

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Renal dysfunction is common in candidates for liver transplantation (LT) and is observed in 15%–25% of patients [123]. Renal replacement therapy (RRT) was performed in the patients with refractory renal dysfunction, to manage uncontrolled metabolic acidosis, electrolyte imbalance, volume overload, and brain edema. The patients with hemodynamic instability were managed with continuous renal replacement therapy (CRRT) [2].
Since LT may cause massive bleeding and require a large amount of volume resuscitation, many clinicians worry about hemodynamic and metabolic instability during LT in patients with severe preoperative renal dysfunction. Although there have not been definite criteria for initiating intraoperative RRT, many institutions have performed intraoperative RRT in recipients with severe preoperative renal dysfunction to prevent critical uremic complications and to facilitate fluid management. Studies and cases r eporting successful management of intraoperative RRT during LT have been reported [456].
However, despite the proposed benefits of intraoperative RRT, it carries additional risks, such as exposure to an extracorporeal circuit, need for anticoagulation, and added costs [57]. Meanwhile, we have experienced that the balance of acid-base, electrolytes, and body fluid can be well maintained through regular laboratory test and careful hemodynamic monitoring during LT without intraoperative CRRT. Because there is no firm evidence to support this practice, our institution has not been using intraoperative RRT during LT. Accordingly, we described our institutional experience and clinical outcomes for recipients with severe preoperative renal function and were managed without intraoperative RRT. The aim of this study was to show that intraoperative CRRT was unnecessary for LT recipients with severe renal failure.
METHODS
After obtaining the approval from the Institutional Review Board of Samsung Medical Center (2015-11-027-002), we retrospectively investigated all adult patients (age ≥ 18 years) who received LT between December 2009 and May 2015. The recipients, who received preoperative CRRT until immediately before LT, because of refractory renal dysfunction, were enrolled. The recipients were excluded who discontinued preoperative CRRT more than 24 hours before LT because of improvement of renal function and who received simultaneous liver and kidney transplantation.
After anesthetic induction and endotracheal intubation, mechanical ventilation was initiated with a tidal volume of 8–10 mL/kg and an inspired oxygen fraction of 0.5. The inspiratory rate was adjusted to maintain normocapnia. Anesthesia was maintained using inhaled isoflurane and a continuous infusion of remifentanil (0–0.15 µg/kg/min) and the bispectral index (BIS) was used to monitor the depth of anesthesia. Two arterial pressures through the radial and femoral arteries and 2 venous pressures through the internal jugular and femoral vein were monitored. Cardiac output was measured using thermodilution or by analyzing the arterial waveform.
Regardless of the type of donor (living or deceased donor), all donor liver grafts were prepared using histidine-tryptophanketoglutarate solution. Anastomosis of the liver graft was performed with a piggyback technique without a venovenous bypass. After the portal vein anastomosis was performed, the reperfusion phase was initiated by the consecutive release of the hepatic and portal vein clamps. The hepatic artery and bile duct were anastomosed in succession. At the end of the surgery, all recipients were transported to an intensive care unit (ICU) for postoperative care.
Arterial blood was sampled every hour and additional samples were collected at the time of the anhepatic phase initiation, 5 and 30 minutes after reperfusion, to evaluate arterial blood gases (ABGs), electrolytes, hematocrit, glucose, and lactate, throughout surgery. Crystalloid, colloid, and blood products were administered according to the central venous pressure (CVP) and laboratory values. If autologous blood from a cell salvage device was collected, 300 mL of autologous blood was transfused when the hemoglobin (Hb) was < 9.0 g/dL. When the Hb was < 8.0 g/dL, 2 units of leukocyte-deleted packed red blood cell (pRBC) were transfused. Two units of fresh frozen plasma (FFP) were transfused when the prothrombin time international normalized ratio was > 3. If platelet counts were < 30,000/µL, 6 units of platelet concentrate or one unit of single donor apheresis platelets was transfused. Six units of cryoprecipitate were transfused when the fibrinogen level was < 80 mg/dL.
Regular insulin (RI) 10 units were administered with 200 mL 5% dextrose solution when the serum potassium was > 4.5 mEq/L before reperfusion [89]. Sodium bicarbonate was infused when the base excess was < −10 mEq/L during surgery. If the mean blood pressure was < 70 mmHg, we performed the following steps in order. (1) Anesthetic depth was adjusted to maintain BIS values from 40 to 60. (2) Fluids and blood products were administered to maintain the CVP ≥ 5 mmHg. (3) Dopamine was added if cardiac contractility was decreased. (4) Norepinephrine was added up to 0.3 µg/kg/min. (5) Vasopressin and/or epinephrine was added. No protocols were changed during the study period.
