

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Brucellosis is a growing global health problem as a result of increased international travel that permits the spread of the infection from endemic areas to other parts of the world [123]. It is caused by Brucella, a small, slow growing, intracellular Gram-negative coccobacillus that is transmitted to humans by direct contact with infected animals or intake of contaminated raw animal products, such as unpasteurized milk [14567]. Brucellosis almost always causes fever, which may be associated with night sweats [58]. Common treatment includes doxycycline and aminoglycosides, although complicated cases, such as brucellosis combined with endocarditis, osteoarticulitis, or neurobrucellosis, may require stronger medicatinos administered for a longer duration [91011]. Brucellosis is endemic to the Mediterranean basin, the Persian gulf, India, Mexico, and South America [1]. In Korea, the first human case was reported in 2002 [12]. Brucellosis in Korea is normally caused by Brucella abortus from cattle [5]. There have been no reported cases of brucellosis resulting from Brucella melitensis in Korea until now [12]. This paper presents a case of spondylitis complicated by B. melitensis infection that resulted from ingesting contaminated sheep meat while in Iraq.
Case report
A 48-year-old male Korean construction worker with no medical history developed fever and back pain while working in Karbala, Iraq. The patient went to a local hospital, where he received an intravenous steroid injection and oral antibiotics. After his fever spiked to 40°C and his back pain worsened, the patient received 4 days of intravenous antibiotics. When the fever and back pain failed to improve, the patient returned to Korea for further evaluation. The patient was transported to a tertiary hospital in Seoul, Korea that was in the midst of an outbreak of Middle East Respiratory Syndrome (MERS). Due to the patient’s fever and recent travel to Iraq, he was isolated for 72 hours until a sputum test for MERS-CoV came back negative. On admission, the patient’s vitals were as follows: blood pressure 138/92 mmHg, pulse rate 84 beats per minute, respiratory rate 18 breaths per minute, and body temperature 39° C. Laboratory tests showed a white blood cell count of 9,900/mm3 with 60% neutrophils, hemoglobin level of 14.2 g/dL, platelet count of 176,000/mm3, erythrocyte sedimentation rate (ESR) of 24 mm/hr, and C-reactive protein level of 116.7 mg/L (normal range, 0-8 mg/L).
The patient had recently undergone subgingival curettage, so a transthoracic echocardiography was performed to check for infective endocarditis. An MRI of the spine was also performed to evaluate the patient’s back pain. No vegetation was seen during the echocardiography, but the MRI revealed pyogenic spondylitis involving L5 with phlegmon and showing posterior extension to the epidural space at the L5 and S1 levels (Fig. 1). Meanwhile, the Brucella spp. was isolated on three separate blood cultures using MacConkey, and Brucella agars (Fig. 2). As such, we concluded that our patient had brucellosis causing infectious spondylitis [3]. We did not perform the bone biopsy or standard tube agglutination test.
 | Figure 1T2 added sagittal magnetic resonance image (contrast) of the lumbar spine taken on the third hospital day, showing pyogenic spondylitis involving L5 with phlegmon as well as posterior extension to the epidural space at the L5 and S1 levels (arrows).
|
 | Figure 2Gram stain of patient’s blood culture on the third hospital day. On Gram stain, the organisms appeared as faintly stained, Gram negative coccobacilli (×400).
|
We subsequently took a thorough history in order to determine the route of infection while waiting for lab results regarding the brucellosis subspecies [2]. The patient reported attending barbeque parties that served sheep meat every 2-3 weeks during his 6-month stay in Iraq. The patient further reported consuming undercooked sheep meat and pasteurized milk on several occasions during these parties. Since brucellosis is usually transmitted from contaminated sheep and goat products, we concluded that this was the likely route of contamination [2]. The patient denied other contact with animals while in Iraq.
