

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Optimal medical treatment after percutaneous coronary intervention (PCI) has been an important issue since the first coronary angioplasty performed by Andreas Gruentzig in 1977. Medical treatment is provided to decrease the incidence of acute and chronic complications, such as restenosis and stent thrombosis, after PCI. The superiority of dual antiplatelet therapy (DAPT) over anticoagulation was initially demonstrated in a randomized clinical trial (RCT),1) and subsequently, many studies have focused on refining DAPT strategies. The primary drug in DAPT is aspirin (an adenosine diphosphate receptor antagonist), and combinations with various P2Y12 inhibitors have been studied to reduce thrombotic complications. The initial P2Y12 inhibitor ticlopidine was replaced by clopidogrel owing to adverse effects, such as neutropenia and thrombotic thrombocytopenic purpura.2) Subsequently, there were issues regarding the optimal dosage and duration of DAPT involving aspirin and clopidogrel, and long-term DAPT (>12 months) was found to help in the secondary prevention of ischemic events.3)4) Later, more potent P2Y12 inhibitors, such as prasugrel and ticagrelor, were introduced to achieve greater platelet inhibition, decrease inter-individual variability in platelet inhibition, and reduce thrombotic complications. However, high platelet inhibition was often associated with an increased bleeding risk. Thus, there is a trade-off between decreasing ischemic risk and increasing bleeding risk. Meanwhile, there is a lower need for stronger platelet inhibition in the current PCI population when compared to that in the PCI population a decade ago. Advances in current PCI devices, including new-generation stents, have reduced the risk of stent thrombosis, and more patients with a high bleeding risk are being treated with PCI, leading to a shorter DAPT duration.
The DAPT issue is a current topic in the East Asian population owing to their unique racial characteristics that are distinct from those of Westerners. However, current guidelines are mostly based on Western trials performed in the Western population.5)6) This discrepancy has led to confusion among East Asian physicians and low adherence to the current guidelines. For example, data from the Korean Health Insurance Review and Assessment Service indicated that new-generation P2Y12 inhibitors (prasugrel and ticagrelor) were used in only 40% of the acute myocardial infarction (AMI) population, despite the fact that these agents are recommended over clopidogrel for patients with AMI in the current guidelines.7)
Therefore, in this review, we will discuss various issues regarding DAPT in East Asian patients. Specifically, we will discuss topics, including clopidogrel usage in East Asian patients, the unique characteristics of East Asian patients, new-generation antiplatelet agents in East Asian patients, and the optimal DAPT duration according to current risk scores for DAPT duration. Finally, we will discuss the need for East Asian-specific guidelines according to the results of a dedicated Asian study.
Go to : 
CLOPIDOGREL IN EAST ASIAN PATIENTS
The benefit of clopidogrel as a key drug in DAPT for acute coronary syndrome (ACS) was established by the CURE, COMMIT, and CLARITY trials.8)9)10) Clopidogrel combined with aspirin could reduce the incidence of 1-year clinical events by up to 20% when compared to the incidence with single antiplatelet therapy using aspirin. Later, DAPT involving aspirin and clopidogrel was included in the guidelines as a mandatory treatment. However, some patients still presented with ischemic outcomes after PCI. Thus, studies focused on individual heterogeneity with regard to the responsiveness to clopidogrel. Clopidogrel is a prodrug that needs to be converted into active metabolites by the hepatic cytochrome P450 (CYP) system before it irreversibly binds to the P2Y12 receptor and inhibits platelet aggregation (Figure 1).11) Therefore, genetic polymorphisms of the CYP system may affect the conversion of clopidogrel into active metabolites. Various mutations of CYP2C19, CYP3A4/5,12)
CYP1A2, and CYP2B6 are known to decrease clopidogrel activity and increase the risk of cardiovascular events.13)
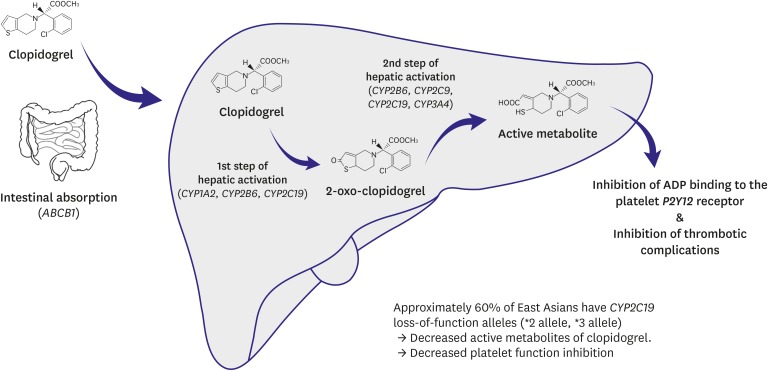