We collected recipients' perioperative data from electronic medical records. Preoperative variables included patients' demographics, the use of CRRT, laboratory findings associated with kidney function, the model for end-stage liver disease (MELD) score [10], the Child-Turcotte-Pugh (CTP) score [11], and chest radiograph findings. All preoperative variables were based on the last data within one week before LT. Intraoperative variables included duration of anesthesia and operation, amount of crystalloid or colloid infused, and transfusion, as well as urine output and ascites. One unit of single donor apheresis platelets was counted as 6 units of platelet concentrates. Amount of blood loss was calculated based on the lost red cell mass because direct estimation was difficult [12]. Data on ABG values, dose of pressors (dopamine, norepinephrine, vasopressin, and epinephrine), amount of RI bolus administration due to potassium levels > 4.5 mEq/L before reperfusion, and amount of sodium bicarbonate infusion due to base excess < −10 mEq/L during surgery were collected. The dopamine, vasopressin, and epinephrine doses were converted to the norepinephrine equivalent dose [131415]. Then, the maximal norepinephrine equivalent dose was calculated as a sum of the dopamine, norepinephrine, vasopressin, and epinephrine doses. Postreperfusion syndrome was diagnosed when the mean arterial pressure was 30% lower than the previous value at the end of the anhepatic stage for at least 1 minute during the 5 minutes after reperfusion. Immediate postoperative variables were based on the first findings of laboratory values and chest radiograph after the recipients arrived at the ICU. The reading of chest radiograph was based on judgement of the authors and review of the radiologist. A critical arrhythmia was defined as new-onset atrial fibrillation, sustained ventricular tachycardia, or cardiac arrest. Postoperative clinical outcomes included lengths of stay in the hospital and the ICU, in addition to graft loss and mortality at postoperative 30-day and 1-year.
IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA) was used for statistical analysis. Categorical variables were presented as number and frequency. They were compared using chi-square test or Fisher exact test. Continuous variables showing normality were then analyzed using Student t-test and expressed as mean ± standard deviation (SD). Continuous variables not showing normality were then analyzed using Mann-Whitney test and expressed as median (interquartile range [IQR]). The recipients' survival rates after LT were calculated using the Kaplan-Meier method. All P-values were calculated using 2-tailed test. A P-value of less than 0.05 was considered statistically significant.
RESULTS
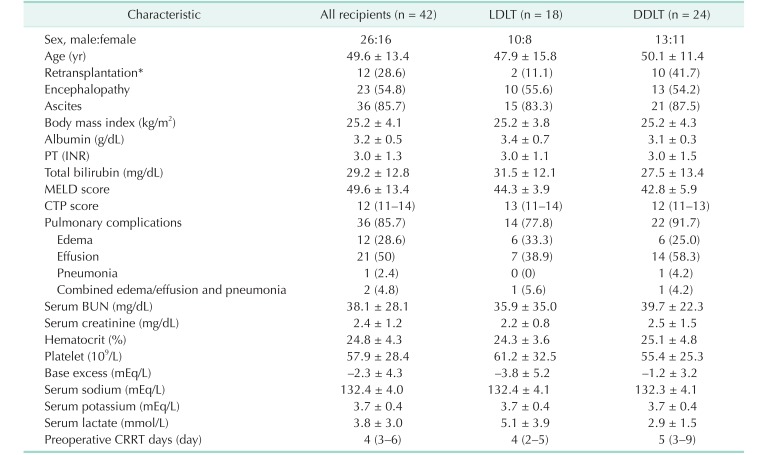
During the study period, 706 recipients of LT were screened. Of those, there were 42 adult recipients, who received CRRT until immediately before LT. The recipients' demographics and details of their preoperative status are described in Table 1. Seventy-six point two percent (76.2%, 32 of 42) of recipients had the MELD scores more than 40 and the mean MELD score (SD) were 49.6 (13.4). In pretransplant period, 83.3% of recipients already had pulmonary edema and effusion and 85.7% of recipients had uncontrolled ascites.
