

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Although the incidence of gastric cancer in Korea is gradually decreasing, it is still the second most prevalent type of cancer and the third most common cause of death. There is an increased risk of developing gastric cancer with increasing age [12]. With advances in surgery, gastric surgeons often come across elderly patients who need surgical treatment for gastric cancer [3]. The appropriate treatment of elderly patients with gastric cancer has always been a major challenge. The patients' families often weigh the risks and benefits of surgical treatment before making a decision. Initially, this issue, performing surgical treatment or not in far elderly patient, was not dealt with so often. Large-scale Surveillance, Epidemiology and End Results (SEER) data revealed that age alone is not a contraindication for cancer treatment in most elderly patients. However, the data indicated low survival rate during the first year of diagnosis [4]. This reflects the negative impact of cancer treatment on patients' survival, especially in the first year. Hence, a more practical approach towards cancer treatment for the elderly needs to be developed.
There are varying criteria to classify a patient as elderly. Theoretically, elderly can be defined as a person who is older than 65 years of age according to the World Health Organization (WHO) criteria; however, most surgeons do not agree with this definition for clinical studies. Other definitions have been suggested, but no specific number can exactly reflect the biological age criteria. Therefore, we considered a novel criterion for classifying an individual as elderly, on the basis of the average lifespan of the specific country in which the study was performed. The average lifespan can reflect the biologic age criteria to some extent.
Laparoscopic gastrectomy has become a standard treatment for gastric cancer. It has been proven to reduce post-operative complications compared with open gastrectomy, in the KLASS-01 results [5]. In an era where minimal invasion is preferred, laparoscopic gastrectomy for elderly patients with gastric cancer is worth exploring. Before proceeding with the surgery, a plan of post-operative care and quality of life after surgery are also necessary. Thus, we planned to evaluate the safety and efficacy of laparoscopic gastrectomy in very elderly patients.
MATERIALS AND METHODS
Patient selection
We performed a retrospective analysis of a prospectively collected database. In all, 856 patients who underwent laparoscopic gastrectomy for gastric cancer between 2004 and 2015, performed by a single surgeon (W Kim), were enrolled in this study. The laparoscopic approach was employed for all patients with gastric cancer except for those exhibiting tumors with definite serosal invasion. From this database, 14 patients with stage IV cancer, 5 patients who had undergone a partial surgery, and 1 patient with carcinoid tumor were excluded. The remaining 836 patients were divided into the elderly group (EldG) (men: ≥77 years, women: ≥84 years) and non-elderly group (nEldG) (men: <77 years, women: <84 years) considering the average lifespan of the Korean population for the year 2010. This year was selected because 2010 marked the median period of our study. Basic clinicopathologic characteristics and surgical outcomes were compared between the 2 groups.
Surgical procedures were followed according to the Japanese gastric cancer treatment guidelines [6]. Patients with stage II or III cancer underwent adjuvant chemotherapy with S-1 for 1 year. Post-operative complications were considered as events that occurred within 30 days after surgery, and post-operative mortality was defined as death within 30 days after surgery or death directly related to the surgical procedure. This study protocol was reviewed and approved by the Institutional Review Board of Yeouido St. Mary's hospital (IRB number: SC17RESI0085).
Propensity score matching analysis
To eliminate a bias in the basic characteristics, a propensity score matching was done for covariates, including sex, tumor depth, node status, and extent of resection. Score-matched patients were also compared in terms of their clinicopathologic characteristics and surgical outcomes. In addition, overall and cancer-specific survival rates were compared between the 2 groups. Risk factor analysis for post-operative complications and overall survival (OS) were performed considering various variables, including age, American Society of Anesthesiologists (ASA) score, tumor, node, metastasis (TNM) stage, and complication occurrence.
Statistical methods
Categorical variables were compared using Pearson's χ2 test, and continuous variables were compared using the Student's t-test. All continuous variables are expressed as means±standard deviation. Survival analysis was performed using the Kaplan-Meier method and log-rank test. Multivariate risk factor analysis for OS was performed using the logistic regression model. All statistical results were considered significant when the P-value was less than 0.05. Statistical analyses were performed using the SPSS statistical software version 18.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Clinicopathologic characteristics and surgical results
Of the 780 patients in the nEldG, 56 were considered for further analyses after propensity score matching with the patients in the EldG. On comparing the clinicopathologic characteristics, the EldG showed a higher ASA score and a higher rate of comorbidities. The incidence of hypertension was nearly 2 times higher in the EldG (28/56, 50%) than in the nEldG (18/56, 32.1%), with a marginal significance (P=0.055). Nearly the same distribution of tumor depth, lymph node metastasis, and cancer stage was observed following matching between the 2 groups (Table 1).
Table 1
Clinicopathologic characteristics between elderly and non-elderly patients in the entire study population and in the matched population