In addition, many studies have suggested that East Asians might have a distinct response to clopidogrel owing to their unique profile of CYP polymorphisms. We previously reported that the mean on-treatment platelet reactivity in 1,431 consecutive Korean patients was 241.9±70.3 P2Y12 reaction units (PRU), which is significantly higher than that in previous reports from Western countries.14) Similar findings have been reported in Japanese and Chinese patients, indicating that this may be related with racial characteristics.15)16) One of the proposed mechanisms of clopidogrel hypo-responsiveness in East Asians is associated with polymorphism of the CYP2C19 gene, which has a role in the hepatic activation of clopidogrel. Overall, approximately 60% of East Asians have CYP2C19 loss-of-function alleles (*2 allele, *3 allele), while only 30% of Caucasians have these alleles.17) In various previous clinical studies, including our study, the cut-off value for ‘high on-treatment platelet reactivity’ was greater in East Asian patients than in Caucasian patients.18)19)20)
Various attempts have been made to overcome clopidogrel hypo-responsiveness. High-dose clopidogrel (150 mg/day) was evaluated in the OPTIMUS study for high-risk patients with type 2 diabetes mellitus21) and in the CURRENT-OASIS RCT for ACS patients. In the CILON-T study, triple antiplatelet therapy (aspirin, clopidogrel, and cilostazol) was compared with DAPT.18) These studies showed greater reduction in platelet reactivity with additional therapy. There was an association between greater platelet inhibition and less ischemic events; however, the reduction in ischemic events by the intensified regimens did not reach statistical significance probably because of the insufficient number of patients. In the HOST-ASSURE RCT, 2 different intensified antiplatelet regimens for 1 month were compared (double-dose clopidogrel with aspirin versus triple agents [DAPT and cilostazol]).22) The PRU value was lower and the incidence of ischemic events tended to be lower for triple agents than for double-dose clopidogrel on top of aspirin. Both regimens were comparable and very effective for reducing target lesion failure rate to less than 3% at 1 year with a contemporary drug-eluting stent (DES). Thus, such intensified regimens for 1 month may be beneficial in patients undergoing PCI, who have high risks of thrombosis and bleeding.
Many studies have been performed to examine whether platelet function monitoring and genetic testing might be able to identify patients with a high risk of ischemic outcomes, which may allow appropriate modification of DAPT. However, unexpectedly, all randomized trials failed to demonstrate any benefit of platelet function monitoring.23)24)25)26) Therefore, currently, platelet function testing and genetic testing are not recommended for tailoring DAPT according to patient characteristics.5)
Go to :
UNIQUE CHARACTERISTICS OF EAST ASIANS AND THE ASIAN PARADOX
According to the abovementioned studies, the frequency of clopidogrel hypo-responsiveness is known to be greater in East Asian patients than in Caucasian patients. Many trials have shown that clopidogrel hypo-responsiveness is a strong and independent risk factor for post-PCI thrombotic complications.12)19)27)28) However, East Asian patients are known to have less thrombotic events and more bleeding events when compared to the findings in Caucasian patients. This concept was termed the “Asian Paradox,” which led to the suggestion of different thresholds of platelet reactivity between East Asian and Caucasian patients.17) The Asian paradox is not the first concept to suggest a racial difference in the ischemic/bleeding threshold between East Asian and Caucasian patients. Shen et al.29) reported that Asian patients with atrial fibrillation were at greater risk for warfarin-related intracranial hemorrhage, and Mak et al.30) reported that the Asian ethnicity was an independent predictor of moderate bleeding complications in the CHARISMA trial. Moreover, a patient-level meta-analysis of seven RCTs suggested that prolonged DAPT was a significant predictor of bleeding complications in only the East Asian population (Figure 2).31)
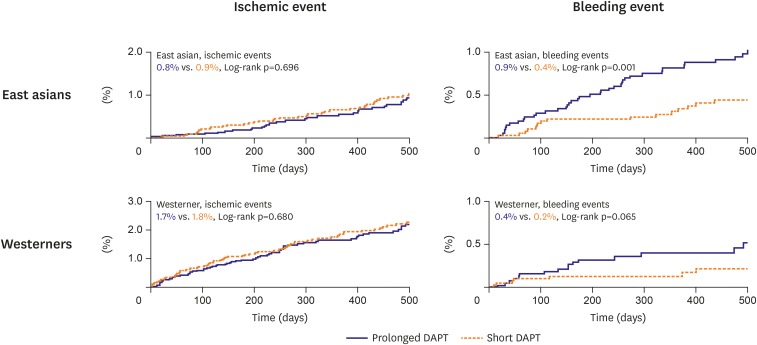 | Figure 2Ischemic and bleeding events according to prolonged versus short DAPT in East Asians and Westerners. Absolute frequency of ischemic events was half in Asians than Caucasians, while incidence of bleeding was 2-times in Asians than Caucasians. Prolonged DAPT failed to reduce ischemic events in both Asians and Caucasians, while increased bleeding events, remarkably in East Asian patients. This figure was modified from the original version.31)DAPT = dual antiplatelet therapy.
|
