

 PDF
PDF ePub
ePub Citation
Citation Print
Print


TO THE EDITOR: Babesiosis is an infectious disease caused by hemoparasite Babesia and transmitted by certain ticks or transfusions. Few Babesia species (B. microti, B. venatorum, B. duncani, B. divergens) are associated with human infection. Although many patients are asymptomatic and recover spontaneously, the infection can be persistent, refractory, and life-threatening in immunosuppressed hosts, especially those receiving chemotherapy or immunosuppression, transplant, or splenectomy [1234].
We report the case of a healthy young patient who was concurrently diagnosed with acute symptomatic Babesia infection and chronic myeloid leukemia (CML). A 23-year-old man, living in New Hampshire, presented with fever, fatigue, myalgia, and arthralgia for 2 weeks. The patient had no history of any malignancy, transfusion, chemotherapy, or immunosuppression. He had no recent travels or did not recall any tick exposure.
At admission, the patient complained of sweating, body aches, and headache. Physical examination was unremarkable except fever (40℃). Blood tests showed left-shifted neutrophilic leukocytosis (white blood cell: 89.6×103/µL; myelocyte 17%, metamyelocyte 8%, band/segmented neutrophil 69%, lymphocyte 3%, monocyte 3%) and normocytic anemia (hemoglobin 9.3 g/dL; mean corpuscular volume 84.5 fL). Serum liver function tests were normal except increased lactate dehydrogenase (654 U/L). Abdominal computed tomography scan showed splenomegaly. After specimen collection for blood culture and serologic tests to rule out the infectious etiology, the patient was started on general antimicrobial therapy. The blood culture for aerobic and anaerobic microorganisms was negative. Serologic tests showed positive B. microti immunoglobulin M (IgM; >1:320; reference range, <1:20) and cytomegalovirus (CMV) IgM (2.57; reference range, <0.89). Human immunodeficiency virus screening, Lyme IgM/IgG, Epstein-Barr virus anti-viral capsid antigen IgM, B. microti IgG, and Anaplasma phagocytophilum IgM/IgG antibodies were negative. Monospot test result was negative.
Given the presence of marked left-shifted neutrophilic leukocytosis in peripheral blood (PB), bone marrow (BM) biopsy was performed to rule out leukemoid reaction or underlying myeloid neoplasm. BM biopsy showed hypercellularity (100%) and left-shifted granulocytic hyperplasia. Megakaryocytes were slightly increased with many having small hypolobated (dwarf) forms (Fig. 1A, B). Sea-blue histiocytes were increased. However, there were no increased blasts or significant dysplasia. Flow cytometric analysis showed no evidence of a lymphoma or leukemia. Results of immunohistochemistry for CMV was negative on the core biopsy. Interestingly, BM aspirate smears showed many small single or multiple ring-form organisms within the erythrocytes, with occasional 4 rings representing the stages after breakdown of the classic tetrad (“Maltese cross”) (Fig. 1C). No other cellular inclusions or granulomatous lesions were noted. Acute Babesia infection was diagnosed in combination with elevated B. microti IgM by immunoassay. Fluorescent in situ hybridization demonstrated BCR/ABL1 fusion in 187/200 (93.5%) of interphase cells (Fig. 1D). Karyotype showed 46,XY,t(9;22)(q34;q11.2) [20]. Real-time quantitative polymerase chain reaction (PCR) showed p210 BCR/ABL1 fusion transcript (e13a2 and e14a2; International Scale 60.8%) in PB. Therefore, diagnosis of CML in chronic phase was rendered. After diagnosis of Babesiosis, the patient received antimicrobial therapies (atovaquone, azithromycin, clindamycin) for 7 days and showed a good response with no intraerythrocytic Babesia in PB smears. Therapy of tyrosine kinase inhibitors (TKIs) and potential BM transplant were discussed.