Continuous variables were presented with mean±standard deviation and compared with Student's t-test. Nominal variables were presented with a number (%) and compared with χ2 analysis.
EldG = elderly group; nEldG = non-elderly group; BMI = body mass index; ASA = American Society of Anesthesiologists; pT = pathologic tumor; pN = pathologic node; pTNM = pathologic tumor, node, metastasis.
![]()
After propensity matching, 3 types of resection based on the extent of surgery were considered. A pylorus-preserving gastrectomy was performed only in the nEldG. Distal gastrectomy was performed on 42 (75.0%) and 43 (76.8%) patients of the EldG and nEldG, respectively. D2 lymph node dissection was performed more often in the nEldG (69.6%) than in the EldG (44.6%), and the number of retrieved lymph nodes and surgical time were less in the EldG (Table 2).
Table 2
Surgical results between the elderly and non-elderly patients in the entire study population and in the matched population

Continuous variables were presented with mean±standard deviation and compared with Student's t-test. Nominal variables were presented with a number (%) and compared with χ2 analysis.
EldG = elderly group; nEldG = non-elderly group; PPG = pylorus-preserving gastrectomy.
![]()
There were no statistical differences in the rate of post-operative complications, both, in terms of overall complications and complications with Clavien-Dindo IIIa or more (Table 3). Additionally, there was no difference in the in-hospital mortality between the groups. Although the rate of other specific types of complications was similar between the groups, pulmonary complications developed more frequently in the EldG than in the nEldG (EldG vs. nEldG, 8.9% vs. 0%, respectively; P=0.022).
Table 3
Details of complications between the EldG and nEldG in the matched population

Nominal variables were presented with a number (%) and compared with χ2 analysis.
EldG = elderly group; nEldG = non-elderly group; NS = not significant.
![]()
Survival and risk factor analysis
Fig. 1 shows survival analysis between the EldG and nEldG. The 5-year OS rate was significantly lower in the EldG than in the nEldG in the matched population (EldG vs. nEldG, 51.5% vs. 80.9%, respectively; P=0.006) However, there was no difference in cancer-specific survival between the 2 groups (EldG vs. nEldG, 88.4% vs. 88.0%, respectively; P=0.385). In addition, there was no difference in the disease-free survival between the groups. In all, 8 and 16 patients died in the nEldG and EldG, respectively. Two (25%) and 8 patients (50%) died within a year of the surgery in the nEldG and EldG, respectively. Two patients in the nEldG and 6 patients in the EldG died of non-cancer-related problems.
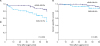 | Fig. 1Survival analysis between the EldG and nEldG: (A) OS, (B) cancer-specific survival.
EldG = elderly group; nEldG = non-elderly group; OS = overall survival.
|
On univariate and multivariate risk factor analyses for overall mortality, age, ASA score, TNM stage, and development of complications were found to be related to a significant reduction in OS (Table 4).
Table 4
Risk factor analysis for OS in matched groups

