

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The human thumb is unique as it represents the most intricate and complex mechanism to carry out many functions ranging from fine skilled movements to forceful grasps. Normal flexion of the thumb requires the integrity and harmonized action of a number of fine structures that are centered around the flexor tendon [1]. The most important is the retinacular pulley system around the flexor pollicis longus (FPL) tendon. These pulleys are the focal thickened area of the flexor tendon sheaths. It allows the tendon to glide inside it smoothly and also maintain apposition of tendon and bone across the joint. So that it acts as an efficient fulcrum for flexion and extension of thumb without bowstringing of the tendon [2]. There is a controversy in the literature about the number and morphology of pulleys of thumb. Doyle and Blythe [3] studied the pulley system of the thumb and reported that it has three pulleys: two annular pulleys namely A1 and A2 and one oblique pulley between this. Schmidt and Fischer [4] described two annular pulleys A1, A2, and Y shaped fibre complex between this having proximal annular and distal oblique part. Bayat et al. [2] could identify a distinct variable pulley (Av) between A1 and oblique pulley in 90% cases. They were previously considered as an annular part of Y shaped fiber complex by Schmidt and Fischer [4]. Thus according to them, the pulley system of thumb consists of four components namely A1, Av, oblique, and A2 and opposed to the traditional view of only three [24]. Schubert et al. [5] did extensive cadaveric study and could find distinct Av pulley in 93% of hand specimen. Based on this they classified morphological pattern of pulley system into four types [5]. Magnetic resonance imaging study by Hirschmann et al. [6] could identify all pulleys (A1, Av, oblique, and A2) in 100% of asymptomatic cases they studied. Damage to the pulley system whether, partial or complete could affect performance of the digit [2]. It can occur during surgical release of pulley while treating trigger thumb or when excessive stress is imposed on these structures in activities such as rock climbing [1]. Trigger thumb is corrected most commonly by surgical release of the A1 pulley when medical management fails. Even though, the surgical release of the pulley in treating trigger thumb is a simple procedure, the success rate depends on the anatomical knowledge of pulley of the thumb [7]. It is also important for reconstruction of the damaged pulley system [8]. To our knowledge of morphology and morphometry study of pulley system of the thumb has not been described in detail in Indian literature and hence this study was conducted with the aim to document its morphology and morphometry in Indian population.
Go to : 
Materials and Methods
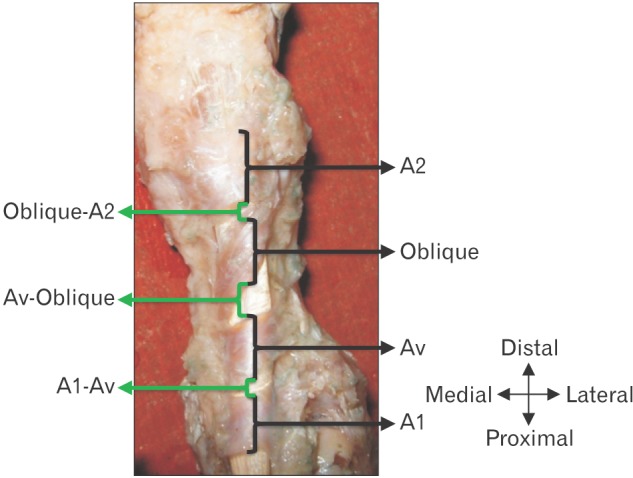
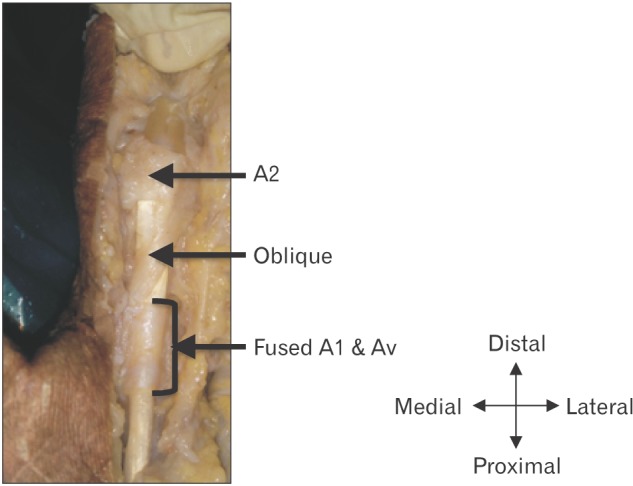
The present study was performed in fresh adult human cadavers that have been donated to the Department of Anatomy, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry through the institutional body donation program following the ethical guidelines. The protocol for this research project was approved by the Institute Ethic committee, JIPMER. Cadavers with any evidence of damage or loss of tissues in the region of thumb were excluded from this study. Dissection was carried out in 28 cadavers, out of which 18 were male and 10 were female cadavers. In one female cadaver right side thumb was amputated previously and was not included in the study. Thus total 55 cadaveric thumbs were included in this study. The cadaver number, age, gender and side of the hand were noted and the following dissection steps were followed. Thumb was kept in extended position. Length of the thumb was measured from the proximal thumb crease to the tip of the thumb. A longitudinal skin incision was made in the palmar aspect of the thumb from its base to the tip. The superficial fascia, the digital nerves, and arteries were retracted to expose the flexor sheath around the FPL tendon. The proximal and the distal edges of each pulley were identified and the flexor sheath between the pulleys was dissected and removed. The morphology of each pulley in thumb was noted and classified into four types according to Schubert et al. [5]. Other variation in its morphology was also noted. The width of the pulley such as A1, Av, oblique, and A2 was measured. The gap distance between the pulleys such as A1-Av, Av-oblique, and oblique-A2 was also measured (Fig. 1). Gap distances between other pulleys were calculated as follows.
