

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Discrepancies between clinical symptoms, radiographic findings, and operative findings for temporomandibular joint (TMJ) disorders sometimes confuse clinicians. For this reason, many studies have tried to discover markers of TMJ disorders with resected tissue or molecules in synovial fluid and cartilage to make accurate diagnoses.
Disc tissue is adaptable to loading and this adaptation results in consequent disc remodeling. It has been reported that articular disc and bony changes are related to various kinds of extracellular matrix and expression of certain enzymes1. Matrix metalloproteinase (MMP) affects progress of TMJ disorders and also serves as a crucial indicator of early stage degenerative joint changes. It has been demonstrated that MMPs and their inhibitors are involved in both physiological and pathological conditions in rabbit study2. In human studies, MMP-1, 2, 3, 9, and 13 have been detected in the synovial fluid of osteoarthritis (OA) patients3456, and expression and concentration of MMP-2, 3, and 9 increased in synovial fluid of patients with internal derangement (ID) or OA47. Therefore, it can be suggested that upregulation of MMP-1, 2, 3, 8, 9, and 13 in the synovial fluid from TMJ ID or in OA patients means pathological degradation and destruction of TMJ tissue8.
The MMP family contains the only mammalian proteinases known as ‘collagenases’. The ‘classical’ collagenases-1, 2, and 3 (MMP-1, 8, 13) are specific for certain collagens. Collagenases can affect matrix changes in the retrodiscal tissue which is composed of collagen type I and II. Meanwhile, activated MMPs are mainly regulated by tissue inhibitor of metalloproteinase (TIMP), classified as TIMP-1, 2, 3, and 4. Among TIMPs, TIMP-1 resists collagenase, stromelysin, and gelatinase.
The retrodiscal tissue from TMJ disorder patients who underwent TMJ surgery usually shows fibrous degeneration, congestion, adhesion, or perforation. But because of difficulties in subject selection, current studies are insufficient to find out extracellular matrix-related factors for these changes. Therefore in this study, MMP-1, 8, 13 and TIMP-1 expression were investigated from retrodiscal tissue sections obtained during TMJ open surgery. To understand the relationship between expression of these enzymes and TMJ structural changes, immunohistochemical findings, magnetic resonance imaging (MRI), and operative findings were analyzed.
II. Materials and Methods
1. Materials
This study was conducted on 39 TMJs of 39 patients who had undergone discoplasty or discectomy. Patients were diagnosed as ID or OA based upon clinical examination and MRI at the Department of Oral and Maxillofacial Surgery at Gangnam Severance Hospital (Seoul, Korea).
The wedge-shaped sample was obtained from the lateral side of retrodiscal tissue during discoplasty. During discectomy, tissue samples were obtained from both articular disc and retrodiscal tissue.
2. Methods
1) Immunohistochemistry
Each 5 µm-thick tissue section, which had been fixed in 10% neutral-buffered formalin and embedded in paraffin, was placed on a silanized slide. Sections were deparaffinized with xylene and soaked in ethanol. The sections were incubated in 3% hydrogen peroxide for 10 minutes to quench endogenous peroxidase activity and washed with Tris-buffered saline (TBS). After blocking the binding of nonspecific protein using serum blocking solution for ten minutes, sections were incubated with a primary antibody, diluted 1:50, for an hour at room temperature. Each MMP-1 antibody (EP1247Y; Abcam, Cambridge, UK) and MMP-8 antibody (EP1252Y; Abcam) were rabbit monoclonal to origins with synthetic peptide corresponding to residues in human MMP-1 or MMP-8. MMP-13 antibody (Abcam) was a rabbit polyclonal to MMP-13 human recombinant MMP-13 protein. TIMP-1 antibody (102D1; Abcam) was a mouse monoclonal origin from which BALB/C mice injected with recombinant human TIMP-1.
After washing in TBS, sections were incubated with a biotinylated secondary antibody for ten minutes at room temperature and rinsed. Then, they were rewashed after ten minutes of incubation with streptavidin-peroxidase at room temperature. In the above process, Histostain-plus kit (Zymed, Camarillo, CA, USA) was used. Finally they were colorized by diaminobenzidine tetrahydrochloride (DAB), counter-stained with Meyer's hematoxylin, and sealed with glycerol.