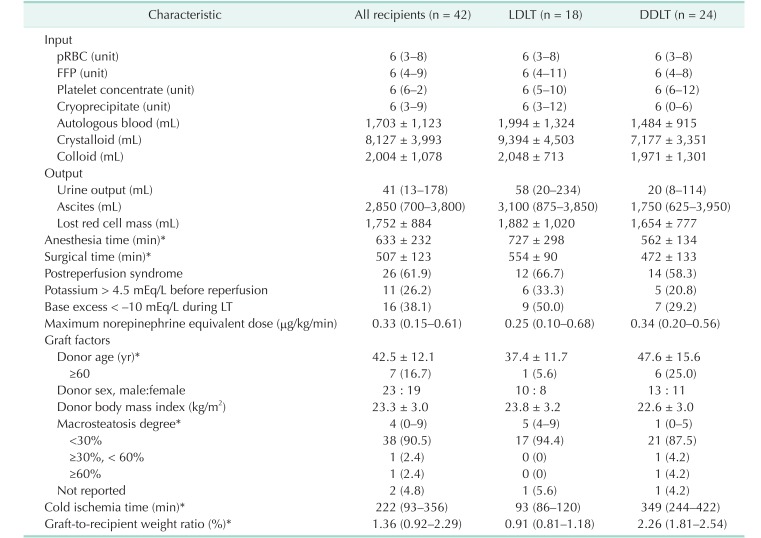
The intraoperative details during the LTs are described in Table 2. Median transfused blood products were 6 units in each blood product (pRBC, FFP, platelet concentrates, and cryoprecipitate). And autologous blood from cell salvage was used in most of recipients except three. Amount of mean blood loss calculated from the lost red cell mass was 1,752 mL. Considering that we targeted Hb 8.0 g/dL and hematocrit 24 %, the mean estimated blood loss was approximately 7,300 mL (1,752 × 100/24). While a large amount of blood loss occurred and transfusion was performed, the amount of median (IQR) urine output was 4.25 (10.45) mL/hr. Twenty-six point two percent (26.2%) of recipients used RI bolus, and 38.1% of recipients used sodium bicarbonate to control serum potassium levels (>4.5 mEq/L before reperfusion) and metabolic acidosis (base excess < −10 mEq/L throughout LT). There were no critical cardiac arrhythmias in all recipients.
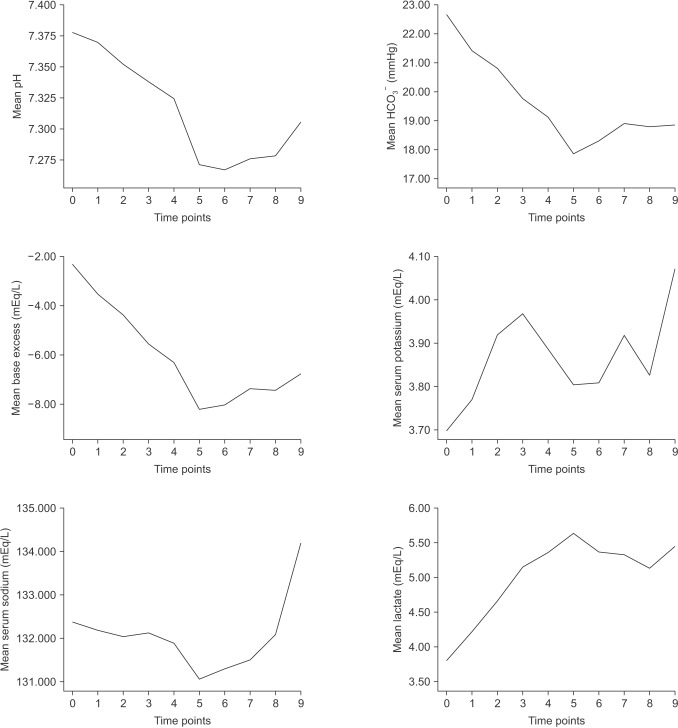
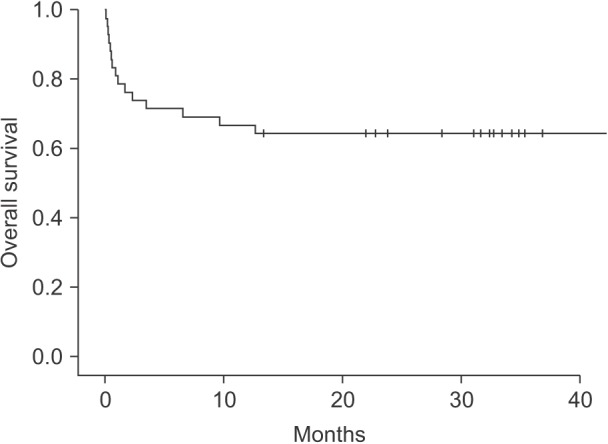
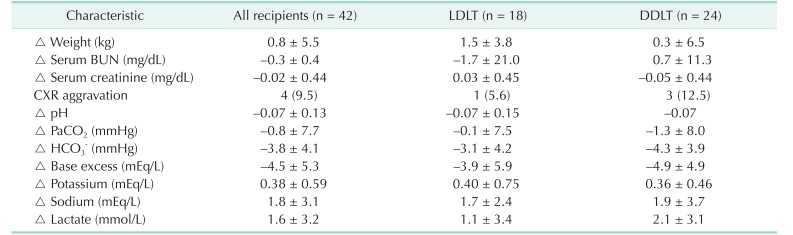
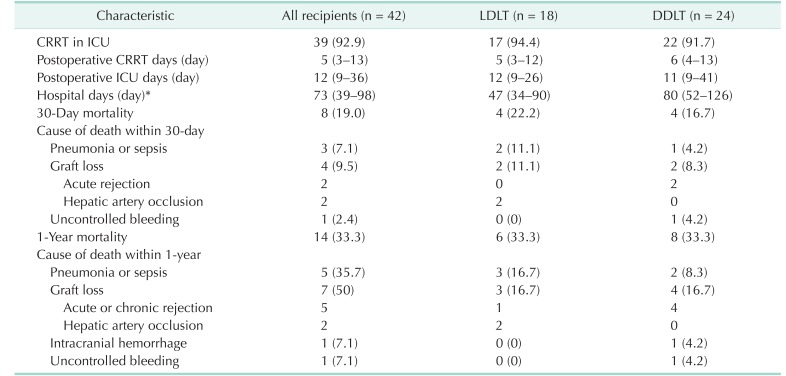
Differences of parameters between the beginning and the end of surgery are described in Table 3. There were no significant differences between living donor LT and deceased donor LT. Changes in laboratory values at each time point during LT are shown in Fig. 1. Postoperative outcomes are described in Table 4. In the majority of recipients, postoperative CRRT was routinely applied immediate after LT (92.9%). The postoperative 1-year mortality was 33.3% (Fig. 2).
DISCUSSION
In our retrospective analysis, we investigated the recipients of LT who had severe renal dysfunction supported with CRRT in the pretransplant period. However, all recipients were managed without intraoperative RRT. Our objectives were to evaluate expected adverse events associated with renal dysfunction in the