The dissection was carried out with micro dissection instruments with the help of magnifying lens and the operating stereo microscope. All these measurements were taken along the longitudinal axis of the thumb using Mitutoyo digital vernier caliper (Kawasaki, Japan) to the nearest millimeters. The measurements were recorded thrice and the mean of measurements was taken as final. Morphological types of the pulleys were expressed in proportion. Width and gap distance between the pulleys were expressed in mean, standard deviation. Mean difference between the left and right side and between the genders was analyzed using paired t test and the P-value less than 0.05 was considered statistically significant at 5% alpha error with 95% confidence interval. Linear regression graph was plotted to look for relationship between length of the thumb with gap distances and width of the pulleys.
Go to :
Results
All paired cadaveric thumbs showed the symmetrical morphological pattern of pulley system (26 pairs) except one pair which showed an asymmetrical pattern in left and right thumb. The pulley system of thumb thus consisted of four pulleys: A1, oblique, A2, and Av pulley placed between A1 and oblique. Pulley system of thumb has been classified into four types based on presence or absence of Av pulley and the orientation of the fibers of Av pulley [5].
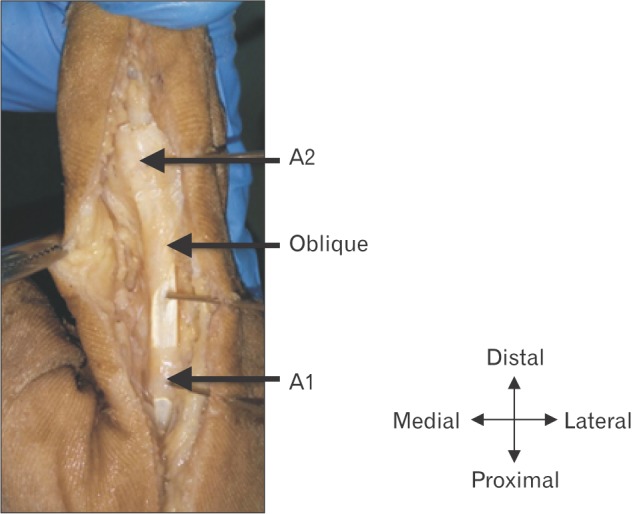
- Type I: Av pulley was absent. Other pulleys namely A1, oblique and A2 were present (n=4, 7.27%) (Fig. 2).
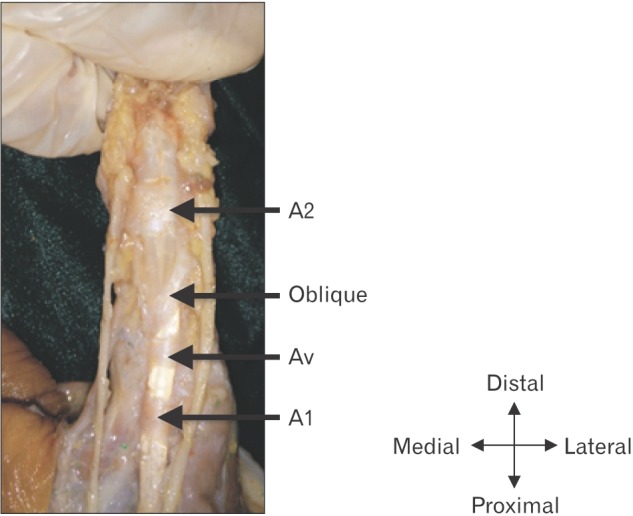
- Type II: Av pulley was present in addition to other three pulleys. The direction of Av was transverse to the long axis of FPL tendon. All pulleys were separate from each other (n=10, 18.18%) (Fig. 3).
