I. Introduction
The World Health Organization (WHO) recently classified the keratocystic odontogenic tumor (KOT), previously referred to as an odontogenic keratocyst (OKC), as a ‘tumor,’ and not as a cyst, because of its aggressive nature, high mitotic rate, and association with genetic and chromosomal abnormalities
1.
KOTs primarily occur in the areas of teeth that erupt in the mouth, or in the posterior site of the mandibular third molars. Most KOTs appear as separated, solitary lesions, but they can also appear as multiple cysts. According to previous studies on single lesions, KOT is predominant in males, and occurs in people as young or younger than 20 years, with a recurrence rate of 3% to 60%
234. However, few studies investigated KOTs with multiple lesions. In cases of KOTs with multiple lesions, tumor involvement in the jaws is greater, and if the tumors are left untreated, a patient with multiple lesions may have higher risks of morbidity compared to someone with a single lesion. Therefore, it is necessary to determine: 1) the number of lesions per patient; 2) whether there is a difference between single lesion KOTs and multiple lesions; and 3) the postoperative recurrence rate. As such, the goal of this study was to evaluate the clinical features of multiple KOT patients with respect to age, sex, prevalent sites, invasiveness, recurrence, treatment, prognosis, and relevance with systemic syndromes.
II. Materials and Methods
Patients in this study were those with a confirmed diagnosis of KOT through biopsy, and those who underwent surgery with an estimated diagnosis of multiple KOTs on two or more surgical sites. Patient data was obtained from the records of the Department of Oral and Maxillofacial Surgery in the Pusan National University Hospital, and from the Pusan National University Dental Hospital, for approximately 11 years and 3 months (from January 1, 2005 to March 31, 2016). All histologic diagnosis titles were acknowledged as KOT, and not OKC, by the Department of Pathology, following the recent classification decision of WHO.
The patients and specific surgical sites were retrospectively analyzed based on patient medical records, radiographs, and biopsy results. The analyses were based on various perspectives, including sex and age, lesion site, operative methods, number of operations per patient, recurrence rates, recurrence sites, and tendency and association with unerupted or impacted teeth. When counting the number of multiple lesions, a follicular space with a diameter of 3 mm or more was determined as one cystic lesion. Data are shown as mean±standard deviation, and differences between the groups were determined with a two-tailed Student's t-test to calculate the P-values, and P<0.05 was considered statistically significant. All analyses were performed by using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA).
This study was approved by the Institutional Review Board of the Pusan National University Dental Hospital (PNUDH-2017-019).
IV. Discussion
KOT usually occurs as a single lesion, although it can also occur as multiple lesions. In a study conducted by González-Alva et al.
5, 24 patients had multiple KOTs from a total of 183 KOT cases. Therefore, we examined the characteristics of KOTs that appeared in multiple lesions in this study.
KOT is generally known to occur in young individuals. According to Myoung et al.
6, the most frequent occurrence was noted in individuals aged 30 years or less. According to Chirapathomsakul et al.
7, as in most other studies, KOT was most prevalent at 11 to 40 years of age. Chirapathomsakul et al.