OS = overall survival; CI = confidence interval; EldG = elderly group; nEldG = non-elderly group; BMI = body mass index; ASA = American Society of Anesthesiologists; pTNM = pathologic tumor, node, metastasis.
![]()
DISCUSSION
Elderly patients are known to develop more postoperative complications after major abdominal surgery, because of pre-existing comorbidities and low functional reserves [789]. Gastric cancer needs a major surgery to prevent metastasis. For decades, laparoscopic surgery has been generally adopted in every field of surgery. Randomized clinical trials, as well as many retrospective studies, have revealed advantages of laparoscopic gastrectomy over open gastrectomy in terms of early recovery, less pain, and fewer complications [51011]. There have been several attempts to explore the feasibility of gastrectomy in elderly patients because of changes in the average lifespan globally [121314]. Similar results for elderly patients, such as less blood loss and early recovery of the patients ≥80 years of age, have been reported. In addition, a meta-analysis comparing laparoscopic gastrectomy with open gastrectomy for elderly patients with gastric cancer revealed less blood loss, shorter hospital stays, and fewer postoperative complications in the laparoscopic group [15].
Once the benefits of laparoscopic gastrectomy for gastric cancer were fully established, many studies focused on comparing the short and long-term results between the elderly and non-elderly patients. The objective was to explore whether surgical treatment for specific elderly patients would be beneficial for their remaining lifespan. One study reported that non-cancer-specific deaths in elderly patients with clinical stage I gastric cancer could be negligible with laparoscopic gastrectomy [12]. In our study, 5 patients with stage I gastric cancer died of non-cancer-related reasons within a year of surgery. Considering the natural course of early gastric cancer, those patients might not have benefitted from the surgical treatment. However, ethical principles do not allow studies which include a surgical and a control groups (a group that does not undergo any treatment for a disease). Thus, to establish the safety or benefit of surgery, surgical results for the very elderly and non-elderly patients can be compared as an alternative. In this study design, the criteria for defining a patient as elderly is debatable because no specific age can exactly reflect the biological age criteria. Yoshida et al. [13] compared elderly and non-elderly patients who underwent laparoscopic distal gastrectomy, defining patients of 65 years of age and above as elderly, and showed a higher incidence of pulmonary complications, delirium, and lower OS in the elderly patients. In a Korean study, 71 elderly (≥70 years) patients were compared with non-elderly patients who underwent laparoscopic total gastrectomy [3]. This study reported that elderly patients were more vulnerable to grade III or higher complications. Another Japanese study, which used 75 years and older as the age for classifying elderly patients, showed no significant differences in the rate of complications between the EldG and nEldG [16]. In this report, age itself was not a significant risk factor for the development of post-operative complications, but ASA score and pre-operative comorbid conditions were important factors for the outcomes of surgery. Age criteria are defined by the individual principal investigators, and no definite criteria exist. Hence, we used the criterion of the average lifespan of the study population to reflect the patients' biologic status as precisely as possible. In addition, there is a definite gap in the average lifespan between men and women. This difference was also considered in this study setting.
In the present study, elderly and non-elderly patients in the entire cohort and in the matched population were compared. Matching was done to eliminate bias regarding sex, tumor stage, and type of resection. The most important difference was the higher ASA score and the higher number of comorbidities in the elderly patient group. Even under this condition, there was no significant difference in the occurrence of post-operative complication, except pulmonary complications, which showed a marginal difference. In this study, laparoscopic gastrectomy seems technically feasible for elderly patients with gastric cancer. In previous studies comparing the results of laparoscopic gastrectomy between elderly and non-elderly patients, age itself was not a significant factor that affected post-operative complications [171819]. Although propensity matching was performed to minimize the bias, more patients with less extensive lymph node dissection were included in the EldG. This might be due to the surgeon's discretion during surgeries in the elderly patients. This could affect the results of comparison of post-operative morbidity and mortality between the 2 groups. However, there was no difference in cancer-specific survival between the groups, and this reflects real-life clinical settings.
The age of elderly patients was a significant independent risk factor for OS, but there was no difference in the disease-free survival between the 2 groups. We estimate that stage of the tumor might be the most powerful factor for OS in patients with gastric cancer. In addition, pre-operative status (ASA score or the number of comorbidities) and incidence of complications were important factors that influenced overall post-operative survival. In the Japanese study, although there was no difference in the recurrence-free survival between the groups, OS in the EldG was lower than that in the nEldG [13]. When assessing survival, we should also focus on the unexpected early mortality, which reflects the patients' general condition by the surgical procedure. The early mortality was found to be related to post-operative complications directly or indirectly. On multivariate analysis of risk factors related to OS, the incidence of complications, tumor stage, ASA score, and combined resection were independent risk factors. Although the development of complications may not affect the overall difference in survival in the entire matched population, it would deteriorate the health of elderly patients with low physiologic reserves compared to non-elderly patients. These events would affect each patient critically. Hence, a more meticulous and safe surgical approach for such elderly patients is necessary.
This study has several limitations. First, the study cohorts were selected from a database retrospectively and may have potential selection bias. To overcome this problem, we performed a propensity-matching analysis. In addition, there is no quality of life data available because of the retrospective design. Second, as the most interesting clinical question is whether laparoscopic surgery is better compared to no surgery in elderly patients who are in average lifespan age or older, this study design has technical limitations. The real valuable study should analysis between surgery group and an observational group among only elderly patients.
In conclusion, laparoscopic gastrectomy can be safely adopted in very elderly patients with gastric cancer who have outlived the average lifespan of the Korean population. However, the survival benefit is still questionable, and meticulous patient selection is highly recommended.
 XML Download
XML Download