

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intestinal dysfunction after abdominal surgery is the leading cause of prolonged hospital stays and additional health-care costs, which has been considered a common and inevitable outcome to some extent [1]. Thus, improving postoperative intestinal dysfunction is of great importance. It is characterized by abdominal distention, nausea, vomiting, delayed passage of flatus or bowel movement. In recent decades, many therapeutic strategies have been used to improve postoperative intestinal dysfunction, such as fast track surgery [2]. However, all have limited efficacy and are not free of side effects.
Daikenchuto (DKT) is one of the most widely administered traditional herbal medicines in the Asia-Pacific area with active components containing Japanese pepper, processed ginger, and ginseng [3]. It has been recently employed to improve intestinal dysfunction [4] and very few side effects have been reported. In intestinal ischemia-related diseases, DKT was associated with ameliorating microvascular dysfunction [5]. Several studies demonstrate that DKT significantly increases superior mesenteric artery blood flow resulting in improvement of intestinal dysfunction [6]. However, the studies regarding DKT in improving postoperative intestinal dysfunction have conveyed inconclusive results [789101112131415]. We therefore conducted a meta-analysis of relevant randomized controlled trials to assess the efficacy of DKT in improving intestinal dysfunction after abdominal surgery.
METHODS
This meta-analysis followed the Cochrane Handbook for Systematic Reviews of Interventions [16] and reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary material 1) [17]. Two reviewers separately conducted literature retrieval, data extraction, quality assessment, and statistical analysis, with inconsistency solved by discussion and by the chief reviewer. Specially, a statistician in our group performed and reviewed the statistical section.
Literature search and inclusion criteria
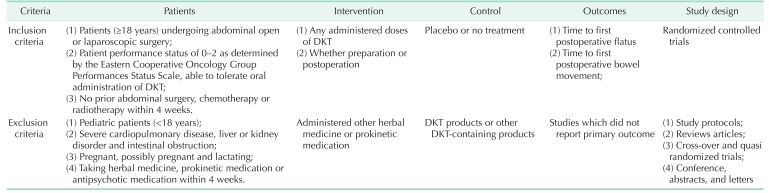
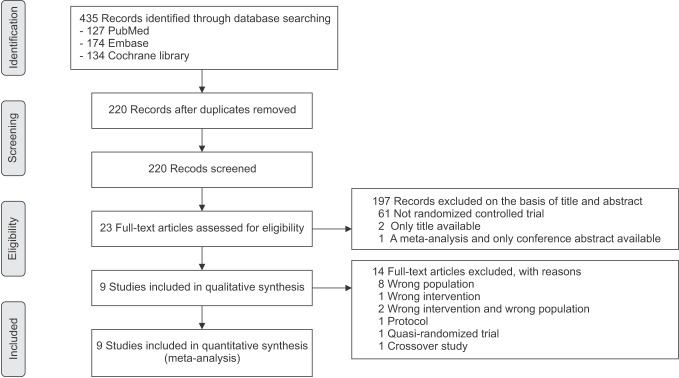
Databases (PubMed, the Cochrane Library, and Embase) were comprehensively searched to identify relevant trials (up to February 10, 2017). The search strategy used the following format terms: “Daikenchuto” or “Dai-kenchu-to” or “Dai-ken-chu-to” or “DKT” or “TJ-100” or “N100” or “TU-100”. DKT, TJ-100, N100, and TU-100 are the trade names of Daikenchuto. No language restriction was imposed. Moreover, reference to relevant articles was examined manually for potentially eligible trials. The whole search process was carried out iteratively until no new publications could be found. Detailed search strategies were attached to Supplementary material 2. We present an adapted PRISMA flowchart showing the process of study selection. We only included randomized controlled trails (RCTs) focused on DKT for intestinal dysfunction in patients after abdominal surgery. Detailed inclusion and exclusion criteria are presented in Table 1.
Data extraction and risk of bias assessment
The following data would be extracted: first author, year of publication, clinical setting, demographic feature (number of patients, age, and sex), type of interventions for DKT, indication of surgery, type of surgery and outcomes, which would be entered into a normalized data collection Excel form (Microsoft Corp., Redmond, WA, USA). Quality assessment was performed by using the guidelines from the Cochrane tool [18]. All included studies were assigned as ‘low,’ ‘unclear’ or ‘high’ risk, using the following criteria: (1) random, (2) allocation concealment, (3) blinding, (4) incomplete outcome data, (5) selective reporting, and (6) other bias by 2 independent investigators.
