

 PDF
PDF ePub
ePub Citation
Citation Print
Print



PREFACE
Many efforts have been made to reach a higher accuracy in the tumor staging classifications (1). Tumor staging classifications demand to be constantly updated to latest clinical, anatomic, numeric criterion, pathological, molecular biology, genetics and biochemical findings in order to fulfill their function of internationally accepted standardization and comparability of objective pathological data as the basis for managing patients with malignant diseases (1).
Specific standards have to be considered for the determination of the anatomical spread of malignant tumors by the clinical tumor-node-metastasis (cTNM) and pathological tumor-node-metastasis (pTNM) classifications, since these are the best to provide guidelines for individual patient therapy decisions, prognosis estimation and support health policy-relevant efforts (2).
Shift to new classifications for pT, N, and M is based on a presumed better prognostic stratification, necessarily requiring the introduction of arbitrary cut-offs validated on the simple basis of statistical observations. Moreover, the possibility of discriminating different tumor stages is addressed to satisfy the principles of reproducibility and standardization needed to obtain worldwide comparable survival curves. In fact, an ideal staging system should be independent of the type of treatment, being able to correctly stratify different prognostic groups too (123).
Changes to the cTNM/pTNM need to be 1) evidence-based and 2) compatible with the previous version in order to measure years of collected knowledge with cases from the revised classification (3). In particular, the second issue exhibits a peculiar relevance in cases of thyroid cancer characterized by low aggressiveness, resulting in long observation periods for the collection of valid clinical evidences (45).
Over the last several years, there have been important changes in the terminology used for histological classification of thyroid cancer and important changes to the American Joint Committee on Cancer (AJCC)/TNM staging. Therefore, the new 2017 AJCC/TNM staging system of the thyroid is now recommended (6).
Although the protocols are relatively straightforward, this article focuses on some practical issues as well as on occasional bias that may be encountered when the new classification is applied to stage cancers of the thyroid gland (6). However, only few contributions and comments with controversial results are reported in the literature concerning the comparison between previous and updated 2017 TNM classification for thyroid cancer.
REVISIONS OF STAGING CLASSIFICATIONS
Thyroid cancer is the most common primary endocrine neoplasm (4). All patients with thyroid cancer should undergo tumor classification and staging prior and after treatment. It is widely accepted that the knowledge of the full tumor extension spectrum (T) is essential for amenable resection and accurate interpretation to optimize patient management.
Over time, many staging and scoring systems have been proposed for the classification and prognosis of patients with thyroid malignancy (4). Currently, the non-ideal predictive performance of existing prognostic systems is due to their inherent limitations as well as to an absence of reproducibility in the results of different populations (123).
The 6th edition of the TNM classification, already published in 2002, made significant changes to categorize the spread of the primary thyroid tumor (pT category) as a clear criticism from most clinicians involved in diagnosis and therapy of thyroid cancer (78). Especially, the lack of compatibility of this classification with the previous classification (5th edition) was criticized, as both the important issues for clinical management carcinomas with a <10 mm size as well as organ growth were no longer identifiable and therefore attributable to categorization (9).
The explanations and suggestions for the ramification of the categories T1/pT1 and T3/pT3 presented in the following TNM supplement to the 6th edition into the subcategories T1a/pT1a and T1b/pT1b or T3a/pT3a, and T3b/pT3b basically contributed to the required precision (10). Unfortunately, many clinicians adhered only to the original TNM classification and did not consider the suggestions of the subsequently published TNM supplement (10). Thus, no nationwide introduction and acceptance of the proposed changes in the TNM supplement could be achieved. Incomprehensibly, the subcategorization of T1/pT1 in T1a/T1b or pT1a/pT1b introduced in 2003 in the 7th edition of the TNM classification was taken over in 2009, thus contributing basically to international standards; by contrast, the equally necessary subdivision of the category T3/pT3 in order to clearly differentiate organ-growing carcinomas thyroid-restricted carcinomas with a size larger than 4 cm was not likewise applied (11).