We initially began treatment with ceftriaxone (2 g/day) and vancomycin (45 mg/kg/day) until infective endocarditis was ruled out via echocardiograph. After blood cultures were positive for Brucella spp., we began rifampin (600 mg/day), doxycycline (100 mg PO, q12h), and streptomycin (1 g/day) to target complicated brucellosis with infective spondylitis in accordance with WHO guidelines [3910]. While on this treatment, that patient’s CRP levels dropped to 19 mg/dL on the 16th hospital day. After the patient’s fever resolved, CRP levels decreased to 13.1 mg/dL on the 26th hospital day. After 5 months of treatment, CRP levels decreased to 1.0 mg/dL. We discontinued streptomycin on the 30th hospital day. Rifampin and doxycycline were discontinued on the 143th day since the initiation of treatment.
Analysis using 16s rRNA sequencing was used to confirm the presence of Brucella spp.. We used a forward primer of 5’-TTGGAGAGTTTGATCCTGGCTC-3’ and a reverse primer of 5’-GGCGTGGACTTCCAGGGTATCT-3’. Sequencing was commissioned by Macrogen. Blast and EzTaxon were used to analyze the sequence. According to Blast analysis, a 99.6% equivalence (720 of 723 bp) was found with several subspecies of Brucella (B. abortus, Brucella suis, B. melitensis, Brucella canis, and Brucella pinnipedialis, among others). EzTaxon analysis demonstrated a 99.86% equivalence (722 of 723 bp) with several subspecies of Brucella (B. abortus, B. canis, Brucella ceti, B. melitensis, and Brucella microti, among others). The Brucella subspecies was confirmed as B. melitensis by sequencing the omp31 gene. By PCR assay targeting the BCSP31 gene, Brucella spp. was confirmed. B. melitensis was confirmed by using PCR assay targeting the IS711 locus (Fig. 3).
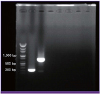 | Figure 3
BSCP31 gene targeted PCR and Brucella melitensis specific primer. The 1st lane is the ladder. The 2nd lane is BSCP31 gene targeted PCR using a specimen obtained from patient that shows a BCSP31 band at the 223 bp. The 3rd lane is PCR using a B. melitensis specific primer (IS711) with a specimen obtained from the patient that shows an IS711 band at the 731 bp.
|
Discussion
The incidence of brucellosis worldwide varies from less than 0.03 to 160 per 100,000 persons. Brucellosis has been practically eradicated in developed countries and is now mostly found in Mediterranean and Middle Eastern countries, especially Iraq, Jordan, and Saudi Arabia, as well as areas of Latin America, particularly Mexico and Argentina, the Polynesian islands of Wallis and Futuna, and the Mexico/United States border. It has lately also been found in some Central Asian countries, such as Kyrgyzstan and Azerbaijan. The spread of the disease is attributed to increasing travel between affected countries [13]. The first case of brucellosis in Korea was reported in 2002 [14]. The number of cases sharply increased between 2005-2008, with 158 cases in 2005, 215 cases in 2006, and 101 cases in 2007. As a result of improved treatment for affected persons and new vaccination programs for cows, the rate of cases declined, and there were only 7 cases of brucellosis diagnosed in 2016.
Until now, the major mode of transmission of brucellosis remains unclear. However, brucellosis of Korea seem to be transmitted through close contact with blood, fetus, urine, and placenta of domestic cow that has been infected by B. abortus, or inhalation of B. arbortus while examining or slaughtering cow [15]. This case report details the first incidence of B. melitensis imported to Korea from a patient who recently visited Iraq that resulted in brucellosis and infective spondylitis. In this international era, brucellosis in Korea is no longer limited to B. abortus. In the future, more cases of imported brucellosis are expected due to the fact that many Korean businesses are located in the Middle East, leading to increased exposure to pathogens endemic to this area.
Physicians should consider brucellosis in all patients presenting with fever and a history of recent travel to brucellosis-endemic areas.
 XML Download
XML Download