

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The objectives of cancer staging are as follows: identify patient prognosis, aid in planning of treatment, and evaluate treatment results [1]. Therefore, accurate staging is a fundamental process, and the staging system should be simple, accurate, and reproducible [2]. With respect to this, traditional cancer staging systems have been based on the anatomical extent of tumors and have been represented as tumor, node, metastasis (TNM) staging: the extent of the primary tumor (T), lymph node (N) involvement, and presence of distant metastasis (M). With the increase in the knowledge on cancer biology, classic TNM staging, which was only based on anatomical factors, has been modified to include biologic factors that are associated with patient prognoses, and such modified staging systems have been proposed for various cancers [3]. These modifications are expected to provide additional precision and flexibility to the staging system.
Gastric cancer is one of the leading causes of death worldwide [4], and it is a heterogeneous disease that causes various treatment outcomes in clinical practice. To understand the biology of gastric cancer and improve treatment outcomes, the molecular characteristics of gastric cancer have been evaluated, and the classifications of tumor biology have been proposed [567]. These efforts provide an invaluable insight on the biology of gastric cancer; however, the clinical implication of these classifications has not been validated in other cohorts. Consequently, these results have not been adopted in current clinical practices [8].
Using the knowledge on the up-to-date molecular classifications of gastric cancers, single patient classifier (SPC) algorithms [9] were recently developed based on a four-gene real-time reverse transcription-polymerase chain reaction (RT-PCR) assay that differentiates among 3 different prognostic groups (low-, intermediate-, and high-risk) for patients with stage II/III gastric cancer, and these results were validated in a subset of patients from the Capecitabine and Oxaliplatin Adjuvant Study in Stomach Cancer (CLASSIC) trial [10], which is a randomized controlled trial showing the benefits of adjuvant capecitabine plus oxaliplatin followed by D2 gastrectomy compared to surgery alone. Patient stratification using the SPC algorithm reflected the biology of tumor microenvironment, such as immune cell infiltrations, which are significantly associated with patient prognoses. Because such prognostic groups of the SPC algorithm (prognostic single patient classifier; pSPC) were independent of prior prognostic factors and TNM stage [9], the modified TNM staging system with pSPC information may have a better prognostic performance than the current TNM staging system (the American Joint Committee on Cancer [AJCC] 8th edition staging system) [3] for patients with gastric cancer. To evaluate this hypothesis, we investigated the clinical impact of pSPC in an independent cohort and compared the prognostic performance of the modified TNM staging system based on pSPC with the current AJCC 8th edition staging system in multiple cohorts.
MATERIALS AND METHODS
Patient cohorts in this study
To elaborate and confirm the results of a previous study that discovered and validated the clinical utility of the pSPC [9], the data of 652 patients who underwent surgery with curative intent for stage II/III gastric cancer at Yonsei Cancer Center between January 1, 2000 and December 31, 2004 were evaluated (defined as Cohort_C). The inclusion criteria were as follows: 1) patients who were 18 years or older with histologically confirmed gastric cancer, 2) those with pathologic stage II and III gastric cancer according to the AJCC 6th edition staging system, 3) those who underwent D2 gastrectomy with curative intent, 4) those without macroscopic and microscopic residual tumor, and 5) those with formalin-fixed paraffin-embedded (FFPE) tumor tissue. Meanwhile, the exclusion criteria were as follows: 1) those who received chemotherapy or radiation therapy before surgery, 2) those with an RNA level from the FFPE tumor section of less than 400 ng, and 3) those with an RNA quality from the FFPE tumor section (A260/280) of less than 1.8. This study was approved by the Institutional Review Board of Yonsei University College of Medicine Severance Hospital (1-2017-0003).