intraoperative and immediate postoperative periods. We found that the recipients managed with preoperative CRRT had great preoperative severity of illness based on MELD and CTP scores, and showed a large amount of intraoperative bleeding and blood product requirements. However, serum potassium levels and metabolic acidosis were well controlled medically. In addition, pulmonary edema/effusion aggravation occurred in only 9.5%. No one developed severe hyperkalemia (serum potassium > 5.5 mEq/L) or critical arrhythmias, such as newonset atrial fibrillation, sustained ventricular tachycardia, and cardiac arrest during LT. All recipients finished their operations without uncontrolled complications.
Preoperative renal dysfunction is a common complication in patients with end-stage liver disease and it is associated with postoperative morbidity and mortality [1617]. The preoperative renal function is an important component in the MELD score and has now become the standard tool in liver allocation [10]. The common causes of renal dysfunction in recipients of LT are divided into 2 categories, prerenal azotemia and intrinsic renal disease [1]. Hepatorenal syndrome is a functional prerenal azotemia. Intrinsic renal disease includes acute tubular necrosis, acute interstitial nephritis, immunoglobulin A nephropathy, and others. Renal dysfunction can be promoted by systemic hypotension, antibiotics, intravenous contrast, or prolonged ischemia. In the LT candidates with severe renal dysfunction, complications such as acidosis, electrolyte derangement, and volume overloads can occur. Therefore, preoperative RRT is applied to the LT candidates with medically refractory renal dysfunction. Types of RRT are peritoneal dialysis, intermittent hemodialysis, CRRT, and sustained low-efficiency dialysis [2]. The LT candidates with hemodynamic instability were managed with CRRT to reduce complications associated with rapid correction [2].