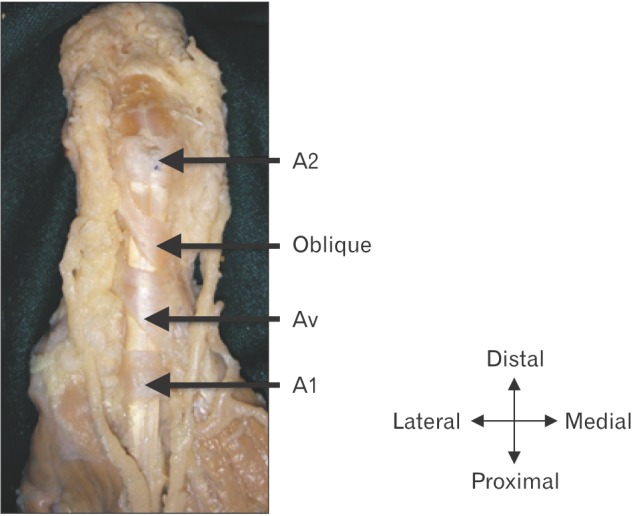
- Type III: Similar to type II. But the direction of fibers Av pulley was oblique running from ulnar to radial side proximo—distally to the long axis of FPL tendon (n=30, 54.55%) (Fig. 4).
- Type IV: All pulleys were present. The Av pulley fibre was transverse and was fused with A1. No gap was present between A1 and Av pulley (n=10, 18.18%) (Fig. 5).
In the asymmetrical pair, the right thumb revealed the presence of A1, Av, and A2 pulleys but the oblique pulley was absent (n=1, 1.82%). Whereas in the left thumb type III pattern was observed. The Av pulley fiber in type III was either triangular (proximal border oblique and distal border horizontal) or entirely oblique (both proximal and distal border oblique in direction). The fibers of Av pulley present in type II, III, and IV arose from the adductor pollicis.
Overall width of the A1, Av, oblique, and A2 pulley is represented as dot distribution graph (Fig. 6). Width of the pulleys according to its morphological types is tabulated as Table 1. In type IV, the fibres of A1 and Av pulleys were fused together so the mean and standard deviation of width from the proximal edge of A1 to distal edge of Av was measured and found to be 10.91±2.38 mm. The mean and standard deviation of gap distances between each pulley of the thumb according to different morphological types of pulleys are summarized (Table 2). The paired t test showed no significant difference in mean width and gap distances between the right and left hand except gap distance between oblique and A2 pulley (Table 3). Gender did not influence much on the width and the gap distances of the pulleys (Table 4). Linear relationship existed only between width of the Av pulley and length of the thumb (Fig. 7, 8).