It should also be clarified that the TNM/pTNM categorization of thyroid carcinomas used until 2002 was not ideal, but it was at least consistent and clearly applicable (9). In particular, the fact that carcinomas with minimal cross-organism growth (i.e., microscopic evidence of tumor spread into the perithyroid adipose tissue, regardless of tumor size) in the pT4 category with (massive) growth into designated anatomical structures on the neck (musculature, trachea, larynx, esophagus, recurrent laryngeal nerve, subcutaneous adipose tissue, but also the prevertebral fascia and cervical and mediastinal vessels) were thrown into a large pot, from the point of view of biological relevance certainly made little sense (9).
During the last decades, the staging protocols continue to evolve and are under constant revision and change. The changes made in 2002 (6th edition) that carcinomas with minimal extrathyroid spread are no longer assigned to the same T/pT category as massive carcinomas infiltrating carcinomas, was therefore welcome (6). This progress was, however, relativized by the combination of minimally organ transplanting carcinomas with carcinomas limited to the thyroid gland >4 cm and also the tumor size of the carcinomas with “minimal extrathyroid propagation” remained unconsidered. However, the subcategorization T3a/pT3a and T3b/pT3b, already proposed in the 2003 Supplement (10), could eliminate the obvious deficiency taking into consideration the basis of clinico-pathological evidence.
8TH EDITION OF THE TNM CLASSIFICATION OF THYROID CARCINOMAS
Extrathyroidal extension of papillary thyroid carcinoma (PTC) is a risk factor for tumor recurrence (1213141516). By 7th edition of TNM classification, differentiated thyroid carcinoma with extrathyroidal extension is designated T3 (minimal invasion), T4a (extended invasion), or T4b (more extensive unresectable invasion), according to the degree of tumor involvement (11).
In October 2016, the AJCC (www.cancerstaging.org) published the 8th edition of the AJCC/TNM cancer staging system, which will replace the 7th edition utilized by clinicians, cancer registries and researchers since 2009 (6). The actual implementation date for the 8th edition cancer staging system was planned to be 1 January 2018 in order to allow the cancer care community to make the infrastructure changes needed for data collection and implementation (6).
The new TNM/pTNM categories only distinguish thyroid-limited carcinomas (T1/pT1, T2/pT2, and T3/pT3a) and cancer with macroscopic extrathyroid propagation in defined anatomical structures (6).
These latter structures involve the sternohyoid muscle, sternothyroid muscle, or omohyoid muscle (i.e., T3b/pT3b), or subcutaneous tissue, larynx, trachea, esophagus, recurrent laryngeal nerve (T4a/pT4a), the prevertebral fascia and/or mediastinal vessels, or surrounding the carotid artery (T4/pT4) (6). The spread to the muscles mentioned above must be macroscopically visible (6).
Microscopically evident extrathyroid propagation in perithyroid soft tissue (i.e., “minimal extrathyroid propagation”) is not mentioned in the new TNM/pTNM categories, although this is not a rare event (61213141516). Interestingly, the TNM classification of the AJCC indicates that minimal extrathyroid proliferation should not be included in either T category or stage definition (6).
For the first time, Synoracki et al. (17) proposed some changes to nicely provide the opportunity to standardize a minimal extrathyroid spread in relation to tumor size (pT category) and to make it accessible to prospective scientific analysis (Table 1). Moreover, the concept of “minimal extrathyroid spread” of thyroid carcinomas in the context of the special anatomical conditions of the thyroid gland and its limiting structures must be more precisely histomorphologically defined than before (61213141516). Nevertheless, the clinical impact of minimal extrathyroidal extension in patients with papillary thyroid microcarcinoma is still controversial (17181920).