There are some plausible explanations for these findings. First, the unique demographics, comorbidities, and disease patterns of East Asian patients can potentially influence the different responses to antiplatelet agents.32) Particularly, East Asians have a low body mass index, and it has been shown that a high body mass index is associated with a hypercoagulable state.33) Second, genetic polymorphisms of thrombosis-related factors (i.e., factor V Leiden [G1691A] and prothrombin G20210A gene), different levels of hemostatic factors (i.e., fibrinogen, D-dimer, and factor VIII), and differences in plasma endothelial activation markers (i.e., von Willebrand factors, ICAM-1, and E-selectin) might contribute to the racial differences in thrombogenicity.17) According to these findings, in a consensus statement paper from the World Heart Federation, Levine et al.34) stated that the risk profiles for both ischemia and bleeding differ between East Asian patients and Caucasian patients and that a different “therapeutic window” of on-treatment platelet reactivity might be appropriate for East Asian patients.
Go to :
NEW-GENERATION ANTIPLATELET AGENTS IN EAST ASIAN PATIENTS
To overcome the limitations of clopidogrel, 2 new-generation P2Y12 inhibitors (prasugrel and ticagrelor) have been introduced. The TRITON-TIMI 38 study was a landmark trial comparing prasugrel to clopidogrel in ACS patients undergoing PCI.35) This study showed that prasugrel decreased the incidence of adverse cardiovascular events (primary endpoint: hazard ratio [HR], 0.81; 95% confidence interval [CI], 0.73–0.90), but increased the incidence of bleeding events, especially in elderly patients, patients with a low body weight, and those with a history of stroke. Subsequent sub-studies confirmed the mortality benefit of prasugrel in various populations,36)37) and some nationwide studies revealed the favorable effects of prasugrel on mortality.38) The other P2Y12 inhibitor ticagrelor significantly reduced the incidence of the primary ischemic endpoint (HR, 0.84; 95% CI, 0.77–0.92) with no increase in major bleeding events in the PLATO study.39) The beneficial effects of ticagrelor on mortality have been consistently confirmed in sub-studies40)41)42) and in registry-based studies.43) Based on the findings of these studies, prasugrel and ticagrelor were included in the current guidelines and were recommended for patients with ACS.5) However, it should be noted that the effects of these new-generation P2Y12 inhibitors have not been clearly clarified in East Asian patients. Kang et al.44) analyzed the East Asian subset of the PLATO trial and showed consistent beneficial effects of ticagrelor in East Asian patients. However, only 551 East Asian patients were analyzed, and the results showed a similar trend for the East Asian population and the Western population, without statistical significance. Additionally, Goto et al.45) performed an RCT on ticagrelor in Japanese ACS patients and found that ticagrelor did not reduce the incidence of ischemic outcomes and increased the bleeding risk. We previously performed a retrospective analysis of a nationwide cohort of Korean AMI patients and found that the new P2Y12 inhibitors were associated with a significantly higher bleeding risk (aspirin plus prasugrel vs. aspirin plus clopidogrel: HR, 2.14; 95% CI, 1.53–2.99; p<0.001; aspirin plus ticagrelor vs. aspirin plus clopidogrel: HR, 2.26; 95% CI, 1.73–2.95; p<0.001), with no decrease in the incidence of thrombotic events (Figure 3).32) Saito et al.46) confirmed the efficacy and safety of prasugrel in Japanese ACS patients, but the authors used a lower dose than that mentioned in the current guidelines (20 mg loading dose and 3.75 mg maintenance dose). Additionally, a recent study based on the Health Insurance Review and Assessment Service Korean database showed that the new-generation P2Y12 inhibitors had favorable effects on 30-day mortality in AMI patients undergoing PCI.7) However, this was a limited study owing to the lack of information in the nationwide database (data on the predictors of acute complications, such as clinical presentation, left ventricular function, angiographic disease extent, and medication, were not available). Collectively, previous studies failed to provide concrete evidence for the beneficial effects of the new-generation P2Y12 inhibitors in East Asian patients. Before the current guidelines are adopted, we should consider the unique features of East Asian patients in terms of the ischemic/bleeding threshold.