In a previous study [9], the SPC RT-PCR assay kit (nProfiler I; Novomics Co., Ltd., Seoul, Korea), which is based on 4 identified classifier genes (GZMB, WARS, SFRP4, and CDX1) and 5 reference genes (ACTB, ATP5E, HPRT1, GPX1, and UBB), was used to evaluate 307 patients with gastric cancer (Cohort_E). Its clinical impact was validated in an independent cohort of patients who were treated in the CLASSIC trial (ClinicalTrials.gov, NCT00411229; underwent D2 gastrectomy and received adjuvant capecitabine and oxaliplatin chemotherapies [n=323] or underwent surgery alone [n=302] for gastric cancer) [10], and this cohort was defined as Cohort_V (n=625) in this study. These 2 cohorts (Cohort_E and Cohort_V) were revisited, and 1,584 patients were finally enrolled in the present study (307 from Cohort_E, 625 from Cohort_V, and 652 from Cohort_C).
Identification of the SPC
Two pieces of 3-mm tumor tissue cores were obtained from the FFPE samples, and RNA was extracted using the MasterPure Complete DNA and RNA Purification Kit (Epicentre Technologies, Madison, WI, USA). Patients were classified into 3 groups (low-, intermediate-, and high-risk) according to the pSPC testing with a commercial Good Manufacturing Practice grade kit (nProfiler I; Novomics Co., Ltd.). Briefly, the positive expression of both GZMB and WARS defined the low-risk (highly immune) group. Among the other patients (low immune), the expression of SFRP4 (stem-like classifier gene) stratified patients into the intermediate-risk (SFRP4-negative) and high-risk (SFRP4-positive) cohorts.
Modified TNM staging based on the pSPC algorithm
To determine whether the pSPC algorithm can be adapted to the TNM staging system, provide better stratification, and predict prognosis, we compared the prognostic performances of the 8th edition of the AJCC and modified TNM staging systems, considering the pSPC. For the modification of the TNM staging system, one-grade down-staging was applied to all patients who were classified into the low-risk group based on the pSPC algorithm in the AJCC 8th edition staging system; otherwise, for the intermediate- and high-risk groups, the modified TNM and AJCC 8th edition staging systems were identical. That is, if a patient with stage IIIA gastric cancer according to the AJCC 8th edition staging system was classified as low-risk based on the pSPC algorithm, the revised TNM was IIB.
Statistical analysis
Categorical and continuous variables were presented as number with percentage and mean with standard deviation, respectively. Survival data were represented by overall survival (OS) and disease-free survival (DFS), which were defined as time from surgery to death by any cause and the time from surgery to recurrence or death by any cause, whichever occurred first, respectively. The Kaplan-Meier curves and adjusted Cox survival estimates were used to generate survival curves. The log-rank test and Cox proportional hazard model were utilized to compare prognoses. Harrell's C-index was used to compare the prognostic performance of each staging system [11]. A P-value <0.05 was considered statistically significant. The IBM Statistical Package for the Social Sciences software version 20.0 (SPSS Inc., Chicago, IL, USA) and R software version 3.4.3 with “survival” and “compareC” packages were used for statistical analyses (R Project for Statistical Computing, Vienna, Austria).
RESULTS
Patient demographics
The mean age of Cohort_C was 57.3 (±11.9) years, and of the participants, 226 (34.7%) were women. The most common tumor location was in the antrum (n=345, 52.9%), and 567 (87.0%) gastric cancer cases involved over the proper muscle layer (pT3/T4). A total of 229 patients (35.1%) had stage II cancer, and the remaining patients had stage III cancer. Most of the patients (94.5%) in this cohort received adjuvant chemotherapy after surgery. Moreover, 84 (12.9%), 253 (38.8%), and 315 (48.3%) of the patients were classified as low, intermediate, or high-risk using the pSPC algorithm, respectively. The demographic characteristics of the overall population (n=1,584) (Cohort_E [n=307], Cohort_V [n=625], and Cohort_C [n=652]) were similar to those of Cohort_C, as described in Table 1.