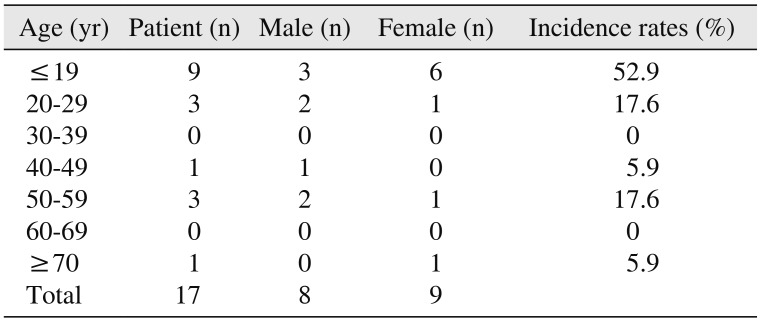
7 reported that men and women were almost equal in incidence, although some studies found a higher occurrence in males. This study revealed similar results. There was no definite correlation between gender and multiple KOTs, although was significantly prevalence in teenagers. The patients' mean ages were 28.4±20.1.(
Table 1)
Table 1
Multiple keratocystic odontogenic tumor (KOT) patients by sex and age
|
Age (yr) |
Patient (n) |
Male (n) |
Female (n) |
Incidence rates (%) |
|
≤19 |
9 |
3 |
6 |
52.9 |
|
20–29 |
3 |
2 |
1 |
17.6 |
|
30–39 |
0 |
0 |
0 |
0 |
|
40–49 |
1 |
1 |
0 |
5.9 |
|
50–59 |
3 |
2 |
1 |
17.6 |
|
60–69 |
0 |
0 |
0 |
0 |
|
≥70 |
1 |
0 |
1 |
5.9 |
|
Total |
17 |
8 |
9 |
|

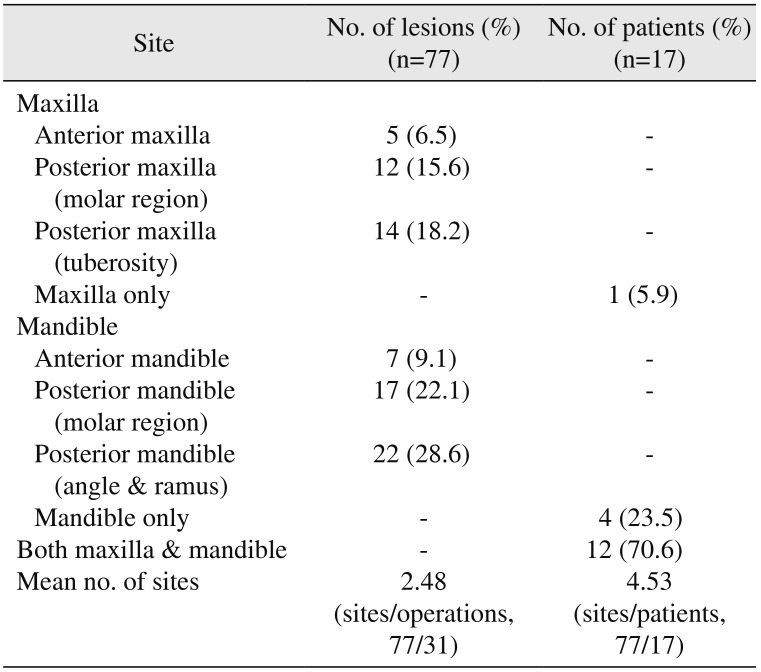
KOT is more prevalent in the mandible than in the maxilla, with a large number of sites occurring in the posterior body and ascending ramus. Previous studies found that KOT had a marked tendency to involve the posterior body and the ascending ramus of the mandible, with a 49% rate of incidence
89, which was similar to the results of the this study. The most prevalent site was the mandibular posterior area. In the present site, the molar region and angle, as well as the ramus of the mandible, accounted for 50.6% (39 of 77 sites) of the total sites.(
Table 2)
Table 2
Analysis of lesion occurrence sites
|
Site |
No. of lesions (%) (n=77) |
No. of patients (%) (n=17) |
|
Maxilla |
|
|
|
Anterior maxilla |
5 (6.5) |
- |
|
Posterior maxilla (molar region) |
12 (15.6) |
- |
|
Posterior maxilla (tuberosity) |
14 (18.2) |
- |
|
Maxilla only |
- |
1 (5.9) |
|
Mandible |
|
|
|
Anterior mandible |
7 (9.1) |
- |
|
Posterior mandible (molar region) |
17 (22.1) |
- |
|
Posterior mandible (angle & ramus) |
22 (28.6) |
- |
|
Mandible only |
- |
4 (23.5) |
|
Both maxilla & mandible |
- |
12 (70.6) |
|
Mean no. of sites |
2.48 (sites/operations, 77/31) |
4.53 (sites/patients, 77/17) |
Between the maxilla and the mandible, the mandible was a more common site of multiple KOTs. However, the most popular types were lesions in both the maxilla and the mandible (
Table 2), which were similar to the results of a previous study conducted by Chirapathomsakul et al.