Table 1
Proposal for additions to the 8th TNM classification of thyroid carcinomas (modified according to Synoracki et al.) (617)

| pTNM | Text of the 8th edition with amendments/additions | Comments |
|---|---|---|
| Primary tumor | Included are papillary, follicular, medullary, poorly differentiated carcinomas, hurdle cell carcinomas and undifferentiated (anaplastic) carcinomas | Expand application for medullary carcinomas |
| pTX | Primary tumor cannot be assessed | - |
| pT0 | No evidence of primary tumor | - |
| pT1a1 | Tumor 1 cm or less in greatest dimension, limited to the thyroid gland | - |
| pT1a2 | Tumor 1 cm or less in greatest dimension, with “minimal extrathyroid spread” | Definition of “minimal extra thyroidal propagation” (see section of the same name) |
| pT1b1 | Tumor more than 1 to 2 cm or less in greatest dimension, limited to thyroid | - |
| pT1b2 | Tumor more than 1 to 2 cm or less in greatest dimension, with “minimal extrathyroid propagation” | Definition of “minimal extrathyroid propagation” (see section of the same name) |
| pT2a | Tumor more than 2 cm, but not more than 4 cm in the largest extent, limited on the thyroid gland | - |
| pT2b | Tumor more than 2 cm, but not more than 4 cm in largest extent, with “minimal extrathyroid propagation” | Definition of “minimal extrathyroid propagation” (see section of the same name) |
| pT3a1 | Tumor more than 4 cm in largest extent, limited to the thyroid gland | - |
| pT3a2 | Tumor more than 4 cm in largest extent, with “minimal extrathyroid spread” | Definition of “minimal extrathyroid propagation” (see section of the same name) |
| pT3b | Tumor of any size with macroscopic extrathyroid propagation in named neck muscles (i.e., spread into sternohyoid muscle, sternothyroid muscle, or M. omohyoideus) | A microscopic confirmation of the macroscopic findings is essential for definition |
| pT4a | Tumor spreading beyond the thyroid capsule and invading one or more of the following structures: subcutaneous soft tissue, larynx, trachea, esophagus, recurrent laryngeal nerve | - |
| pT4b | Tumor invades pre-vertebral fascia, mediastinal vessels or encloses the carotid artery | - |
| pNX | Regional lymph nodes cannot be assessed | |
| pN0 | No regional lymph node metastases | Selective neck dissection and histological examination usually of 6 or more lymph nodes. If the examined lymph nodes are tumor free, but the number of usually examined lymph nodes is not reached, should be classified pN0? |
| pN1a1 | Metastases in lymph nodes of the level VI (pretracheal and paratracheal, included prelaryngeal lymph nodes/Delphi lymph nodes) or upper mediastinal lymph nodes; limited to the affected lymph nodes; without extracapsular spread | |
| pN1a2 | Metastases in lymph nodes of the level VI (pretracheal and paratracheal, included prelaringeal lymph nodes/Delphi lymph nodes) or upper mediastinal lymph nodes, with extracapsular spread | Extranodal spread of lymph node metastases is with a significantly worse prognosis associated (181920) |
| pN1b1 | Metastases in other unilateral, bilateral or contralateral cervicals (level I, II, III, IV, and V) or retropharyngeal lymph nodes; on the restricted lymph nodes; without extracapsular spread | |
| pN1b2 | metastases in other unilateral, bilateral or contralateral cervicals (level I, II, III, IV, and V) or retropharyngeal lymph nodes, with extracapsular spread | Extranodal spread of lymph node metastases is with a significantly worse prognosis associated (181920) |
| pM1 | Distant metastasis microscopically confirmed | pM0 and pMX are in the pTNM categorization no applicable categories |
![]()
HUMAN THYROID GLAND
The degree and site of invasion is an important prognostic factor for thyroid cancer.
Grossly, the human thyroid gland is a lobular epithelial organ embedded in soft tissue (fat and striated muscle) (21); it consists of 2 lateral lobes, centrally connected by the isthmus, which gives a butterfly-like appearance to the thyroid (22). The more or less marked lobus pyramidalis represents the caudal remnant of the developmental thyreoglossus duct (23).
The tissue of the thyroid gland is mostly composed of follicles, which are made up of a central cavity filled with a sticky fluid called colloid.
