

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Axillary nerve (C5, C6) arises from the posterior cord of brachial plexus [1]. It runs underneath the deltoid muscle and its anterior branch is at particular risk of iatrogenic injury [2]. Axillary nerve is the most commonly injured nerve during several orthopedic surgeries, especially during deltoid splitting approach for surgical repair of rotator cuff and for fixation of proximal humerus fractures [3]. Injury to axillary nerve may result in motor paralysis and atrophy of the deltoid muscle leading to weak abduction and forward flexion [4]. Several authors have investigated the anatomical course of the nerve and reported that axillary nerve is located about 5 cm from the tip of the acromion and thus splitting of deltoid fibres more than 4 cm from this tip is not recommended [35]. However, several anatomical studies have shown a wide range of the “safe area” for axillary nerve ranging from 3 to 7 cm from the acromion [6789].
The aim of the present study was to investigate the distance of the axillary nerve from the acromion and its relation with upper arm length and also to re-define the “safe area” for the axillary nerve during surgical splitting of deltoid muscle.
Go to : 
Materials and Methods
The study was conducted on sixty shoulders of thirty embalmed cadavers (26 males and four females) with age range from 40 to 65 years. Shoulders with signs of previous surgery or any other deformity were excluded. Keeping the arm in neutral position (by the side of the body), an incision was given along the delto-pectoral groove. Degree of rotation of shoulders could not be assessed as most of the cadavers were too stiff. Skin and fascia over the shoulder region were removed to expose the deltoid muscle. The muscle was separated/released from the clavicle, acromion and spine of scapula as close to its origin as possible and reflected downwards and backwards. Sub deltoid fascia over the inner surface of deltoid was removed to expose the nerve (Fig. 1). Care was taken so as not to damage the nerve deep in the muscle. The entire course of the nerve along with its anterior branch was noted. In order to represent the axillary nerve on the outer surface of the deltoid, needles were pierced through the deltoid into the axillary nerve and then whole flap of the muscle was sutured back to its original anatomical position [10]. The line joining these needles represented the course of the nerve on the outer surface of deltoid (Fig. 2). The distances from the anterior and posterior edge of acromion to the course of the axillary nerve were measured with the help of digital vernier calipers (with least count of 0.01 mm) and recorded as anterior and posterior acromio-axillary (AA) distances respectively. To estimate the correlation between the AA distance and arm length, upper arm length was measured from the superior border of the lateral edge of the acromion to the tip of the lateral epicondyle of the humerus. The ratios between anterior and posterior AA distance and upper arm length were calculated and recorded as anterior index and posterior index, respectively.
 | Fig. 1The inner surface of deltoid muscle showing the main trunk of axillary nerve with its anterior branch after removal of sub deltoid fascia over it.
|
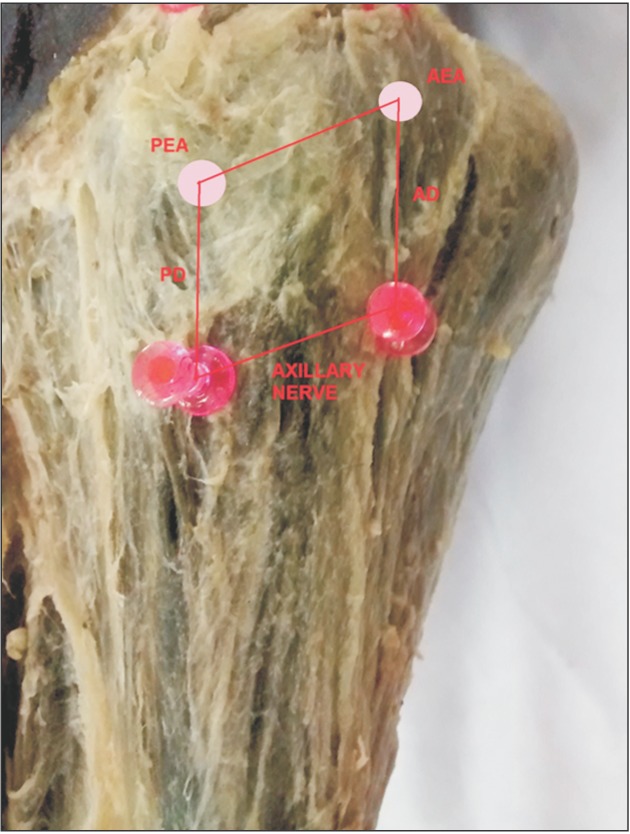 | Fig. 2The deltoid muscle was replaced in its original anatomical position. The course of axillary nerve is shown with the help of needles, and the anterior acromio-axillary distance (AD) and posterior acromioaxillary distance (PD) were measured. AEA, anterior edge of acromion; PEA, posterior edge of acromion.
|
Statistical analysis
Correlation analysis was performed between upper arm length and anterior and posterior AA distances with the use of SPSS 16.0 software version for windows (SPSS Inc., Chicago, IL, USA). The anterior index and posterior index were analyzed with the use of descriptive method with SPSS 16.0 software version for windows.