2) Evaluation of immunohistochemical staining
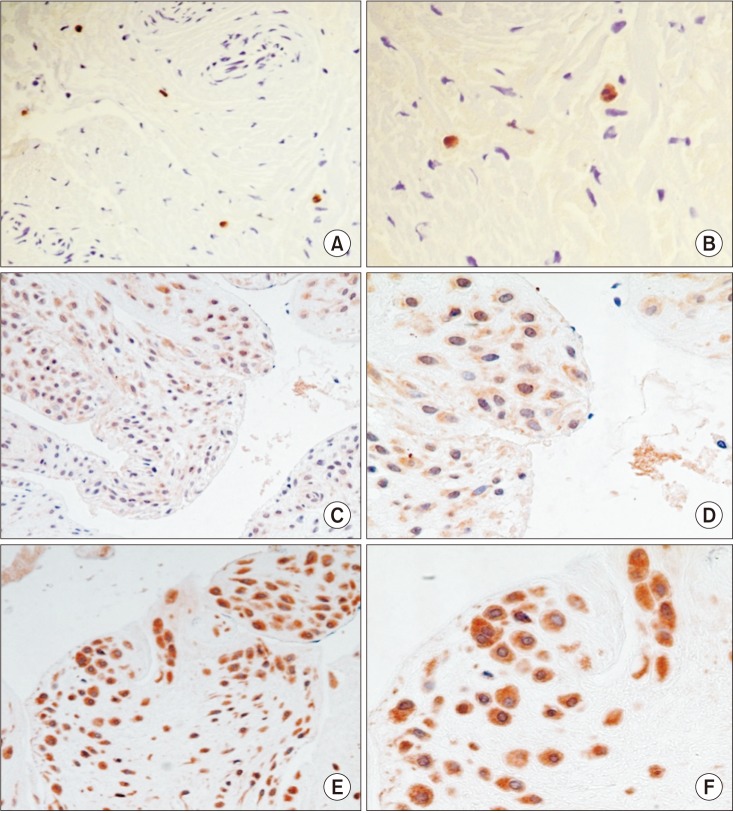
Staining patterns were classified into three grades according to expression levels of MMP-1, 8, 13 and TIMP-1. Those with diffuse expression less than 20 cells were classified as grade I; multiple group expression from 20 to 100 cells, grade II; and positive expression more than 100 cells, grade III.(Fig. 1)
3) Analysis of magnetic resonance imaging findings
MRI findings for ID were classified into four groups—normal position, disc displacement with reduction (DDcR), early stage of disc displacement without reduction (EDDsR), and late stage of disc displacement without reduction (LDDsR), based upon the position and status of joint disc on T-1 weighted MRI9.
(1) Normal: The disc is biconcave with the posterior band lying over the condyle, and the central thin zone is located between the condyle and the posterior part of the articular eminence.
(2) DDcR: When the jaw closes, the disc displaces anteriorly, anterolaterally, or anteromedially. But when the jaw opens, the disc is reduced to normal position.
(3) EDDsR: The disc displaced relative to the condylar head, regardless of jaw position. Disc slightly thickens at its posterior edge or begins to be deformed anatomically. When the jaw closes, the disc displaces slightly forward. When the jaw opens, disc deformity is observed.
(4) LDDsR: The disc displacement is similar to EDDsR, and also significant anatomical disc deformity is seen such as spectacles shape or amorphous form. When the jaw opens, the disc follows anterior movement of the condyle without anatomical deformity.
The diagnosis of degenerative joint depended on whether a patient has OA which includes erosion of mandibular condyle or condylar fossa, sclerosis, or absorption of cortical bone and signal change of bone marrow. The diagnostic criteria of OA on MRI are as follows:
(1) Normal bony structure
(2) Mild stage of OA
(3) Severe stage of OA
MRI findings for joint effusion were classified into level 0, 1, 2, or 3 based upon the amount of fluid collection or signal intensity on T-2 weighted MRI9.