7, which reported significantly more multilocular lesions in the mandible as opposed to the maxilla.
Almost all of the operations were enucleations, except for one case of marsupialization (
Table 3), although this particular case changed to enucleation during treatment. According to a systematic review by Blanas et al.
10, the recurrence rate of KOT was 17% to 56% when only simple enucleation was performed. However, according to the systematic review of 997 KOT lesions by Al-Moraissi et al.
11 that was based on 14 articles, the recurrence rates were 18.2% for enucleation and 27.1% for decompression; accordingly, enucleation was considered to be more useful in preventing the recurrence of KOT, and should be chosen if possible.
Table 3
Treatment methods

|
Enucleation |
Marsupialization |
|
No. of patients |
16 |
1 |
KOT has a thin and weak wall, and is usually accompanied by a daughter cyst. Therefore, it is not easy to completely remove a KOT with a simple enucleation
12. However, enucleation is currently the most common surgical method
131415. To lessen the recurrence rate, we should consider additional surgical methods after enucleation, such as cautery with chemicals (e.g., Carnoy's solution), or cryotherapy and peripheral ostectomy by using a round bur
1516.
Resection with a safety margin could be another alternative. However, Blanas et al.
10 reported a problem with high morbidity when this method was used, despite the recurrence rate of 0%. Also, it was not commonly accepted by patients and surgeons because of its benign nature.
To measure recurrence rates, we should differentiate purely recurred lesions from secondary lesions. Secondary lesions come from other sites not associated with a previous operation site. Purely recurred lesions are lesions that actually recurred from a previous operation site. According to one study, the frequency of recurrence of KOT in various studies ranges from 5% to 62%
9. Chirapathomsakul et al.
7 reported a KOT recurrence rate of 22.6%, while Myoung et al.
6 reported 58.3%. Moreover, Myoung et al.
6 reported a total of 11.7% of patients experienced two or more recurrences. Then, when an oral cavity was divided into six parts by region, the recurrence rate was high in the mandibular posterior part. Finally, González-Alva et al.
5 found a recurrence rate of 13.1%.
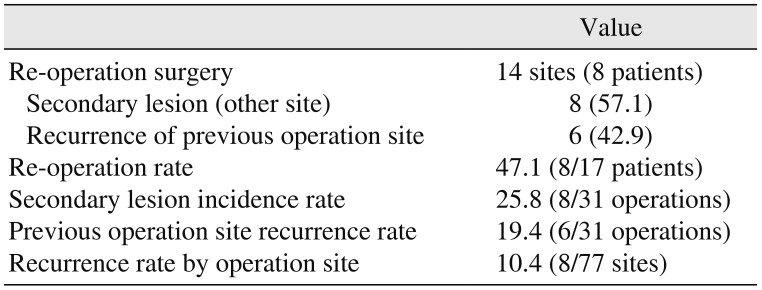
In this study, the recurrence rate was 10.4% (8 of 77 sites), and the rate of re-operation on one patient was 47.1%.(
Table 4,
Fig. 1) The recurrence rate may vary by calculation because it will be based on either one patient or each lesion. Therefore, a simple comparison with other studies might be difficult, although such a study could be useful. Jo et al.
17 reported that patients with multiple lesions showed a higher recurrence rate than patients with single lesions.
Fig. 1
Frequency of operations for each patient. Patients had an average of 1.82 operations, including surgeries due to recurrence. One patient had four operations, which was the maximum number of operations per person.