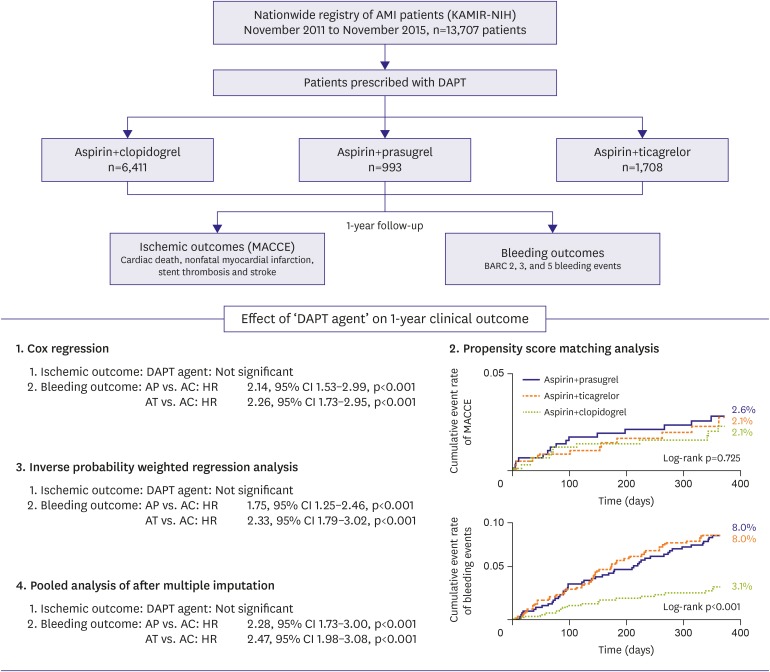 | Figure 3Results from a retrospective analysis of a nationwide cohort of Korean AMI patients. During a 1-year follow-up period after index PCI, ischemic outcomes and bleeding outcomes were analyzed. Compared with clopidogrel (AC), new generation P2Y12 receptor inhibitors prasugrel (AP) and ticagrelor (AT) could not decrease ischemic outcomes, while significantly increased bleeding outcomes. Consistent results were shown in multivariate cox regression analysis, propensity score matching analysis, inverse probability weighted regression analysis, and pooled analysis after multiple imputation. This figure was modified from the original version.32)AMI = acute myocardial infarction; CI = confidence interval; DAPT = dual antiplatelet therapy; HR = hazard ratio; MACCE = major adverse cardiac and cerebral events; PCI = percutaneous coronary intervention.
|
Go to :
PREVIOUS CLINICAL STUDIES ON OPTIMAL DAPT DURATION
Although DAPT is essential after PCI, the optimal DAPT duration has not been established. In the DES era, 14 large-scale RCTs have compared the efficacy and safety of long-term and short-term DAPT (Table 1). Among these studies, 6 RCTs compared long-term DAPT (24–48 months) to short-term DAPT (6–12 months) in order to determine the efficacy and safety of extended therapy.47)48)49)50)51)52) These studies reported that long-term DAPT reduced late and very late stent thromboses and prevented ischemic events in other non-stented sites. The Dual Antiplatelet Therapy study was the largest trial in which patients without ischemic or bleeding events during the initial 12 months after PCI were randomized to receive additional DAPT for 18 months or to receive aspirin monotherapy.50) Extended DAPT resulted in a 1.0% absolute reduction in stent thrombosis, a 1.6% absolute reduction in major adverse cardiac events, and a 0.9% absolute increase in moderate or severe bleeding events.