Go to :
Results
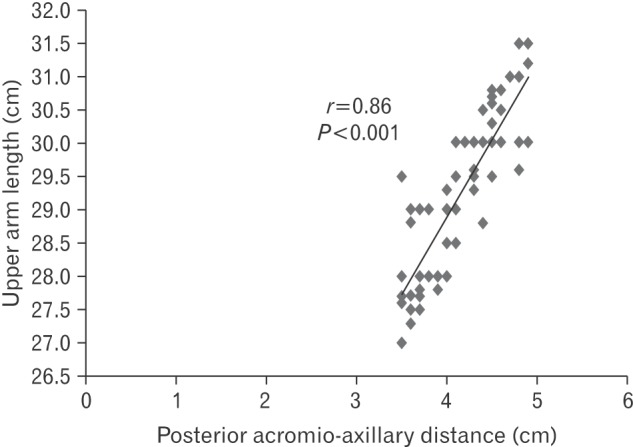
In our study, the mean value of upper arm length was 29.30±1.61 cm. The mean of anterior AA distance was 5.22±0.60 cm, and the mean of posterior AA distance was 4.17±0.45 cm (Table 1). There was a significant correlation between the upper arm length and anterior AA distance (r=0.89, P<0.001) (Fig. 3). Significant correlation was also found between upper arm length and posterior AA distance (r=0.86, P<0.001) (Fig. 4). The mean of anterior index was 0.18±0.02 (range, 0.15–0.21) and the mean of posterior index was 0.14±0.01 (range, 0.12–0.16). The ideal safe area for the axillary nerve was found to be a quadrangular area above it and the size of which would depend on individual's upper arm length.
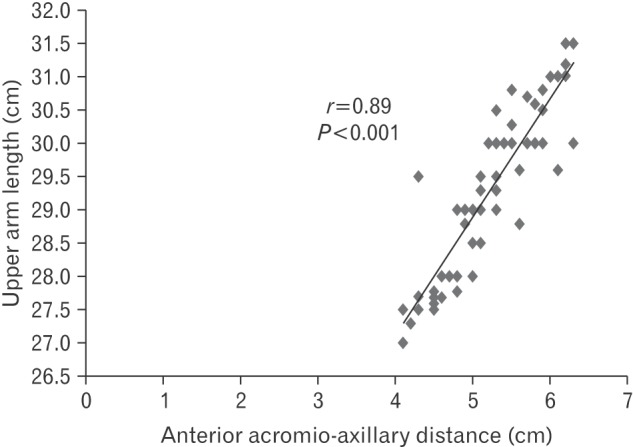 | Fig. 3Graph illustrating the correlation between upper arm length and anterior acromio-axillary distance.
|

Go to :
Discussion
The avoidance of iatrogenic injury to the axillary nerve during surgical intervention (open surgery or arthroscopic) of the shoulder region is a matter of concern for orthopedic surgeons. Deltoid-splitting incisions are widely used for open rotator cuff repair, intramedullary nailing of humeral fractures, and shoulder arthroscopy [111213]. Many researchers have studied the anatomy of axillary nerve and made an effort to define a so called safe area rather a safe distance for deltoid splitting incision. However, the safe area varies widely according to different authors. Most of the authors have deduced the average distance of the axillary nerve from different landmarks of acromion process and thus derived the maximum permissible length of deltoid split or safe deltoid split.
Abbott and Saunders [6] stated that incisions made with separation of the fibers of the deltoid should not extend downward for more than 3.81 cm below the margin of the acromion.
Burkhead et al. [14] studied the axillary nerve in 51 embalmed and five fresh cadaveric specimens. They found that in nearly one fifth of the cadavers, the nerve at some point in its course around the humerus in the deltoid muscle was less than 5.00 cm from the palpable edge of the acromion and at a minimal distance of 3.10 cm. The difference in the material used in this study (fresh cadavers) or differences in population characteristics may be responsible for the greater percentage they noticed. Duparc et al. [7] reported that the mean distance between the axillary nerve and the insertion of the deltoid muscle on the acromion was 3.40 cm. However, Hoppenfeld and deBoer [8] found this distance to be 7.00 cm. Uz et al. [15] studied 30 shoulder specimens and recorded that the mean distance from the postero-lateral aspect of the acromion process to the axillary nerve and its branches was 7.80 cm. Ikemoto et al. [16] studied 24 shoulders and found that the average distance between the acromion and the axillary nerve on the antero-superior approach was 5.32±0.60 cm in both shoulders. Gurushantappa and Kuppasad [17] dissected forty shoulders and found that the mean distance of axillary nerve from postero-lateral aspect of acromion process was 7.46±0.99 cm. Abhinav et al. [4] dissected 30 cadaveric shoulders and found the average AA distance to be 6.00 cm in neutral position.
