

 PDF
PDF ePub
ePub Citation
Citation Print
Print


TO THE EDITOR: A 38-year-old man with history of corrected rheumatic heart disease was incidentally diagnosed with BCR-ABL1-positive chronic myeloid leukemia (CML). He was treated with imatinib 400 mg/day, with which he achieved major molecular remission (MMR) after 12 months of therapy. He was followed up regularly with examinations of complete blood counts and 6-monthly quantitative BCR-ABL1 transcript levels, which improved to MR4.5 in 24 months. After 4 years of regular treatment with good drug compliance, he showed loss of MMR on routine testing with increased BCR-ABL1/ABL1 transcript levels of up to 32.4% on the international standard (IS) scale. Hemogram showed hemoglobin level of 68 g/L, leukocyte count of 4.6×109/L, and platelet count of 202×109/L. Peripheral blood film (PBF) showed leukoerythroblastic picture with eosinophilia (13%), basophilia (10%), and significant dysgranulopoiesis (Fig. 1A–C). Bone marrow was markedly hypercellular with 4% blasts, marked dysgranulopoiesis, dysmegakaryopoiesis (>90% dwarf forms) (Fig. 1D, E), eosinophilia (16%), and basophilia (9%). This morphology was consistent with a loss of hematological responses. Conventional cytogenetics revealed 49,XY,+8,t(9;22)(q34;q11.2),i(17)(q10),+der (22)t(9;22)(q34;q11.2). Fluorescent in situ hybridization (FISH) using the Vysis BCR/ABL1/ASS1 Tri-Color Dual Fusion Probe and TP53/CEP17 dual colour Probe (Abbott Molecular, Abbot Park, IL, USA) confirmed the presence of an additional Philadelphia chromosome and loss of one copy of TP53 gene in concordance with isochromosome 17q (Fig. 1F, G). In a patient who previously achieved MMR, these cytogenetic abnormalities suggest clonal evolution and hence are consistent with accelerated phase of CML. In view of secondary resistance to imatinib therapy, ABL kinase domain mutation analysis by Sanger sequencing was performed, which did not reveal any mutations. He was subsequently administered dasatinib 100 mg daily. However, after 2 weeks of treatment, the patient developed symptoms of fluid overload and heart failure attributed to dasatinib. The dose of dasatinib was then decreased to 50 mg daily, which was well tolerated. The patient showed normalization of counts, and the 3-month quantitative BCR-ABL/ABL ratio was 3.4% IS (target <10%). However, he continued to show granulocytic dysplasia in PBF. FISH revealed BCR-ABL positivity and additional signals consistent with extra Philadelphia chromosomes in 90% of the cells. Dysplasia, although not a recognized criterion, has been previously reported as a characteristic feature of accelerated phase of CML [12]. Even in the era of molecular monitoring, a careful morphological evaluation of PBF continues to be important when accelerated phase of CML is suspected, and further confirmatory tests, such as chromosome studies, should be performed for early diagnosis and subsequent timely treatment. The inclusion of dysplasia as a surrogate marker of clonal evolution should be further investigated in larger studies.
Figures and Tables
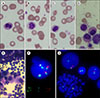 | Fig. 1(A–C) Peripheral blood film shows significant dysgranulopoiesis in the form of hypolobation of the nucleus, hypogranulation, and abnormal coarse chromatin clumping. Platelet anisocytosis with large and giant platelets were also found. (D, E) Hypercellular bone marrow shows dysgranulopoiesis and many dwarf megakaryocytes (×40, May-Grunwald Giemsa stain). (F) Fluorescent in situ hybridization (FISH) using BCR/ABL1/ASS1 Tri-Color Dual Fusion Probe shows 1 orange aqua (normal ASS1-ABl1 gene), 1 green (normal BCR gene), 1 orange aqua green (from derivative chromosome 9 with ASS1-ABL1-BCR fusion gene), and 2 orange green fusion (from derivative 22 with BCR-ABL1 fusion genes) signals, which are consistent with the presence of an extra Philadelphia chromosome. (G) FISH using TP53/CEP17 probe shows 1 orange (from TP53 gene) and 2 green signals (from centromere of chromosome 17), which is consistent with loss of 1 copy of TP53 gene in concordance with isochromosome 17q.
|
Acknowledgments
All authors have contributed equally in this manuscript. All authors agree to the content of the manuscript and its interpretations.
References
1. Enright H, Weisdorf D, Peterson L, Rydell RE, Kaplan ME, Arthur DC. Inversion of chromosome 16 and dysplastic eosinophils in accelerated phase of chronic myeloid leukemia. Leukemia. 1992; 6:381–384.
2. Bain BJ, Heller M. Dysplastic basophils in the accelerated phase of chronic myelogenous leukemia. Am J Hematol. 2011; 86:949.

 XML Download
XML Download