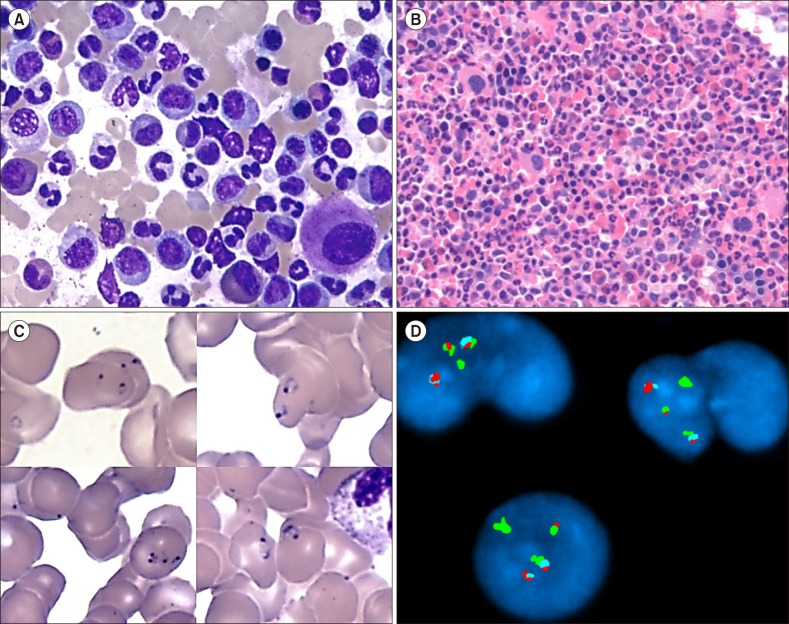 | Fig. 1Bone marrow (BM) histopathologic and cytogenetic findings at diagnosis. (A, B) BM aspirate and biopsy showed left-shifted granulocytic hyperplasia with a high myeloid:erythroid ratio and megakaryocytes with small hypolobated (dwarf) forms (A: Wright-Giemsa stain, ×1,000, B: hematoxylin and eosin stain, ×400). (C) The composite pictures from the aspirate smears showed small single or multiple ring-form organisms within the erythrocytes. One of the erythrocytes in the left lower part showed the stage occurring after the breakdown of the classic tetrad (“Maltese cross”) (Wright-Giemsa stain, ×1,000). (D) Fluorescent in-situ hybridization in BM specimen using tri-color dual fusion probes (BCR/ABL1/ASS1) demonstrated BCR/ABL1 translocation (red-green fusion) in 3 interphase cells. ABL1 and ASS1 probes in chromosome 9q34 region and BCR probe in chromosome 22q11.2 region showed red, aqua, and green signals, respectively (Abbott Molecular, Abbott Park, IL).
|
The Northeast and Upper Midwest part of the US is endemic for Babesiosis, and the majority of infection is caused by B. microti, transmitted by the tick, Ixodes scapularis, which also causes Lyme disease and anaplasmosis. Elderly, immunocompromised, or asplenic patients are at high risk of persistent Babesia infection [4]. Acquired Babesiosis after transfusion of blood products from asymptomatic donors has been recently increasing [5]. The clinical manifestations of Babesiosis, which infects erythrocytes, can range from asymptomatic disease to mild/moderate to fatal illness. Mild/moderate illness can manifest as non-specific flu-like symptoms (chills, sweats, anorexia, headache, myalgia, non-productive cough, arthralgia). Physical examination can include fever or splenomegaly and hepatomegaly occasionally. Severe Babesiosis can cause severe hemolytic anemia, disseminated intravascular coagulation, acute renal failure, and multisystem organ failure, which is threatening in immunosuppressed or asplenic patients [236].
The patient likely had an environmental source of infection since he never received transfusions or immunosuppressive therapy, was physically active, and lived in New Hampshire, an endemic area for Babesia. When tick exposure is suspected, other infections such as Lyme disease/borreliosis, ehrlichiosis, and anaplasmosis should be screened to rule out co-infection. Up to 50% of Babesiosis patients have a history of Lyme disease or positive serologic results for antibodies against Borrelia burgdorferi [6].
The diagnosis of Babesiosis is made after identifying small single or multiple ring forms or the pathognomonic “Maltese cross” or tetrads of Babesia organisms within/outside erythrocytes on thin blood smears [36]. The exclusion of other parasites forming intraerythrocytic ring forms should be taken into consideration as differential diagnosis. PCR and serologic studies support the diagnosis and help in monitoring the therapeutic response. As shown in this case, antimicrobial therapy with either quinine and clindamycin or atovaquone and azithromycin for 7–10 days is effective for mild/moderate Babesiosis. However, the therapy can be prolonged for at least 6 weeks in immunocompromised patients with additional transfusions [57].
In this young patient, BM biopsy and genetic studies revealed chronic phase of CML. The median age of CML diagnosis is approximately 67 years. CML diagnosed at younger ages (15–29 yr) is referred to as adolescents and young adults (AYA) and represents a small distinct group, ranging from 8% to 13% of all CML patients [89]. Studies of AYA patients with CML demonstrated different biology and prognosis compared with older patients [8910]. AYA patients show higher leukocyte count, incidence of splenomegaly, higher PB blasts percent, and lower hemoglobin levels than older patients. Splenomegaly in CML is attributed to the expansion of myeloid cells and immune-inflammatory response. The spleen sequesters erythrocytes infected with Babesia or platelets by macrophages. In immunocompetent patients with some degree of higher splenomegaly, like our patient, Babesia infection can cause spontaneous splenic rupture or infarction related to splenic erythrophagocytosis [38].
TKI therapy has drastically improved the outcome of CML patients. Survival outcomes seem to be unaffected by age. However, AYA patients show higher progression rate to aggressive or blastic phase and inferior response to TKI therapy than older patients [89].
To the best of our knowledge, this is the first case of concurrent diagnosis of acute symptomatic Babesiosis and CML in a young immunocompetent adult.
 XML Download
XML Download