(1) Level 0: No evidence of high signal intensity in the joint space
(2) Level 1: Fluid collection is seen in the boundary of temporal bone and disc or high signal intensity is visible within the folded disc
(3) Level 2: High signal intensity is visible in the anterior recess of upper or lower joint space. It extends outside the boundary of the disc
(4) Level 3: High signal intensity is seen in the whole region of the upper or lower joint space
4) Analysis of operative findings
The patients were categorized into four groups. The first group showed no signs of adhesion or perforation. The second group showed partial or entire adhesion of the articular disc or the retrodiscal tissue to the condylar eminence or fossa. The third group showed perforation with upper joint cavity connected to the lower joint cavity. The fourth group showed both adhesion and perforation.
5) Statistical analysis
Data analysis was performed by chi-square test and Fisher's exact test of cross tabulation analysis using IBM SPSS Statistics ver. 12.0 for Windows (SPSS Inc., Chicago, IL, USA).
This study was conducted with approval from the Institutional Review Board at Yonsei University Gangnam Severance Hospital (IRB no. 3-2015-0076) and in compliance with the Declaration of Helsinki.
III. Results
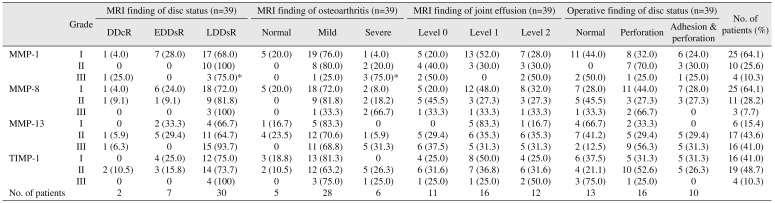
Three males (7.7%) and 36 females (92.3%) were included in the present study with the average of age 33 years (range, 21–70 years). Twenty-eight patients underwent discoplasty while the other 11 underwent discectomy. The expression levels of MMPs and TIMP-1 are shown in Table 1. MMP-1 and MMP-8 were expressed in all cases, and 64% of cases showed grade I expression. MMP-13 was expressed in all cases; however, 44% and 41% of cases showed grade II and III expression.
1. Comparison with MRI findings
Normal positioned disc was absent in this study and 2, 7, and 30 joints were diagnosed as DDcR, EDDsR, and LDDsR respectively based on MRI. In MMP-13 expression, 86.7% of the LDDsR group showed grade II or III. With more severe disc derangement status, more frequent MMPs and TIMP-1 expression was observed.(Table 1)
With regard to OA, 5, 28, and 6 joints were categorized as normal, mild, and severe stage respectively. Interestingly, in mild and severe OA stages MMP-13 grade II and III showed higher percentages. But among mild stage patients, grade I were dominant in other MMPs and TIMP-1.(Table 1)
In joint effusion, 11 cases were level 0, 16 cases were level 1, and 10 cases were level 2. Level 3 was not found in this research. There was not statistical significance in comparison between expression of MMPs or TIMP and joint effusion level.(Table 1)
2. Comparison with operative findings
In 13 cases, adhesion and perforation was not found. In 17 cases, only perforation was observed and in 10 cases both adhesion and perforation were observed. There were no cases of only adhesion in this research. In perforation and/or adhesion groups, all patients showed grade II or III MMP-13 expression. Once perforation occurred, expression of MMP-13 was increased with statistical significance.(Table 1)
IV. Discussion
MMP is an endogenous proteinase whose activity depends on Zn2. It plays an important role in degeneration of all kinds of collagen, proteoglycan, extracellular matrix, and particularly cartilage. It also contributes to breakdown of basement membrane and metabolism of normal matrix tissue10. MMPs are classified by their function into five groups including interstitial collagenases (MMP-1, 8, 13), gelatinases (MMP-2, 9), stromelysins (MMP-3, 10), membrane-type MMPs, and other MMPs.