The thyroid is surrounded by a capsule of fibroelastic tissue that is continuous with the surrounding peritracheal fascia. The capsule sends septa into the gland, dividing it into lobules. The connective tissue septa support the parenchyma and carry blood vessels, lymphatics and nerves.
There are some regional specificity of the thyroid capsula. The higher resolution reveals that ventral and lateral areas of the 2 lobes are covered by a predominantly continuous connective tissue, while the posterior border of both lobes is opposite adjacent to soft tissue, the so-called thyroid bed, formed by an interrupted and, if present, only very narrow connective tissue capsule (24) (Fig. 1). In the dorsal area, thyroid lobules present adipose tissue parts (25). However, in the isthmus area and in the surrounding of the pyramidal lobe, the thyroid tissue is partially devoid of a defined connective tissue capsule, while striated muscle tissue between lobes of the thyroid can be regularly demonstrated (26, 27) (Fig. 1).

DEFINITION OF “MINIMAL EXTRATHYROID SPREAD”
Local control of PTC with extrathyroid invasion is very important for avoiding residual cancer either in locoregional or in distant metastasis. Additional soft tissue involvement by PTC at the surgery time is an important prognostic factor for long-term patient outcome.
In histopathology, invasive/infiltrative growth is defined as invasion of tumor cells into neighboring structures (25) (Figs. 2 and 3). As a rule, the spread is carried out in non-neoplastic tissue surrounding the invasively growing tumor (26). Occasionally, invasive thyroid carcinoma may infiltrate another neoplasm, such as a parathyroid tumor or a concomitant laryngeal tumor (27).

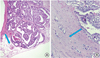 | Fig. 3(A) Papillary thyroid cancer with peri-thyroidal adipose tissue invasion (arrow); (B) intracapsular neoplastic cells (arrow).
|
In the 6th and 7th editions of the TNM classifications, a distinction was made between a “minimal extrathyroid propagation” for thyroid carcinoma and a series of anatomical structures (T4a/pT4a, T4b/pT4b) (T3/pT3) (71126). The microscopic evidence of a “minimal extrathyroid propagation,” however, is obviously subject to a very broad individual interpretation (252627). In detail, the definition of “minimal extrathyroid spread” as used herein includes all primary thyroid carcinomas (in almost all cases it will be an unencapsulated tumor) that more or less infiltrates perithyroid adipose tissue, without any of the subcategories T3b/pT3b, T4a/pT4a, and T4b/pT4b to reach designated structures (26).
In carcinomas located in tissue portions of the connective tissue capsule, the tumor must completely grow through the capsule, but occasional stromal myoplasia may make it difficult or even impossible to assess the course of the thyroid capsule (26). In analogy to other organs (such as the prostate gland), an imaginary course of the original organ capsule can be used as an important reference for assessing an organ-spreading spread (252627).
A special situation exists in the area of the interlobular adipose tissue retractions described above and therefore each infiltration of this adipose tissue should be consequently regarded as “minimal extrathyroid propagation.” However, tumor may invade islands of mature adipose tissue, which can be found regularly within the thyroid tissue, but the occurrence of adipocytes within thyroid neoplasias (adenomas and carcinomas) should be differentiated from the former finding (26).
In thyroid areas with no defined capsule boundary (isthmus, lobus pyramidalis), any infiltration of adipose tissue by a carcinoma is also logically considered to be a “minimal extrathyroidal spread.” Occasionally, there is also a microscopic spread of carcinomas of the striated musculature in this region (26).
In contrast to Mete et al. (28) statement, “minimally invasive” tumor infiltration of the perithyroid soft tissue per se should be considered biologically relevant and therefore examined as organ trans-extrathyroidal growth, since the published studies have yielded quite contradictory results (121628293031).