Reviewing previous literature leaves us with much uncertainty as safe distance varies widely according to different authors. This can be due to the differences in individual diagnostic criteria, measuring techniques, observer error, and confounding factors of the population or ethnic group under study. Most of the authors mentioned above, have measured the AA distance as a vertical length between the lateral edge of the tip of acromion process and a fixed point over the course of the axillary nerve and thus derived the average AA distance. Using this average AA distance as the maximum permissible length of safe deltoid split may still result in some amount of nerve damage as the nerve is not constantly parallel to the lateral edge of the acromion [2] and position of the nerve varies at different points along its course.
In the present study, anterior AA distance was 5.22 cm (range, 4.10–6.30 cm) whereas posterior AA distance was 4.17 cm (range, 3.50–4.90 cm). As the course of the nerve varies at different points along its course, so in an anterior approach, length of the safe deltoid split should be 4.10 cm (shortest anterior AA distance) and in posterior approach, it should be 3.50 cm (shortest posterior AA distance). The main problem of the anterior approach to the shoulder is the risk of anterior deltoid palsy and atrophy as the nerve to this head has a frequent ascending course. By taking the shortest AA distance as the length of safe deltoid split, we can minimize the risk of axillary nerve damage as well as risk of anterior deltoid palsy and atrophy.
Rockwood and Wirth [18] recommended that, when a posterior deltoid-splitting incision is used, the deltoid can be split safely along the line of its fibres downward for a distance of 10.16 cm (approx). Though there is a paucity of literature regarding the prevalence of axillary nerve injury after such a posterior approach to the shoulder, on the basis of the results of present study we can conclude that the use of this approach can be unsafe and the maximum permissible length for posterior deltoid split should be 3.50 cm only.
In our study, we found that upper arm length (distance from the superior border of the lateral edge of the acromion to the tip of the lateral epicondyle of the humerus) was strongly correlated with both the anterior and posterior AA distance, which is absolutely in accordance with the findings of Cetik et al. [10] and Abhinav et al. [4] who found that determination of the length of safe deltoid split not only depends upon the upper arm length but also on the position of the upper limb during surgery and deltoid should not be split in abduction. We have taken all the measurements by keeping the arm in neutral position as this is the most commonly used position for shoulder surgery using anterior or anterolateral approach.
Contrary to the studies mentioned above, few researchers have studied the anatomy of axillary nerve taking dimensions of the deltoid into account.
In a cadaveric study, Kulkarni et al. [19] showed that the axillary nerve is 2.20–2.60 cm above the midpoint of the vertical plane of the muscle. In an another study, Nassar et al. [9] derived axillary nerve index (ratio between the distance of the nerve from the acromio-clavicular joint and the length of the deltoid from the anterior clavicular line) and proposed such index as a useful guide for estimation of the position of the nerve during surgery.
Kontakis et al. [20] who measured the axillary nerve position in relation to deltoid width and length, concluded that the deltoid ratio (width:height) was useful for estimating the location of the nerve. However, measuring internal width and length of deltoid intra operatively is not only difficult but also practically awkward for orthopedic surgeons. It has also been demonstrated that the safe area for a nerve may vary in size according to the length of the limb [21], the shorter the deltoid length, the greater the danger of damaging the nerve at a short distance from the upper border of the muscle [20]. The present study demonstrates that arm length, which is easy to measure, can be used to predict the course of the axillary nerve.
Most of the literature describing the anatomy of axillary nerve have made an effort to define the so called safe area for the axillary nerve during shoulder surgery but ended up defining a vertical line extending from the lateral edge of acromion to the course of the nerve lying circumferentially over the humeral shaft. In our study we have found that the AA distance was not constant at every point along the course of the nerve. The acromion which forms the summit of the shoulder is a large, somewhat triangular or oblong process. So we have considered acromion as a palpable line rather than a single point and have measured the AA distance both from its anterior as well as posterior edges. Most interesting fact is that we didn't find a single limb where these two distances match.
We believe that a “safe area” for surgical splitting of deltoid can be redefined as an area above the course of axillary nerve instead of a safe line. We proposed the “safe area” to be quadrangular in shape, the size of which would depend on the length of the upper arm. This confirms the findings of Cetik et al. [10] who described this safe area as quadrangular in shape, the length of its lateral edges being dependent on arm length. Using the above described safe area for shoulder surgery would preserve axillary nerve and all its branches and provide a safe exposure for the patient during shoulder operations.
In conclusion, we confirm that the distance from the acromion to the axillary nerve is widely variable. As the course of the axillary nerve varies at different point so it is always advised to take the shortest distance as safe deltoid split, by this way we can minimize the risk of nerve injury as well as of anterior deltoid palsy and atrophy. Upper arm length has a strong correlation with both anterior and posterior AA distances. We propose the “safe area” to be quadrangular in shape, the size of which would depend on individual's arm length rather upper arm length.
Go to :
 XML Download
XML Download