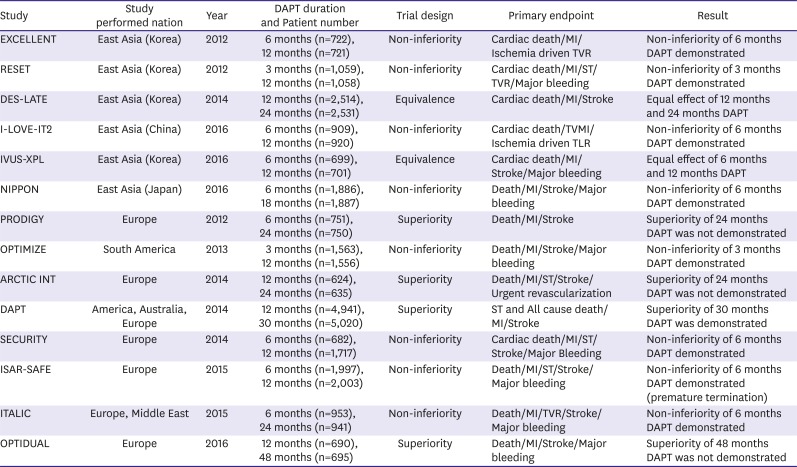
Table 1
Current large-scale RCTs comparing the efficacy and safety of long-term and short-term DAPT
DAPT = dual antiplatelet therapy; MI = myocardial infarction; RCT = randomized clinical trial; ST = stent thrombosis; TLR = target lesion revascularization; TVMI = target vessel myocardial infarction; TVR = target vessel revascularization.
![]()
On the other hand, eight RCTs compared short-term DAPT (3–6 months) to long-term DAPT (12–18 months) in order to determine the efficacy and safety of reduced-duration DAPT.53)54)55)56)57)58)59)60) These studies were mostly designed as non-inferiority trials, and they confirmed the safety of short-term DAPT. The EXCELLENT trial was the first RCT to compare short-term and long-term DAPT, and it showed that 6-month DAPT did not increase the risk of target vessel failure at 12 months after DES implantation when compared to the finding with 12-month DAPT.53)
Interestingly, a weighted risk-benefit analysis and systemic review of previous RCTs performed by the Evidence Review Committee reported that prolonged DAPT decreased the incidences of myocardial infarction by 6 per 1,000 patients and stent thrombosis by 3 per 1,000 patients, but increased the incidence of major bleeding events by 5 per 1,000 patients. With regard to reduced-duration DAPT, there were no increased risks of stent thrombosis and fewer bleeding complications.61)
Among these RCTs, a difference in design can be noted, reflecting the different needs of short DAPT between Eastern and Western populations. Five out of 6 RCTs in East Asian countries compared short-term DAPT (3–6 months) to long-term DAPT (12–18 months). However, in Western countries, 3 (OPTIMIZE, SECURITY, and ISAR-SAFE) out of 8 RCTs evaluated the safety of short-term DAPT (3–6 months) (Table 1). Collectively, we can assume that there is a greater need for short-term DAPT (less than 12 months) in East Asian patients than in Western patients.
Go to :
WESTERN RISK SCORES TO DETERMINE DAPT DURATION
The recent trend of DAPT is based on the concept of “one size does not fit all.”62) Until now, three scoring systems have been used to assess the ischemic/bleeding risk in the PCI population (the PARIS score, PRECISE-DAPT score, and DAPT score), and the current guidelines recommend using 2 specific scores to assess the appropriate DAPT duration (the PRECISE-DAPT and DAPT scores).6)63) However, these scores have limitations that should be considered. First, the PRECISE-DAPT score only evaluates bleeding risk to determine DAPT duration. However, as a high bleeding risk does not warrant a low ischemic risk, both the bleeding and ischemic risks should be considered when deciding the optimal DAPT duration. Second, the DAPT score was developed in a DAPT study, which involved a population free from clinical events within the first 12 months after PCI.50) Therefore, this score should be used to decide whether an individual should continue DAPT beyond 1 year after PCI. Furthermore, this scoring system was derived from the findings of a RCT that included vein graft PCI and paclitaxel-eluting stents, which are not applicable in the new-generation DES era. Moreover, both scoring systems were mainly developed in Western patients, who showed an ischemic/bleeding threshold different from that in real-world East Asian patients. Table 2 presents a brief overview of the current scores.