The prospective categorization of thyroid carcinomas, which spread microscopically from their tissue of origin into the surrounding soft tissue, should be based on the modifications that Synoracki et al. (17) and Brierley et al. (32) proposed in the 8th edition of the TNM classification. Consequently, the “minimal extrathyroid spread” in thyroid carcinoma represents the basis of a systematic scientific analysis of biological relevance, including at the same time the tumor size given as pT category (Table 1) (172632). Furthermore, an analysis of tumor localization as prognostic factor is attractive in the near future (33); on this way, the location of thyroid cancer in the isthmus may be considered as an additional risk factor for radioactive iodine (RAI) avid metastatic disease in pT1a-pT1b DTC patients, regardless of the presence or absence of other risk factors (33).
EVALUATION OF PATIENTS FOLLOWING INITIAL SURGERY FOR MEDULLARY THYROID CARCINOMA (MTC)
The new AJCC staging system (8th edition) has been applied to patients with MTC (6). By definition, a T3a is a tumor >4 cm limited to thyroid, while T3b consists in gross extrathyroidal extension invading only strap muscle (6). The age more than 55 years is associated with poor prognosis (6).
However, in patients with MTC the TNM classification lacks important prognostic factors including: 1) pre- and postoperative serum calcitonin and carcinoembryonic antigen levels, 2) specific mutations as genetic markers, and 3) hereditary associated malignancies (626). Moreover, the AJCC TNM classification for MTC categorize lymph node metastases, not by number but according to the location of nodes within (N1a) or without (N1b) the central neck, regardless the involved compartments. The AJCC staging system should be modified to include groups of lymph node metastases according to number of positive nodes (626).
DISCUSSION
The 8th TNM classification, which has been applicable since the beginning of 2017, only categorizes thyroid-restricted carcinomas (T1/pT1, T2/pT2, and T3/pT3a) and extrathyroid carcinomas into named anatomical structures (6).
An already macroscopically recognizable (non-microscopic) infiltration of the sternohyoid muscle, sternothyroid muscle or omohyoid muscle (T3b/pT3b) or macroscopic or microscopic spread in subcutaneous soft tissue, larynx, trachea, esophagus, recurrent laryngeal nerve (T4a/pT4a), the prevertebral fascia and/or mediastinal vessels or enclosing the carotid artery (T4/pT4) are also categorized (6).
Microscopic “minimal” extrathyroid proliferation into perithyroid soft tissue without infiltration of named structures is lacking, although this is not a rare event and it was included in previous TNM classifications and consistently applied by pathologists and clinicians (791134).
A histologically proven “minimal extrathyroid spread” of thyroid carcinomas has clearly defined effects on the postoperative management of the affected patients through the currently valid guidelines on thyroid carcinoma (35). A recent proposal to categorize carcinomas with “minimal extrathyroid proliferation” was summarized in Table 1 (172632). Consequently, the T-categories pT1a, pT1b, pT2 and pT3a are each subdivided into true thyroid-restricted carcinomas (pT1a1, pT1b1, pT2a, and pT3a1) and “minimal extrathyroid proliferation” carcinomas (pT1a2, pT1b2, pT2b, and pT3a2). This proposal appears necessary to remedy the obvious deficiencies of the 8th edition, in contrast to previous editions of the TNM classification, combining the “minimal extrathyroid proliferation” with the size of the tumor (pT category) as a potential prognostic and therapeutic parameter (6172632).
Oncological outcome correlates with the extent of extrathyroidal invasion, being worse in patients with gross extrathyroidal disease extension than in those with microscopic local invasion apparent on histopathological assessment. However, the risk of clinical recurrence appears similar between patients undergoing margin-negative and “close margin” resection (31). An indication of the possible relevance of this combined parameter is provided by the study by Radowsky et al. (31). In detail, a retrospective analysis on 276 patients with PTC treated between 1955 and 2004 has been performed to determine the impact of margin-negative resection (n=199, 72%), disease up to within 1 mm of surgical margin (n=19, 7%), microscopic (n=39, 14%), and gross (n=19, 7%) extrathyroidal extension (31); in the study, the median follow-up was 3.1–6.8 years per study group (disease-free survival, range 1–37 years) (31). The proportion of patients with age >45 years, prior radiation exposure, distant metastasis at presentation, and those undergoing total thyroidectomy did not exhibit significant differences between groups (31). Tumor size and multifocality correlated with extent of local disease, which in turn was significantly associated with regional nodal disease at the time of first surgery as well as with prevalence of persistence of disease after multimodality therapy. Extent of local disease significantly correlated with subsequent clinical recurrence after a disease-free period (P=0.006); however, recurrence rates were not significantly different between negative and close (≤1 mm) margin resection (31).
