on T1 post-Gadolinium axial and sagittal scan (D, E, and F).
|
Following high dose methylprednisolone treatment (1g daily iv for 5 days), visual acuity returned to normal limits over two weeks, with a residual relative afferent pupillar defect.
In this case MRI data were inconsistent with DIS. In fact optic nerve is not a typical area for MS. Despite the presence of OCBs, diagnosis of MS cannot be allowed.
Go to :
DISCUSSION
We describe 3 typical cases of patients admitted to our hospital for CIS. We underline the differences between 2010 and 2017 criteria for MS diagnosis and discuss the advantages of this further revision in the clinical practice. The first implication is the anticipation of MS diagnosis. As a matter of fact, in the first two cases herein presented, the diagnosis of MS was achieved at clinical onset according to the new criteria, while with the previous criteria the diagnosis would have remained as CIS. In all three patients NMOSD diagnosis was carefully excluded.
The first patient presented an acute transverse myelitis. Brain MRI showed three T2 lesions, while spinal MRI showed two symptomatic T1-weighted gadolinium-enhancing lesions. According to the new criteria, diagnosis of MS could be performed, with demonstration of DIS and DIT. Based on the previous criteria, symptomatic enhancing lesion(s) did not satisfy DIT criteria. The MRI in MS (MAGNIMS) group has recently suggested no distinction should be made between symptomatic and asymptomatic MRI lesions.8 In fact, some studies reported that the presence of a symptomatic lesion identified patients with MS with a high sensitivity and accuracy and without compromising specificity.91011
The second report describes a CIS patient in whom MRI showed numerous T2 lesions suggestive of DIS. The diagnosis of MS would not have been possible with the 2010 criteria, in the absence of at least one gadolinium-enhancing lesion. With the new criteria, even if in absence of DIT, MS diagnosis was possible for the presence of OCBs in CSF.
OCBs reassume now a more relevant role in the MS workup. In 2010 criteria “the Panel reaffirmed that positive CSF findings (elevated immunoglobulin G index or 2 or more OCBs) can be important to support the inflammatory demyelinating nature of the underlying condition, to evaluate alternative diagnoses, and to predict clinically definite MS.” In the 2001 and 2005 a positive CSF finding could be used for reaching diagnosis in case of incomplete MRI findings. Now OBCs can be viewed as substitution for the DIT requirement. Its prognostic value remains undiscussed12: CIS patients with positive OCBs are more than twice as likely to having a second attack as OCB-negative ones, independently from MRI findings.131415 Patients both with OCBs and several T2 lesions present a risk at almost 90% of developing MS within five years.13 The presence of OCBs is the best biological marker to predict conversion to MS and it is associated with a shorter time conversion.14
The third case is a typical optic neuritis (ON) with hyperintense lesion on the right optic nerve. More than one third of CIS are ON. It is important to note that optic nerve is not included as a typical area and should not be considered either for DIS or for DIT. In this case, diagnosis of MS cannot be performed with the new criteria. This patient should therefore be considered as CIS.
The role of optic nerve lesions is debated. In fact, in the MAGNIMS consensus guidelines, the expert panel proposed that lesions in the optic nerve should be added to the criteria for DIS as an additional CNS area.8 It is known that patients presenting with ON as first attack have a lower risk for conversion to MS than patients with other presentations, even if the crucial issue at MS presentation is not CIS topography but MRI at baseline. In fact if a patient with ON has abnormal baseline MRI, his prognosis does not differ from that of other different CIS.16 The 2017 revision of McDonald criteria states that studies to validate MRI, VEP, or OCT in fulfilling DIS or DIT in support of a MS diagnosis are identified as high priority. OCT detects thinning of the retinal nerve fiber layer in the eyes of patients with MS and is important to identify the presence of a unilateral ON in MS.17 In addition, there are other possible future OCT markers of MS disease activity: macular ganglion cell layer+inner plexiform layer for brain atrophy and inner nuclear layer thickness for inflammatory activity.18
An anticipated diagnosis of MS may avoid further clinical and MRI monitoring to support the clinical conclusion, and allow a preventive discussion and counseling for the patients. However, more simplified criteria do not imply an easier diagnosis for clinicians. A correct interpretation of symptoms and signs, atypical symptoms and red flags, to obtain no better explanation,1920 remains mandatory. To avoid misdiagnosis, during evaluation of patients with suspected MS, a careful assessment is necessary, in particular for NMOSD, in fact in some cases uncertainty can occur, particularly with AQP4-seronegative patients.6
Finally, the access to disease modifying therapies to prevent further clinical or radiological dissemination could be anticipated and extended to more patients.
In conclusion, the new 2017 MS criteria may have an important impact in clinical practice: leading to an earlier diagnosis, to an increase in MS cases being diagnosed, anticipating patients' counselling and treatment to avoid the risk of disease dissemination. However, their application requires a more careful assessment of the patients (including CSF analysis) to avoid misdiagnosis and mistreatments, taking into account that many of them are characterized by non-negligible and partly still unknown long-term systemic effects.
Go to :
 XML Download
XML Download