Table 1
Demographic and clinical characteristics of patients with gastric cancer
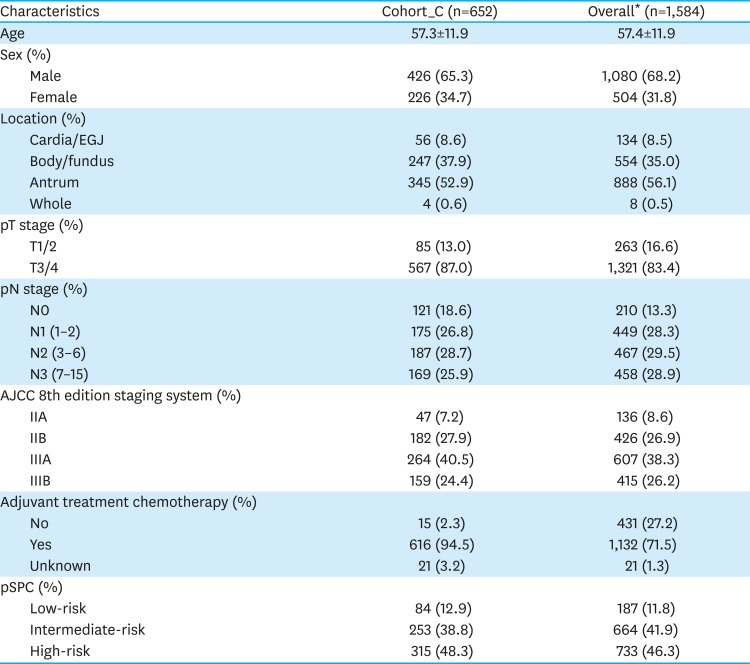
Cohort_C = confirmation cohort; EGJ = esophago-gastric junction; AJCC = American Joint Committee on Cancer; pSPC = prognostic single patient classifier; CLASSIC = Capecitabine and Oxaliplatin Adjuvant Study in Stomach Cancer.
*Overall cohort includes the present Cohort_C (n=652), the evaluation cohort for developing single patient classifier (n=307), and the validation cohort (n=625), which was a part of the CLASSIC trial in a previous study [9].
Prognosis of patients with gastric cancer according to the pSPC algorithm
The prognosis of patients with stage II/III gastric cancer in Cohort_C was well stratified according to the pSPC algorithm. The 5-year OS rates of the low-, intermediate-, and high-risk groups were 82.0%, 66.2%, and 56.1%, respectively, and this difference was statistically significant (Fig. 1A, log-rank P<0.001). In the overall population, a similar outcome was observed. That is, the 5-year OS rates of the low-, intermediate-, and high-risk groups were 82.7%, 71.0%, and 59.9%, respectively (Fig. 1B, log-rank P<0.001). The prognoses according to the pSPC algorithm were still statistically significant when the TNM stage was adjusted using the Cox proportional hazard model. The adjusted hazard ratios (HRs) of the intermediate-risk group compared to the low-risk group were 2.06 and 1.96 in Cohort_C and the overall population, respectively (P=0.001 and P<0.001, Fig. 1C and D). The adjusted HRs of the high-risk group compared to the intermediate-risk group were 1.25 (95% confidence interval [CI], 0.99–1.57) and 1.30 (95% CI, 1.10–1.53) in Cohort_C and the overall population, respectively. The adjusted HRs of high-risk group compared to low-risk group were 2.58 (95% CI, 1.68-3.95, P<0.001) and 2.54 (95% CI, 1.84-3.50, P<0.001) in Cohort_C and the overall population, respectively.
Fig. 1
Classification of the Kaplan-Meier curves and Cox survival estimates for the OS of patients using the pSPC in Cohort_C and in the overall population. (A) Kaplan-Meier curves of the patients in Cohort_C, (B) Kaplan-Meier curves of the patients in the overall population, (C) Cox survival estimates that were adjusted by TNM stages in Cohort_C, and (D) Cox survival estimates that were adjusted by TNM stages in the overall population.