Activated MMPs can be inhibited by a common proteinase inhibitor such as α2-macroglobulin, but are mainly inhibited by TIMPs as the chief endogenous MMP regulator, classified as TIMP-1, 2, 3, and 4. Among them, TIMP-1 is produced by most connective tissue cells and macrophages, and it resists against collagenase, stromelysin, and gelatinase.
The combination of extracellular matrix, including collagen, relieves pressure and tensile force put on joints. However, once these forces start to hurt articular cells, various kinds of degenerative enzymes are secreted and degrade connective tissue. Thus, to detecting TMJ disorders, some studies on synovial fluid have been conducted with the hypothesis that damaged extracellular matrix and degenerative enzymes will be released into the synovial fluid in TMJ disorder patients. These studies already have suggested involvement of MMPs in TMJ disease by increased MMP-13 levels in synovial fluid from patients with ID11. Since most human studies have been carried out using synovial fluid, the production site of these enzymes has never been investigated in degenerated disc tissue. The purpose of this study was to identify MMPs and TIMP-1 immunoreactive patterns with retrodiscal tissue samples obtained during surgery. This study also evaluated the association between these enzymes from retrodiscal tissue and the state of TMJ such as ID, OA, adhesion or perforation of disc.
Collagenase-1 (MMP-1) is produced and immediately secreted from some mesenchymal cells in response to specific inducers12,13. In contrast, collagenase-2 (MMP-8) is primarily produced by neutrophils during their maturation in bone marrow, and it is then stored until the cells are stimulated to degranulate12,13. Collagenase-3 (MMP-13) is found in bone, normal and pathologic cartilage, and various epithelial cancers, and it is the predominant collagenase in mice and rats while collagenase-1 is undetectable in these species13141516. Although each mammalian collagenase can degrade all fibrillar collagens, the preferred substrates for collagenases 1, 2 and 3 are collagens type III, I and II respectively 1718. Gepstein et al.19 reported it has been established that although individual enzymes have similar substrate specificities, their expression pattern is often distinct and characteristic in a certain tissue and cell type. In this study, all cases showed MMP-1, 813 and TIMP-1 expression but the range or cell type of expression were different. MMP-13, so-called ‘osteoblast collagenase’, demonstrated high expression grade generally. With more expression of MMP-13, there was more degenerative ID or OA extent. This could verify the importance of collagen type II in retrodiscal tissue as well as articular cartilage of TMJ. As specificity of collagenases, MMP-1 called ‘fibroblast collagenase’ was expressed on fibroblast and MMP-8 called ‘neutrophil collagenase’ was expressed on neutrophils. The expression site and level of each collagenase showed diversity.
Some conflicting results could be explained partially by differences in the sensitivity of the assays used for detecting MMPs and TIMPs such as immunohistochemistry, in situ hybridization, zymography, western blots, and northern blots. One study reported that different results can be related to detected location of MMPs that isolated chondrocytes, synovial fluids, cultured explants, or intact cartilages20. Huh et al.21 reported that they found MMP-1 mRNA from seven out of eight joints with OA and suggested that MMP-1 from retrodiscal tissue can play a role in destruction of cartilage and bone structure in TMJ. Another study showed that MMP-1 is active in synovial fluid of patients with pain in most cases and that a high concentration of MMP-1 can increase joint inflammation22. As mentioned above, the role of MMP-1 is not yet clear; however, it can be suggested that MMP-1 is involved in disc displacement or other related diseases because collagen is a major component of the retrodiscal tissue. In this study, 5/6 cases in the severe OA group expressed grade II and III MMP-1 expression and it also suggested that MMP-1 is associated with destruction of bone and cartilage of TMJ even with the small experimental group. But the character of MMP-8 expression was unclear in comparison with ID, OA, and surgical findings.