Statistical analysis
We evaluated the efficacy of DKT on improving postoperative intestinal dysfunction based on the data from included RCTs. The time to first postoperative flatus and the time to first postoperative bowel movement were treated as continuous variables and presented as mean difference (MD) with 95% confidence interval (CI). We calculated standard deviations with standard formulae if only medians and ranges were provided. For studies that had not shown the corresponding results, we extracted data from the Kaplan-Meier curves with the Engauge Digitizer version 4.1 (M Mitchell, Engauge Digitizer; http://markummitchell.github.io/engauge-digitizer) [1920]. Heterogeneity was estimated by using the I2 statistic, a quantitative measure of inconsistency [21]. I2 of less than 50% was regarded as accepted heterogeneity. In cases of significant heterogeneity, a random-effects model was used. Whether heterogeneity was present, sensitivity analyses were conducted to evaluate the robustness of our results. Sensitivity analyses were done according to indication of surgery and type of surgery. In addition, the ‘leave-one-out’ influence analyses were performed to explore the influence of a single study on overall pooled effect estimate by omitting a study each time.
RESULTS
Trial selection
The initial search identified 435 relevant publications. After excluding duplicate studies (n = 214) and publications not relevant to DKT (n = 133), not RCT (n = 61), only title available (n = 2), only conference abstract available (n = 1), 23 studies were reviewed for full text. Apart from protocols (n = 1), wrong population and/or wrong intervention (n = 11), we also eliminated a quasi-randomized trial and a crossover study. For a detailed description, see Supplementary material 3. Finally, 9 RCTs [789101112131415] met inclusion criteria and were included in the final analysis. The selection process is shown in Fig. 1.
Description of eligible studies
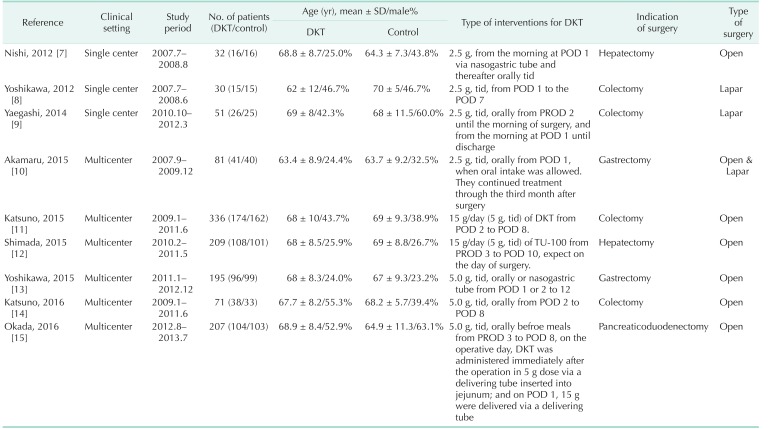
Table 2 summarizes the main feature of the nine RCTs, which were published from 2012 to 2016. The individual total sample sizes ranged from 30 to 336 (total of 1,212 participants). Six hundred eighteen participants were randomized to DKT and 594 to control group. Among these nine RCTs, 6 reported the time to first postoperative flatus [789131415]; 6 reported the time to first postoperative bowel movement [7910111213]. Two studies [89] were about laparoscopic surgery and the others [71112131415] on open procedures. Akamaru et al. [10] reported on laparoscopic and open surgery. Four trials [891114] reported colectomy.
Risk of bias
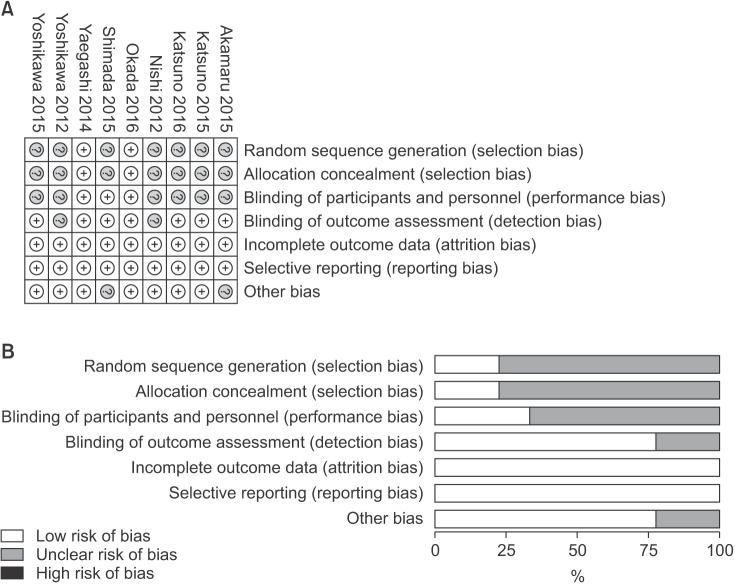
Risk-of-bias details for individual trials were exhibited in Fig. 2A, and the summary of risk of bias in Fig. 2B. Appropriate randomization was produced to avoid possible selection bias in 2 studies [915], which also concealed the allocation sequence using reasonable methods. Two studies [1012] reported their source of funding. As a whole, 2 studies were low risk of bias [915] and others unclear [781011121314].