OS = overall survival; pSPC = prognostic single patient classifier; TNM = tumor, node, metastasis; HR = hazard ratio; CI = confidence interval.
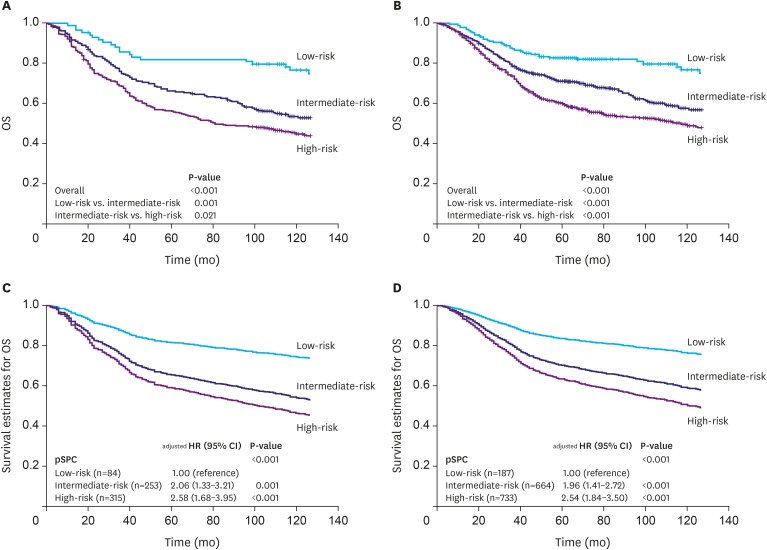
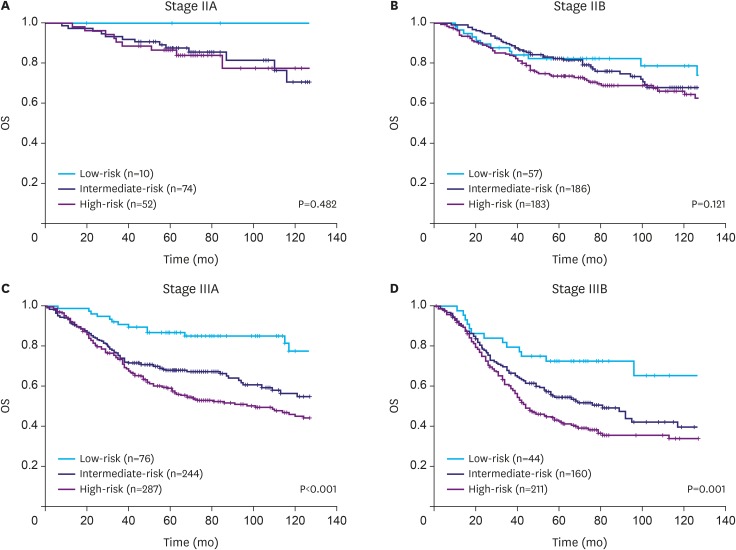
Fig. 2 depicts the results of the subgroup analyses for the prognosis of pSPC by TNM sub-stages in the overall population. The OS of the low-risk group was the best for patients with stage IIA and IIB cancer, although the differences were not statistically significant (log-rank P=0.482 and 0.121, respectively; Fig. 2A and B). The prognosis according to the pSPC algorithm was significantly different for stages IIIA and IIIB (log-rank P<0.001 and 0.001, respectively; Fig. 2C and D). However, the prognoses of the intermediate- and high-risk groups were not statistically significant in stages IIIA and IIIB (log-rank test P=0.091 and 0.194, respectively). To improve the modified TNM staging system as a prognostic tool, we applied one-grade down-staging to all patients who were classified into the low-risk group according to the pSPC in the AJCC 8th edition staging system.