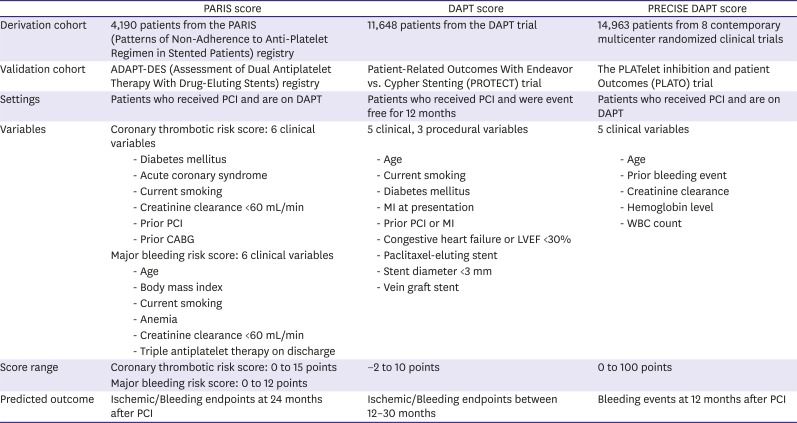
Table 2
Currently used scoring systems in deciding the optimal DAPT duration
CABG = coronary artery bypass grafting; DAPT = dual antiplatelet therapy; LVEF = left ventricular ejection fraction; MI = myocardial infarction; PCI = percutaneous coronary intervention; WBC = white blood cell.
![]()
Based on these findings, we propose the need for an East Asian-specific scoring system that fulfills the following requirements. First, the system should consider the unique characteristics of East Asian patients. The bleeding risk is higher and ischemic risk is lower in East Asian patients than in Western patients,17)34) and these differences should be reflected in the scoring system. Second, the system should be applicable to real-world East Asian PCI populations using new-generation DESs. New-generation DESs have been shown to be safer than previous-generation DESs or even BMSs with regard to restenosis and thrombotic complications,64) and therefore, the DAPT duration may be shortened. Third, both ischemic and bleeding risks should be considered to evaluate the overall ischemic/bleeding risk of an individual. A high bleeding risk does not necessarily indicate a short DAPT duration, as a high bleeding risk frequently overlaps with a high thrombotic risk. The benefit of DAPT after evaluating the possibility of ischemic and bleeding events should be considered. Moreover, the scoring system should assess the optimal DAPT duration immediately after PCI.
Go to :
CONCEPT OF HIGH BLEEDING RISK AND ULTRA-SHORT DAPT
After the inclusion of DAPT with aspirin plus clopidogrel in the guidelines as a mandatory treatment, 2 groups with regard to DAPT duration have emerged. The first group places emphasis on the prevention of stent thrombosis and progressive atherothrombosis with long-term DAPT, while the second group places emphasis on the reduction in the risk of bleeding events with short-term DAPT. This debate on DAPT duration has led to the concept of personalized medicine, where the risks of ischemia and bleeding in a particular individual are considered when deciding the optimal DAPT duration. However, the current general trend is moving toward shortening the mandatory DAPT duration. Particularly, after the LEADERS FREE trial confirmed the safety and efficacy of ultra-short DAPT (1 month) in patients with high bleeding risk,65) many trials are being conducted to confirm the safety of short-term DAPT in high bleeding risk subsets. These trials are in line with improvements in PCI devices and techniques, which have reduced the thrombotic risk associated with devices implanted in the coronary artery. Trials, such as the MASTER DAPT trial (Trial registry at ClinicalTrials.gov: NCT03023020), EVOLVE Short trial (NCT02605447), XIENCE Short trial (NCT03218787), Onyx ONE trial (NCT03344653), and COBRA-REDUCE trial (NCT02594501) will soon provide information on the efficacy and safety of 1-month DAPT in the contemporary DES era. The criteria for high bleeding risk in each on-going trial are shown in Table 3.