Quantitative synthesis of data
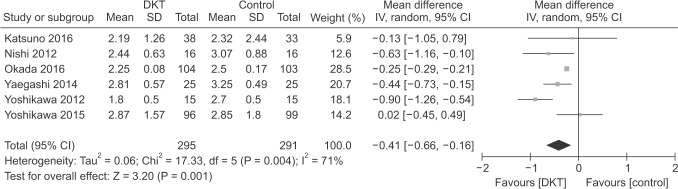
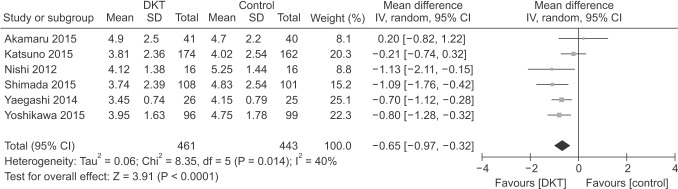
As shown in Figs. 3 and 4, DKT was associated with significantly improving postoperative intestinal dysfunction compared to control group (P < 0.05). Six included studies [789131415] totaling 586 patients (295 in DKT group, 291 in control group) reporting the time to first postoperative flatus. The overall effect favored DKT group (MD, −0.41; 95% CI, −0.66 to −0.16; P = 0.001) (Fig. 3), with significant heterogeneity (I2 = 71%; P = 0.004) (Fig. 3). Moreover, compared with control group, DKT was associated with shortening the time to first postoperative bowel movement (MD, −0.65; 95% CI, −0.97 to −0.32; P < 0.0001) (Fig. 4), without significant heterogeneity (I2 = 40%, P = 0.14) (Fig. 4).
Sensitivity analyses
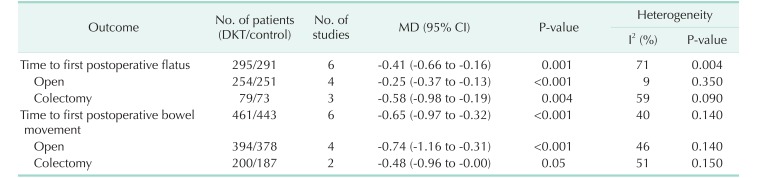
Subsequently, sensitivity analyses were performed to explore the underlying source of heterogeneity and examine the influence of various inclusion criteria on the pooled estimates. The sensitivity analysis in Table 3 based on different inclusion criteria also indicated that DKT was associated with significantly improving postoperative intestinal dysfunction. Inclusion studies of open surgery yielded similar results in the time to first postoperative flatus (4 RCTs; MD, −0.25; 95% CI, −0.37 to −0.13; P < 0.001) (Table 3), with no evidence of heterogeneity (I2 = 9%, P = 0.35), and the time to first postoperative bowel movement (3 RCTs; MD, −0.74; 95% CI, −1.16 to −0.31; P < 0.001) (Table 3), without significant heterogeneity (I2 = 46%, P = 0.14) (Table 3). After inclusion studies of colectomy, the results were still maintained in the time to first postoperative flatus (4 RCTs; MD, −0.58; 95% CI, −0.98 to −0.19; P < 0.004) (Table 3), yet heterogeneity was still present (I2 = 59%, P = 0.09) (Table 3). The studies undergoing colectomy were associated with a slightly decreasing trend in the time to first postoperative bowel movement (2 RCTs; MD, −0.48; 95% CI, −0.96 to −0.00; P = 0.05) (Table 3) with heterogeneity (I2 = 51%; P = 0.15) (Table 3). Furthermore, we performed influence analyses. MD for the time to first postoperative flatus maintained a slight fluctuation from −0.48 (95% CI, −0.77 to −0.20] to −0.28 (95% CI, −0.41 to −0.15), and bowel movement −0.76 (95% CI, −1.07 to −0.45) to −0.57 (95% CI, −0.91 to −0.22) after exclusion of any single trial.