Fig. 2
Classification of the Kaplan-Meier curves for the OS of patients using the pSPC in each stage; (A) stage IIA, (B) stage IIB, (C) stage IIIA, and (D) stage IIIB, according to AJCC 8th edition staging system.
OS = overall survival; pSPC = prognostic single patient classifier; AJCC = American Joint Committee on Cancer.
Comparison of patient distributions and prognostic performances between the AJCC 8th edition staging and revised TNM staging with pSPC
The patient distributions for the AJCC 8th edition staging system and modified TNM with pSPC staging systems in terms of overall populations are shown in Table 2. A total of 187 (11.8%) patients who were classified as low-risk according to the pSPC algorithm underwent one-grade down-staging in the modified TNM staging system compared to the AJCC 8th edition staging system.
Table 2
Patient distributions for the AJCC 8th edition staging system and the revised TNM staging system with a pSPC for stage II/III gastric cancer

| Modified TNM | AJCC 8th edition staging system | ||||
|---|---|---|---|---|---|
| IIA | IIB | IIIA | IIIB | Total | |
| IB | 10 | 0 | 0 | 0 | 10 |
| IIA | 126 | 57 | 0 | 0 | 183 |
| IIB | 0 | 369 | 76 | 0 | 445 |
| IIIA | 0 | 0 | 531 | 44 | 575 |
| IIIB | 0 | 0 | 0 | 371 | 371 |
| Total | 136 | 426 | 607 | 415 | 1,584 |
The Kaplan-Meier curves showed that the prognoses of each sub-stage were well stratified in both the AJCC 8th edition and modified TNM staging systems in terms of OS and DFS (Fig. 3). Using Harrell's C-index, the prognostic performance of the modified TNM staging system was evaluated, and results showed that its prognostic performance was better than that of the AJCC 8th edition staging system in multiple cohorts (Cohort_E, Cohort_V, and Cohort_C). In the overall population, the C-indices of the modified TNM with the pSPC system for OS and DFS were 0.635 and 0.639, respectively, which were significantly higher than those of the AJCC 8th edition staging system (0.620 and 0.624, respectively; P<0.001 and P<0.001; Table 3).
Fig. 3
Kaplan-Meier curves for the OS and DFS of the AJCC 8th edition and revised TNM staging systems; (A) OS of the AJCC 8th edition staging system, (B) OS of the modified TNM, (C) DFS of the AJCC 8th edition staging system, and (D) DFS of the modified TNM staging system.
OS = overall survival; DFS = disease-free survival; AJCC = American Joint Committee on Cancer; TNM = tumor, node, metastasis.
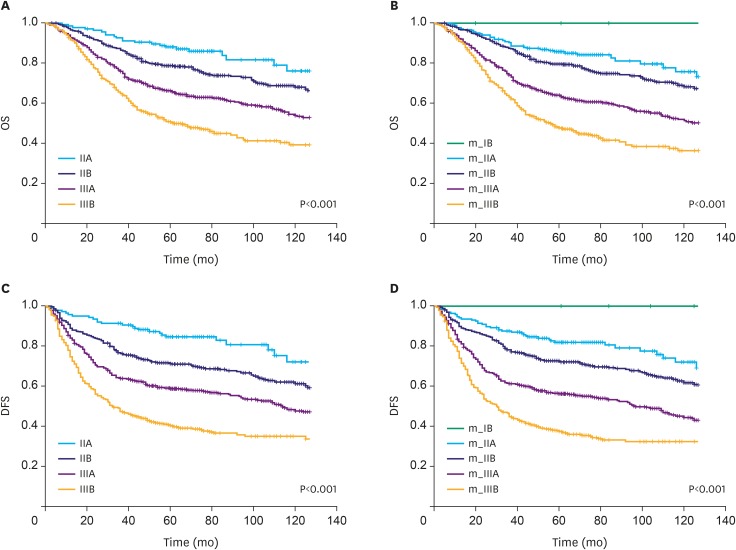
Table 3
Prognostic performance (Harrell's C-index) of the AJCC 8th edition and revised TNM staging systems according to the pSPC systems for stage II/III gastric cancer

DISCUSSION
TNM staging has been periodically updated based on advancements in our knowledge about cancer. Adapting cancer biology, which has been continuously informing clinical oncology, to classical anatomy-based staging was one of a major watershed events for cancer staging after the AJCC 7th edition [12]. The recent AJCC 8th edition staging system succeeds this trend, and it provides non-anatomic prognostic factors with evidence levels for defining cancer stage groups, with the expectations that such approaches can bridge medicine from population-based to personalized [3].