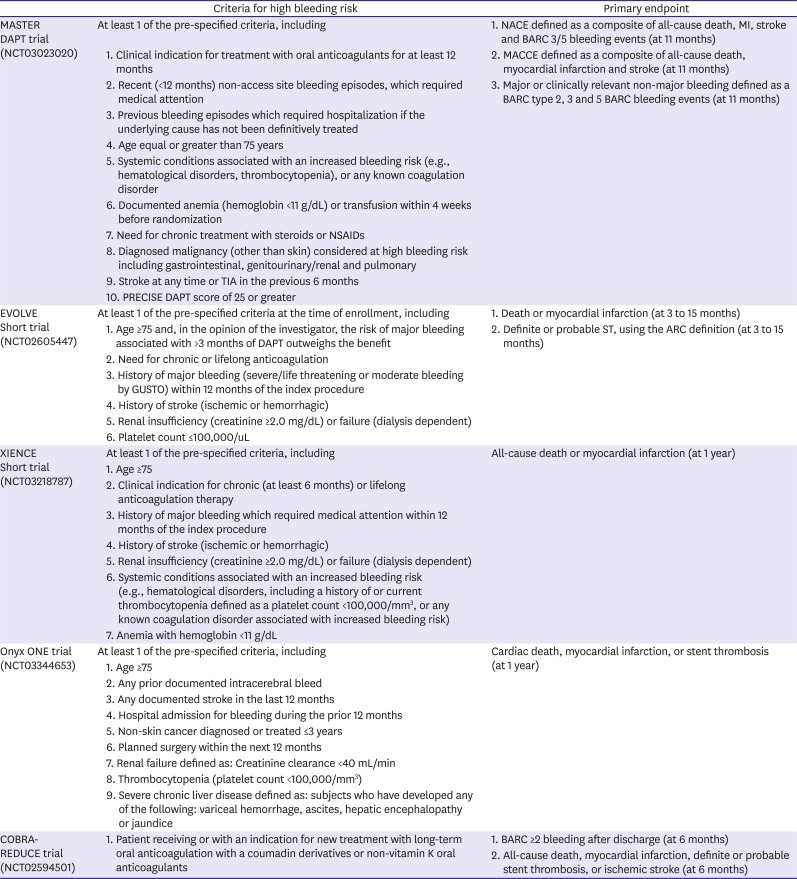
Table 3
The criteria for ‘high-bleeding risk’ of each on-going trial
ARC = Academic Research Consortium; DAPT = dual antiplatelet therapy; MACCE = major adverse cardiac and cerebral events; NACE = net adverse clinical endpoints; NSAIDs = nonsteroidal anti-inflammatory drugs; PCI = percutaneous coronary intervention; ST = stent thrombosis; TIA = transient ischemic attack.
![]()
Go to :
USE OF DAPT IN EAST ASIAN PATIENTS AND THE NEED FOR AN ASIAN DAPT SCORE
Ethnicity is an important factor that should be considered when determining the optimal DAPT duration. As mentioned above, East Asian patients have a unique ischemic and bleeding risk profile, which has been conformed in various studies involving ex-vivo and real-world data. However, the racial effect on the benefit of DAPT has not been well considered by current studies and current guidelines derived from various studies. Thus, physicians in East Asia are reluctant to apply the Western guidelines for antiplatelet agent use after PCI in clinical practice. For example, the new-generation P2Y12 inhibitors are prescribed within 1 year after PCI in less than 50% of all ACS patients, although a decade has passed since landmark studies, such as the TRITON-TIMI 38 and PLATO trials, demonstrated their benefits.35)39) A guideline specifically for East Asian patients and a unique regimen for these patients might help in the fine-tuning of DAPT for this population. We are designing an East Asian-specific scoring system, which is being tentatively named the “A-DAPT (Asian dual antiplatelet agent) score.” This score will reflect the unique ischemic/bleeding risk of East Asian patients and will be directly applicable to real-world East Asian PCI populations using new-generation DESs. The validation results of the A-DAPT score will soon be reported.
Go to :
 XML Download
XML Download