According to the new TNM classification, the extra-thyroid spread (T-category) of thyroid carcinoma is considered as an essential prognostic factor as well as the exclusion or detection of residual tumor (R0 vs. R1 vs. R2) (617263132).
Comparative studies have shown, however, that in the evaluation of the extrathyroid propagation of thyroid carcinoma, there is little agreement among pathologists, which inevitably calls into question the significance of this parameter as an independent prognostic factor (36). However, the main cause of the mismatch is likely to be the lack of a clear definition of the “minimal extrathyroid spread” of a thyroid carcinoma. To remedy this shortcoming, Authors recently proposed a strict definition of “minimal extrathyroid proliferation” (17). Therefore, any microscopically detectable spread of carcinoma primarily from the thyroid tissue into the surrounding adipose tissue has been consistently considered a “minimal extrathyroidal spread,” regardless of whether or not the thyroid tissue in the area of extrathyroid carcinoma spread is delimited by a (narrow) connective tissue capsule. This definition provides the scientific basis for demonstrating or excluding the biological relevance of a microscopically proven “minimal extrathyroid propagation.”
For Mete et al. (28) “minimal invasion” of thyroid carcinoma into perithyroid soft tissue (adipose tissue) did not represent a relevant prognostic factor, while tumor invasion into named structures (named cervical muscles, subcutaneous soft tissue, larynx, trachea, esophagus, recurrent laryngeal nerve, prevertebral fascia, mediastinal vessels) was associated with a worsening of the prognosis (121628293031). This view is supported by some studies, while other studies revealing “minimal extrathyroid proliferation” certainly show significant prognostic importance and appear to be of high interest for the further management of patients (121628293031).
Another intriguing proposal concerns the lymph node capsule-sprouting growth of metastases of thyroid carcinoma, which presents a scientifically documented prognostic value (see also Table 1) (20). In particular, the categories pN1a and pN1b have been subdivided into the subcategories pN1a1/pN1b1, when metastases were limited to the affected lymph nodes or pN1a2/pN1b2, when metastases exhibited extranodal spread.
The incidence of thyroid carcinoma has almost tripled in the last 2 decades, which has been regarded as a “diagnostic epidemic” of generally indolent tumors rather than a “real increase” in thyroid carcinomas (3738). In the meantime, the improved morphological diagnostic approach allows to identify some peculiar new histologic entities, commonly considered to be “very low-risk carcinomas” (3540414243). Among them, unifocal papillary microcarcinomas limited to the thyroid gland (3940), encapsulated follicular carcinomas without angioinvasion but characterized exclusively by a capsular breakthrough (3540414243) and non-invasive follicular neoplasia with papillary-like nuclear features (NIFTP) (4044) have been identified; consequently, further changes in the classification of thyroid tumors should be introduced in order to define these tumors with extremely low malignancy potential.
Finally, the cooperation between the pathologist and surgeon is indispensable in improving the quality of patient care especially in, but not limited to, the area of thyroid cancer management and care. Surgeon's role is important as well as pathologist in new TNM classification. When surgeons perform thyroidectomy, they use perithyroidal sheath or false thyroid capsule. In case of extrathyroidal extension to strap muscle, surgeons resect strap muscle in part. However, the pathologic result with no invasion to strap muscle is not a rare event. Thus, the communication between pathologists and their thyroid surgeon colleagues of pertinent clinical and intraoperative information should be enhanced because, it is often circumstantial and usually occasioned by clinicopathological discrepancies recognized by the surgeon.
 XML Download
XML Download