Recent high-technology platforms, rather than classical anatomy and histology-based approaches, have been used in assessing cancers at genomic levels, and the results have improved our understanding of cancer. Previous studies on gastric cancer have suggested that the condition can be classified into several subtypes according to molecular characteristics [56]. The Cancer Genome Atlas suggested 4 molecularly distinct subtypes of gastric cancer based on the results from the use of various molecular platforms: Epstein-Barr virus, microsatellite instability (MSI), chromosomal instability (CIN), and genomically stable [5]. The Asian Cancer Research Group proposed another 4 distinct molecular subtypes of gastric cancer that were based on mRNA expression data: MSI, microsatellite stable and epithelial mesenchymal transition (MSS/EMT), MSS/TP53+ (p53 active), and MSS/TP53− (p53 inactive) [6]. This knowledge was used to identify candidate genes that represent the characteristics of gastric cancer, and we developed a four-gene-based SPC that can be directly used in clinical practice [9].
In this study, we showed that the pSPC data provides meaningful prognostic information for patients with resectable stage II/III gastric cancer in an independent cohort (Cohort_C). In addition, the modification of the TNM staging with the pSPC information had a better prognostic stratification of OS, DFS, and prognostic performance than the current AJCC 8th edition staging system for stage II/III gastric cancer across multiple cohorts (Cohort_E, Cohort_V, Cohort_C, and the overall population). This result implies that a staging system that uses tumor biology can provide better information to appropriately stratify gastric cancer into homogeneous prognostic subgroups. Several biological characteristics of tumors may be used as prognostic indicators, which include the intra-tumoral infiltrations of cytotoxic T lymphocytes, the extent of which were quantified and translated herein as the low-risk group according to the pSPC. Additional biomarkers, such as MSI status and programed cell death ligand 1 expression, that are associated with the prognosis of gastric cancer [131415], could be considered for future TNM staging updates if such results reproduce in other independent cohorts.
The present study has some limitations. First, only the low-risk group in the pSPC was utilized in the modification of TNM staging system because the prognostic power of the low-risk group was remarkable over the high-risk group compared to the intermediate-risk group in the overall cohort. Second, future studies with more cohorts must be conducted to verify its clinical validity in the incorporation of the high-risk group into the TNM staging system. The patients who were enrolled this study were diagnosed with stage II/III gastric cancer according to the 6th edition of the AJCC staging system. Consequently, the prognostic performance of the pSPC-modified TNM staging system for patients with stage I, IIIc, and IV gastric cancer was not addressed in the present study, and this could be attributed to the relatively low C-indices of the TNM staging systems compared to those of other studies [1617]. Third, one of the major changes from the 7th to 8th edition of the AJCC staging system for gastric cancer is staging migration for patients with more than 15 metastatic lymph nodes; however, the cohorts in this study did not include these patients because the condition was classified as stage IV according to the 6th edition of the AJCC Staging system. Whether this result is applicable to non-Asian patients with gastric cancer, for whom perioperative chemotherapy is used as a standard treatment, should be investigated to understand if results can be generalized to a wider range of patients with gastric cancer.
In conclusion, the pSPC is an independent prognostic factor, along with TNM stage, for resectable stage II/III gastric cancer. pSPC should be considered for gastric cancer staging in future clinical practices and staging systems.
 XML Download
XML Download