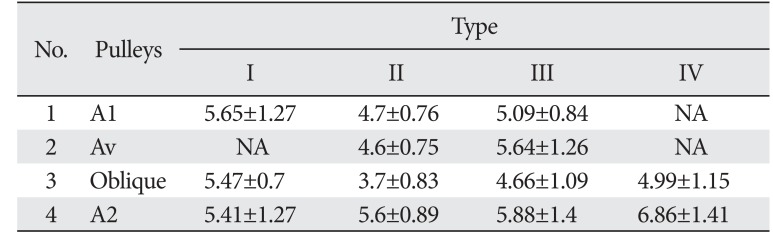
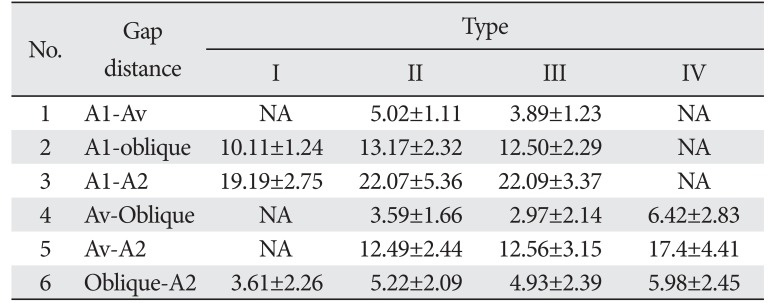
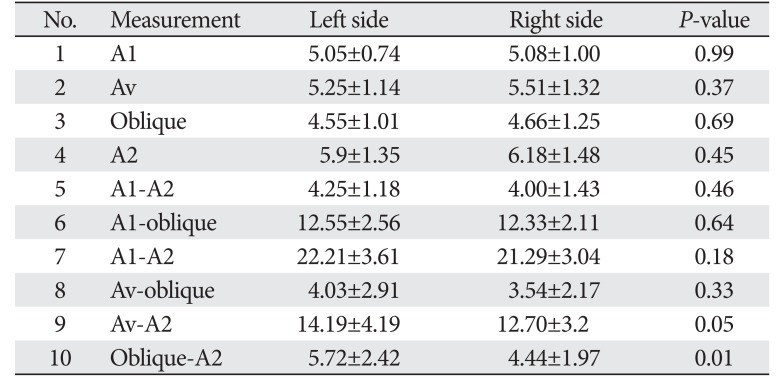
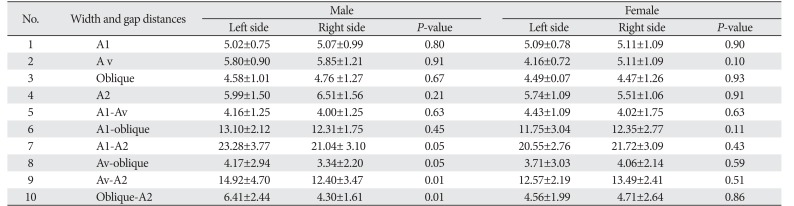
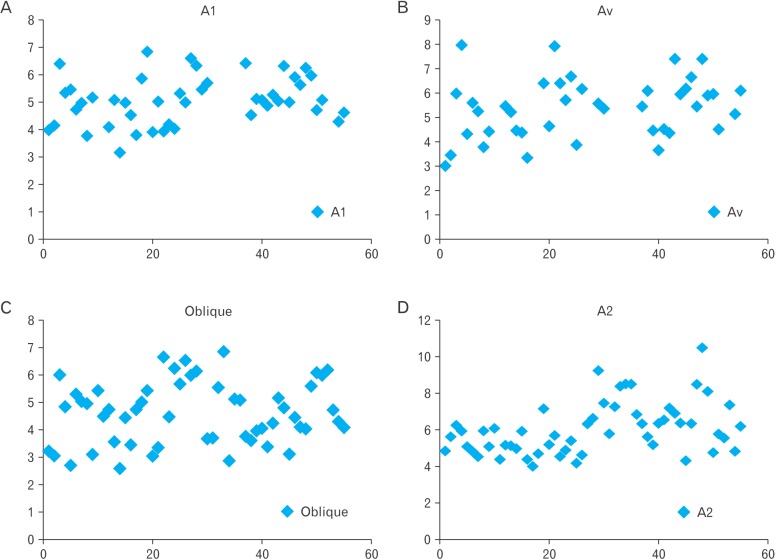
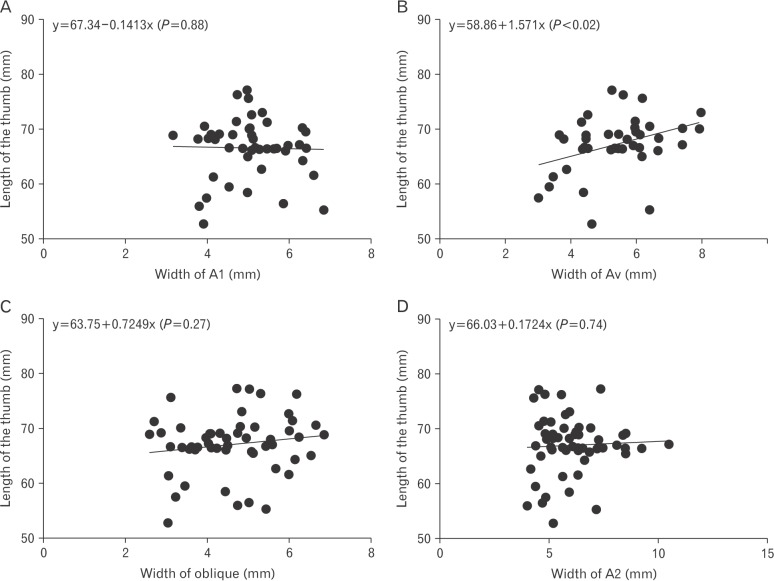
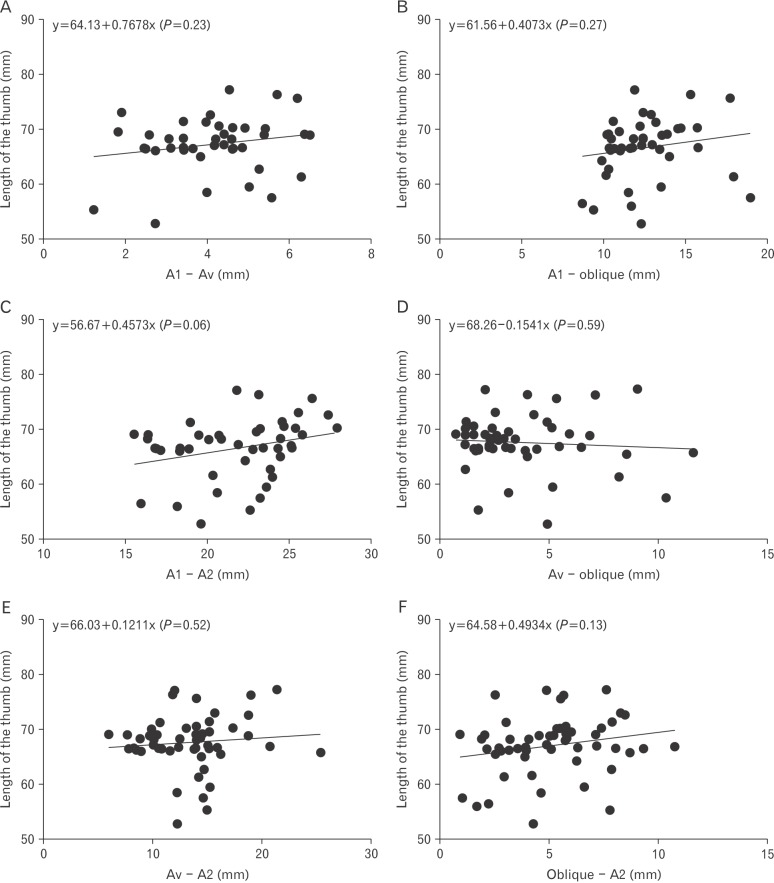
Table 1
Width (mm) of the pulley system of thumb
| No. | Pulleys | Type | |||
|---|---|---|---|---|---|
| I | II | III | IV | ||
| 1 | A1 | 5.65±1.27 | 4.7±0.76 | 5.09±0.84 | NA |
| 2 | Av | NA | 4.6±0.75 | 5.64±1.26 | NA |
| 3 | Oblique | 5.47±0.7 | 3.7±0.83 | 4.66±1.09 | 4.99±1.15 |
| 4 | A2 | 5.41±1.27 | 5.6±0.89 | 5.88±1.4 | 6.86±1.41 |
![]()
Table 2
Gap distance (mm) between pulleys of the thumb
![]()
Table 3
Width and gap distances (mm) of pulleys of the thumb related to left and right side
![]()
Table 4
Width and gap distances (mm) of pulleys of the thumb related to genders
![]()
Go to :
Discussion
Trigger finger is one of the commonest finger aliment that hand surgeons encounters and treat. The lifetime risk of developing trigger finger is about 2%–3%. It is more common in the thumb (trigger thumb) and index finger indicating that it develops due to repetitive finger movements and local trauma [57]. However, few studies have failed to prove this correlation [9]. It can be idiopathic also. Few conditions such as diabetes mellitus, amyloidosis, rheumatoid arthritis predisposes to trigger thumb [10]. Trigger thumb may occur due to a mismatch between the pulley and FPL tendon which impairs smooth gliding of the tendon inside it. This may occur due to FPL tendinosis with a nodule or thickening of A1 pulley or tenosynovitis [11]. The first annular pulley (A1) it the most affected pulley as it is the site of maximal tendon excursion [10]. It manifests as pain, swelling and discomfort in the thumb with characteristic clicking sound when thumb flexion and extension occurs. In severe cases, there is locking of thumb in a flexed position. Medical management includes resting the thumb from repetitive movements, splinting in the extended position, analgesics, and anti-inflammatory drugs. This is effective in about 90% cases. Surgical release of A1 pulley is done when conservative medical management fails [12].