Many clinicians have applied and utilized intraoperative RRT in recipients of LT with preoperative renal dysfunction because they were concerned about complications caused by uncontrolled metabolic acidosis, hyperkalemia, and volume overload, such as pulmonary or brain edema. Although many institutions have presented reports about the use of intraoperative RRT that focused on successful management and the safety of intraoperative RRT [456181920212223], there was no standardized indication for intraoperative RRT. Despite several benefits of intraoperative RRT, there are risks, including insertion of an additional large-caliber central venous catheter, exposure to an extracorporeal circuit, and intraoperative circuit disruption. Especially, because LT requires a lot of clinicians, intravascular lines, and equipment, it is helpful to simplify the environment as much as possible to reduce additional risks. Additionally, the use of systemic anticoagulation or regional citrate seems to be risky during LT, where a large amount of bleeding and blood transfusion is expected. The use of RRT itself may cause significant electrolyte derangements, hypotension, new onset arrhythmia, anemia, and thrombocytopenia. Furthermore, the need for additional consultants and machines adds costs [25723].
Based on our experience of successful management without intraoperative CRRT in early LT cases with severe renal failure, we consistently managed all recipients without intraoperative RRT during LT. We evaluated major complications associated with renal dysfunction, such as electrolyte derangement, acidosis, and volume overload. Nonetheless, even the recipients who needed pretransplant CRRT were managed successfully during LT without critical complications. Serum potassium was sufficiently controlled with only the use of RI without intraoperative RRT. During 5 minutes after reperfusion, which is high risk point of hyperkalemia, no one had hyperkalemia associated complications. Along with preemptive use of RI when serum potassium was > 4.5 mEq/L before reperfusion, the primary use of cell salvage blood prior to the use of banked blood, seemed to contribute to successful managing serum potassium, because the cell salvage blood had a lower serum potassium than the banked blood [2425]. Metabolic acidosis was controlled with sodium bicarbonate and mean systemic blood pressure was maintained at > 70 mmHg with pressors during LT. Intravascular volume was managed strictly according to our protocol. The signs of volume overload, such as pulmonary edema/effusion aggravation was occurred only 4 among 42 recipients (9.5%) and mean postoperative weight gain were within 1 kg. Compared with previous studies showing 4%–47% of post-liver transplant pulmonary edema [26272829], the incidence of pulmonary edema/effusion in our study was not high. During present study period there was one case of simultaneous liver and kidney transplantation. We also managed that case without intraoperative CRRT [30]. Interestingly, serum blood urea nitrogen and creatinine were lower immediate postoperative values than postinduction values. We cautiously theorize that a lot of blood volume exchange from a large amount of blood loss and volume resuscitation had a similar effect with hemodialysis.
We found 81% 30-day and 67% 1-year survival rate in our study. Recently, Agopian et al. [23] reported a study with 91% 30-day and 63% 1-year survival rate in 70 recipients who received preoperative CRRT or intermittent hemodialysis and intraoperative CRRT. Compared with study of Agopian et al. [23], our 30-day survival rate was lower while 1-year survival rate was comparable. However, our MELD score (mean, 49.6) was higher than that of study of Agopian et al. [23] (mean, 39). In addition, none of our recipients could not receive retransplantation due to lack of deceased donor although half of cause of death was graft loss (Table 4). It was contrasted to study of Agopian et al. [23] that more than 90% of recipients, who experienced graft loss within postoperative 30-day, received re-transplantation. Although several factors besides the chance of retransplantation were related with the outcomes such as recipient's condition and availability of living donor, the low retransplantation opportunity might affect our low 30-day survival rate. Considering death from lack of retransplantation opportunity and high preoperative MELD score, our survival rate seems comparable with previous studies.
There were several limitations to our study. First, this study was done at a single center and the sample size was relatively small. Second, we could not compare use and no use of intraoperative RRT in the patients receiving preoperative RRT because our institution did not use intraoperative RRT in all patients. Third, our study was limited to short-term follow-up except for survival analysis. Fourth, because we used the piggyback technique in all deceased donor LT, it might be difficult to generalize our results to other surgical methods. Fifth, we could not evaluate whether deceased donor was a marginal donor because we could not find the record of donor during ICU stays (dose of pressors and so on). However, we think our results are sufficient to raise a question as to whether or not intraoperative RRT is necessary in recipients of LT who have severe preoperative renal dysfunction.
In summary, we investigated the expected adverse events at the intraoperative and immediate postoperative periods in recipients of LT with severe preoperative renal dysfunction, when the recipients were managed without intraoperative RRT. Our results showed that LT was safely performed, even though intraoperative RRT was not used in patients who received preoperative RRT, because of severe preoperative renal dysfunction. Our finding raises a question about the need for intraoperative RRT and we recommend further well-designed trials.
 XML Download
XML Download