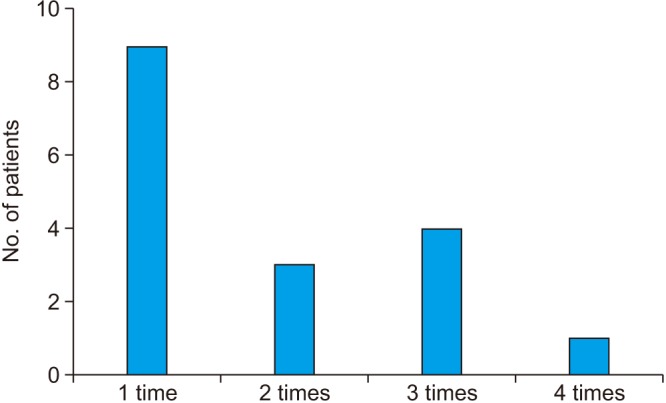

Table 4
Recurrence tendency and rate
|
Value |
|
Re-operation surgery |
14 sites (8 patients) |
|
Secondary lesion (other site) |
8 (57.1) |
|
Recurrence of previous operation site |
6 (42.9) |
|
Re-operation rate |
47.1 (8/17 patients) |
|
Secondary lesion incidence rate |
25.8 (8/31 operations) |
|
Previous operation site recurrence rate |
19.4 (6/31 operations) |
|
Recurrence rate by operation site |
10.4 (8/77 sites) |
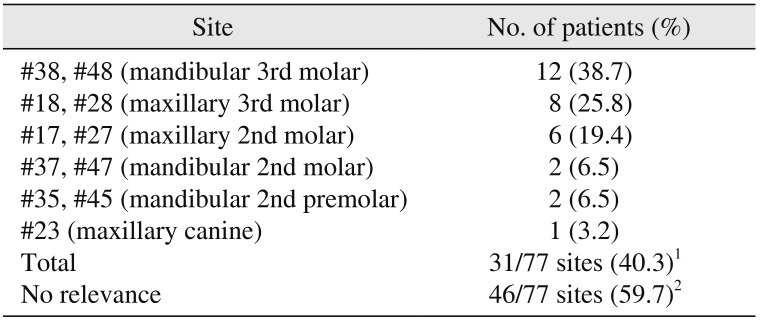
The lesions associated with the unerupted or impacted teeth were present in 31 sites with a rate of 40.3%. Of the 17 patients, 9 patients (52.9%) were identified as having KOT lesions associated with embedded teeth.(
Table 5,
Supplementary Table 1) In one study, 25% to 40% of cases involved unerupted teeth
9. Chirapathomsakul et al.
7 reported that the proportion of lesions related to teeth was 33%, which was higher compared to other studies
81819.
Table 5
Association with unerupted and impacted teeth
|
Site |
No. of patients (%) |
|
#38, #48 (mandibular 3rd molar) |
12 (38.7) |
|
#18, #28 (maxillary 3rd molar) |
8 (25.8) |
|
#17, #27 (maxillary 2nd molar) |
6 (19.4) |
|
#37, #47 (mandibular 2nd molar) |
2 (6.5) |
|
#35, #45 (mandibular 2nd premolar) |
2 (6.5) |
|
#23 (maxillary canine) |
1 (3.2) |
|
Total |
31/77 sites (40.3)1
|
|
No relevance |
46/77 sites (59.7)2
|
Multiple KOTs are frequently associated with NBCCS. Epidermal cysts of the skin, palmar/plantar pits, calcified falx cerebri, enlarged head circumference, rib anomalies (e.g., bifid rib), and OKCs are major clinical features of the NBCCS
920. Basal budding, which is common in KOTs associated with NBCCS, was found in the histological finding of one patient, but there were no definite patients with syndromic signs in this study. Other studies also showed a low association with the syndrome. Indeed, according to González-Alva et al.
5, only 6.0% of patients were clinically related to NBCCS.


 PDF
PDF ePub
ePub Citation
Citation Print
Print



 XML Download
XML Download