The A1 pulley was situated anterior to the metacarpophalangeal joint extending distally to the base of the proximal phalanx. The situation of the pulley is similar to the previous studies and there was no variant anatomy with regard to its location. The fibers of the A1 pulley have been classified as annular, proximal annular, and distal oblique type and superimposed type [13]. However, in our study, the fibers of the A1 pulley were predominantly the annular type and with few thumbs demonstrating proximal annular and distal oblique fibers. In some of the dissected thumbs, the oblique and annular fibers were superimposed.
The mean width of A1 pulley described in various studies are 5.4, 6.00, 6.1, 5.3, and 6.8 mm, respectively [2571415]. In the present study, the mean value of A1 pulley was almost similar to above studies. There was no data in the literature to compare the mean width of A1 pulley on right and left sides. The measurement of A1 pulley in various types was comparable with the previous study (6.2, 5.5, 5.1, and 5.8 mm). However, A1 width in type II was smaller and in type IV was not measured as it was fused with fibers of Av pulley with no gap distance between them [5].
Av pulley was located at the proximal portion of the proximal phalanx. The fibers of Av pulley were either annular or oblique. The annular fibers either remained separate from the A1 pulley or fused with it. In 7% cases, Av pulley was absent. The mean width of Av pulleys reported by various studies is 5.8, 5.5, and 5.9 mm, respectively which is comparable to our study (5.38 mm) [245].
Oblique pulley was also located over the proximal phalanx distal to the Av pulley. The overall width of the oblique pulley (4.1 mm) reported by Bayat et al. [2] is comparable to our study. However, it is greater than that reported by Schubert et al. [5] which was 3.2 mm. The mean width of oblique pulley reported by the previous study according to four different morphological patterns (type I, II, III, and IV) of the pulley is 5.1, 3.1, 3.1, and 3.3 mm, respectively [5]. The results obtained from our study are similar to the above values except type III and type IV that are increased. A2 pulley was located anterior to interphalangeal joint and its fibers were annular. The overall width of A2 pulley and its width with regard to four morphological types obtained in our study were similar to previous study by Schubert et al. [5].
According to Doyle and Blythe [3] sectioning experiment the oblique pulley is necessary to prevent bowstringing of the FPL tendon. However, it was documented later that A1 pulley also plays a significant role in preventing bowstringing together with the oblique pulley. Hence reconstruction of either A 1 or oblique pulley is essential to restore the normal thumb kinematics [16]. Esplin et al. [17] concluded that intact A1 or oblique pulley equally maintain the normal excursion of the FPL tendon. But both these studies were done before a distinct Av pulley was described in the thumb. Therefore, Bayat et al. [2] could not compare their biomechanical study results with the previous studies that did not include Av pulley. However, from his study, they concluded that intact oblique pulley alone could not prevent bowstring of FPL tend and either intact A1 or Av pulley is needed to prevent bowstringing. Biomechanical study by Zissimos et al. [16] showed that the contribution made by the A2 pulley in maintaining the arc of the thumb is minimal. Few studies have reported that in addition to the A1 pulley, the Av pulley can be an additional site of a stenosis. It was hypothesized that incomplete release of the Av pulley could lead to recurrence of trigger thumb in this case [1115].
The knowledge of gap distances can play a significant role in percutaneous or minimally invasive surgeries of the pulleys to avoid excessive release and injury to the adjacent pulley leading to bowstringing or under release causing recurrence of trigger thumb. When both A1 and Av pulley are ruptured, surgical reconstruction of either A1 or Av pulley would be enough to regain normal thumb motion without bowstringing of FPL tendon [4].
The anatomical knowledge regarding morphologic and morphometry of pulley system is essential in the advancing percutaneous surgical techniques like thread trigger finger release [18]. Closed flexor tendon pulley injuries are uncommon in the thumb. A case of closed rupture of both A1 and the oblique pulley was reported as a result of corticosteroid injection in treating trigger thumb. A single palmaris longus tendon autograft was used to reconstruct both A1 and oblique pulley [8]. Similar case has occurred as a result of the sudden passive extension of a flexed thumb similar to the mechanism of long finger pulley rupture [19]. The anatomical knowledge regarding the pulley system of the thumb adds to the existing data. This may help in surgical treatment of trigger thumb, with less complication and in reconstruction of the closed rupture of the pulley of the thumb.
Go to :
 XML Download
XML Download