Among MMPs, MMP-13 (collagenase-3) appears to play a key role in joint connective tissue remodeling. MMP-13 can cleave type II collagen 10 times faster than MMP-1. MMP-13 expression has also been demonstrated in articular cartilage in OA patients and in synovium of rheumatoid arthritis patients. In this study, control disc cells were rarely immunopositive for MMP-13, although a few scattered fibroblast-like cells showed faint positive immunoreactions. MMP-13 was upregulated in TMJ disc tissue from IDs patients. One study also reported that MMP-13 immunolabelling increased with TMJ disc degeneration. Thus MMP-13 has been thought to play an active role in the synthesis of ECM-degrading proteinases23. In this study, with more MMP-13 in retrodiscal tissue, there was more degenerative ID or OA. The particularly severe OA group showed clear expression as grade II or III and this can explain that MMP-13 as well as MMP-1 is related with OA of TMJ. In comparison of MMP-13 expression with the position and status of articular disc, 86.7% of a group of LDDsR showed grade II or III, which means that breakdown enzymes involved in articular disc degeneration become more active as ID progresses. The case of grade III expression with DDsR in MRI was an OA patient who went through discectomy due to severe adhesion and perforation of articular disc.
Marchetti et al.'s study 24 demonstrated that structural modifications of articular disc could be specific responses to functional change of TMJ and variations in extrinsic stimuli may activate intrinsic factors, such as MMPs, that induce structural modifications in discal tissue. The examination found that only the areas with myxoid change or hyalinization were stained or these areas resulted in much more staining than others, and that cell numbers increased in areas with myxoid change. Such differences appeared when the retrodiscal tissue deteriorated or responded to passed-on loading caused by articular disc displacement, which suggests an association with MMPs.
In normal physiological processes, MMP activity is controlled at several levels. Loss of control of MMP activity appears to have serious consequences, and aberrations in MMP expression have been associated with several diseases. Though there is no general awareness of the expression of TIMP-1 in osteoarthritic cartilage and synovium, it is thought that TIMP-1 correlates with the production of MMPs25. It has been reported that there is a correlation between the concentration of TIMP-1 and MMP-1, and the imbalance between them in the progression of OA results in unrecoverable degradation of cartilage matrix26. During OA, the production of TIMP-1 is correlated to the level of MMPs. Their imbalance in the progression of OA may lead to the destruction of cartilage27. Whereas overexpression of collagenage-1, coupled with decreased production of TIMP-1, may impair healing, insufficient proteinase activity may lead to accumulation of wound-associated tissue and delays in wound closure. Thus, the properly regulated, site-specific expression of collagenase, as well as other MMPs, may be needed to promote efficient wound repair13. This study shows lower expression of TIMP-1 than MMPs, because it might be that the experimental groups were patients with TMJ disorder. Four cases of grade III expression of TIMP-1 was applied to LDDsR and mild or severe stage of OA. TIMP-1 expression seemed to affect ID in comparison with OA results, but it was not significant. Nevertheless our study assumes that TIMP-1 can be active if MMP expression pattern fits into grade II or III without any change or destruction in joint structures.
The imbalance between MMP-1 and TIMP-1 also plays an important role in the degradation of extracellular matrix28. This imbalance and reduced expression of TIMP-1, which suppresses the degradation of extracellular matrix, can explain aggressive patterns against bone or cartilage. Follow-up surveys on OA-related symptoms among TMJ disorder, including interactions of MMP-1, 13 and TIMP-1, are required for clinical applications.
This study was aimed to observe how collagenases (MMP-1, 8, 13) and TIMP-1 are expressed in immunohistochemistry of retrodiscal tissue sections in order to understand how their expression pattern is associated with ID, OA, joint effusion, and adhesion or perforation among TMJ disorder patients.
V. Conclusion
In conclusion, MMP-13 plays a critical role in degrading of OA as it is the predominant collagenase in collagen type II and can worsen ID as the collage breakdown enzyme of retrodiscal tissue in TMJ. MMP-1 is related to degeneration of OA. MMP-8 does not characterize specificity with regard to TMJ disorder. TIMP-1 seems to affect ID in comparison with OA expression, but it is not significant. In this study, the causal relation of the imbalance between MMP and TIMP could not be explained, but TIMP activity, which shows a difference with degeneration of TMJ disorders, suggests that TIMP should be considered in potential criteria for prevention of progressive disease via controlling collagenases.
 XML Download
XML Download