DISCUSSION
To our knowledge, this is the first investigation on the efficacy of DKT on intestinal dysfunction after abdominal surgery using meta-analysis of RCTs methodology. In our meta-analysis, DKT was associated with improving postoperative intestinal dysfunction by shortening the time to first postoperative flatus and bowel movement. This indicates that DKT has benefits and should be available as an approach for patients with postoperative intestinal dysfunction.
The principal finding of our meta-analysis is of clinical value, to some extent. Previous clinical control studies have reported conflicting results, with some showing a decrease in the time to postoperative first flatus and bowel movement [9] and some others demonstrating no effect [14]. What is of note is that the number of participants included in these studies was small, for instance, only 15 per group in Yoshikawa 2012 [8], which makes it difficult to come to a solid conclusion. Obviously, the pooled analysis of RCTs was closer to the true intervention effect, which further reveals the advantage of meta-analysis methodology. Therefore, we used extensive inclusion criteria and included various operations with different characteristics to make the results more clinically useful and generalisable.
The current available evidence of our meta-analysis suggested that DKT can be effectively and safely used to improve intestinal dysfunction in patients after abdominal surgery. Moreover, regardless of difference, sensitivity analyses further confirmed the creditability of the pooled intervention effect in outcome of the time to first postoperative flatus. Laparoscopy surgery has many potential advantages in earlier gastrointestinal recovery and shorter hospital stays over conventional open surgery [2425]. However, the results of sensitivity analysis for type of surgery showed that studies of open surgery showed significant decreases in the time to first postoperative flatus and the time to first postoperative bowel movement. Inclusion studies of colectomy showed a significant decrease in the time to first postoperative flatus and a decreasing trend in the time to postoperative bowel movement. After carefully checking, we found that the number of studies enrolled was very small (2 RCTs), and the results may have been influenced by potential biases. Therefore, further studies should focus on large, well-designed RCTs that focus on this issue.
There is accumulating evidence of DKT providing an important contribution in improving intestinal dysfunction [7891215]. Mechanisms underlying this beneficial effect are not fully understood and are most likely multifactorial. The effects of DKT on intestinal transit or motility might be mediated by cholinergic and 5-hydroxytryptamine mechanisms, as demonstrated by experiments finding that DKT was effective against morphine/chlorpromazine-induced intestinal disorders in rodents [26]. It has been demonstrated that DKT has the ability to reduce inflammatory reaction mediated by alpha7 nicotinic acetylcholine receptors activation [27], inhibit cyclooxygenase-2 activity [28], increase the intestinal blood flow through calcitonin gene-related peptide levels [629], and reverse bacterial translocation [30]. The current understanding of DKT in patients with intestinal dysfunction remains incomplete and well-designed studies are required further.
DKT is one of the most widely administered herbal medicines in Japan, and is mainly used for patients with postoperative ileus. Apparently, this compound is often used in Asia-Pacific countries but not in the West. However, it has been approved by the U.S. Food and Drug Administration as an investigational drug in the United States [12]. Moreover, several clinical trials have been launched to investigate its efficacy for Crohn disease, irritable bowel syndrome, and constipation [15]. DKT is a pharmaceutical-grade extract, which is under strict quality-control criteria, comparable with western pharmaceutical drugs in terms of therapeutic strength. It is expected that DKT will be more acceptable to patients and doctors in future clinical practice.
Several limitations should be taken into account. First, we confirmed the efficacy of DKT, but we included a variety of surgeries and different surgical approaches with inherent clinical and methodological heterogeneity, which may be restricted in some specific types of surgeries and thereby have an impact on our results. For example, pancreaticoduodenectomy is a multi-organ operative procedure with a high incidence of morbidity. Thus, further individual participant data meta-analysis focusing on more homogeneous clinical situations should be conducted. In our present meta-analysis, we made a pragmatic decision that to combine all kinds of surgeries reporting DKT use would be more generalisable to clinical practice than to group specific types. In addition, to mitigate heterogeneity, we used the random-effects model. Second, the current meta-analysis confirmed the effectiveness of DKT on improvement of postoperative intestinal dysfunction, but the dosage, the method, and the duration of administration varied in the included studies. Actually, the optimum DKT dosage, the method of administration, and the duration associated with DKT products are unclear. Accordingly, further studies are warranted to explore this optimization. Finally, the present meta-analysis is based on limited studies.
In summary, our meta-analysis is of clinical significance. The current available results show that DKT can significantly shorten the time to first postoperative flatus and time to first postoperative bowel movement, and improve intestinal dysfunction after abdominal surgery. However, it should be interpreted with caution, because of the significant heterogeneity of the studies. Thus, the efficacy of DKT on improving postoperative intestinal dysfunction warrants further investigation.
 XML Download
XML Download