

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The advent of various novel agents, including the new generation of proteasome inhibitors and immunomodulatory drugs, has significantly improved the median survival of patients with multiple myeloma (MM) [1]. Nevertheless, upfront autologous stem cell transplantation (ASCT) remains an integral part of MM treatment, especially for patients younger than 65 years old [23]. Several strategies focusing on different aspects of the ASCT process have been proposed to achieve better overall outcomes. The most extensively developed approach is intensification of the induction regimen administered before ASCT by means of incorporating and combining newer agents [4]. Unfortunately, the median duration of response remains shorter than 4 years even with novel agent induction, and most patients inevitably experience progression [56]. The administration of maintenance therapy following ASCT has also received a great deal of attention in recent years [78910111213]. Thalidomide [11] and lenalidomide maintenance [1213] have consistently shown improved survival [11]. In the real world, however, the use of these agents is somewhat limited in light of their toxicity, as well as financial concerns.
The final strategy, an approach not as extensively explored, is to enhance the immediate pre-transplantation conditioning regimen by either increasing the dose of melphalan or adding another agent. Either melphalan 200 mg/m2 or high-dose melphalan (HDMEL) is the current standard conditioning regimen [14]. Only a handful of alternatives have been studied, and while most failed to show convincing superiority over HDMEL, combined busulfan and melphalan (BUMEL) has shown encouraging results [1516171819]. We designed the present study to investigate the efficacy and clinical outcomes of BUMEL conditioning in Korean patients with MM undergoing upfront ASCT.
Go to : 
MATERIALS AND METHODS
Medical insurance is provided in a universal form in Korea. The National Health Insurance (NHI) program, operated by the Korean Ministry for Health and Welfare, is the sole and mandatory insurance system, covering approximately 98% of the overall Korean population [20]. Meanwhile, the Korean Health Insurance Review and Assessment Service (HIRA) is a government-affiliated organization responsible for insurance claims review and quality control of the NHI. Since the Korean population itself is fairly ethnically homogeneous, both the NHI and HIRA databases can be readily used for nationwide analyses. For the present study, we utilized information from the HIRA and NHI databases to identify adult patients with MM undergoing upfront ASCT between January 2010 and December 2014. Adult patients were defined as those ≥18 years old. We extracted data including patient demographics, time from MM diagnosis to ASCT, bortezomib exposure prior to ASCT, parameters related to ASCT including conditioning regimen and year of ASCT, and survival. Because drugs used as a part of clinical trials are not covered by the NHI, we assumed that patients receiving any treatment within 3 months of MM diagnosis were likely to have participated in clinical trials, and these patients were thus excluded from the study. Patients undergoing tandem transplantation were also excluded. Initially, 1,197 patients undergoing HDMEL conditioning and 107 patients undergoing BUMEL (intravenous busulfan) conditioning were identified. After case matching according to age, gender, year of ASCT, and bortezomib exposure prior to ASCT, 428 patients undergoing HDMEL conditioning and 107 patients undergoing BUMEL conditioning were enrolled for final analyses.
Overall survival (OS) and progression-free survival (PFS) curves were estimated using the Kaplan-Meier method. OS was defined as the time from the date of ASCT to death from any cause. PFS was derived from the date of ASCT to that of progression/relapse, or death from any cause. Transplantation-related mortality (TRM) was defined, tentatively, as death occurring within 100 days of ASCT. Univariate and multivariate proportional hazards regression models were used to identify independent risk factors for survival by means of Cox proportional hazards models. Factors associated with ASCT prognosis were included in multivariate analysis. Differences between groups were assessed using Student's t-test or one-way analysis of variance for continuous variables, and Pearson's chi-square test for categorical variables, as indicated. All analyses were performed using SAS v9.4 (SAS Institute Inc., Cary, NC, USA). P-values of <0.05 were considered statistically significant. This study was conducted according to the ethical standards of the Declaration of Helsinki and was approved by the institutional review board of Seoul National University Hospital. All authors had access to the study data and reviewed and approved this study.
Go to :
RESULTS
Clinical characteristics
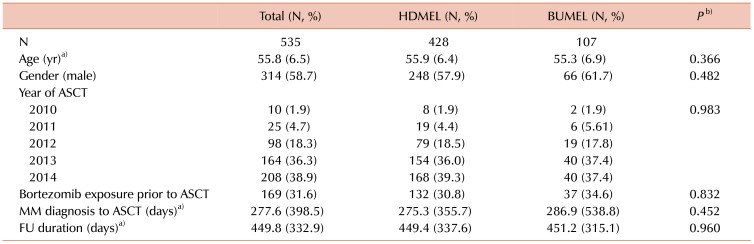
The baseline characteristics of the enrolled patients are shown in Table 1. The mean age for the total cohort was 55.8 years, and the mean time from MM diagnosis to ASCT was 277.6 days (approximately 9.3 mo). About one-third of the patients were exposed to bortezomib prior to ASCT.
Outcomes and toxicity
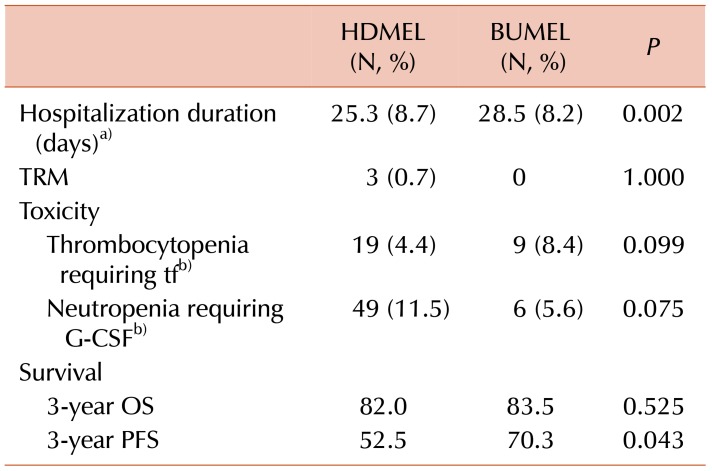
The outcomes of ASCT are shown in Table 2. Patients undergoing BUMEL conditioning consistently showed better PFS than those undergoing HDMEL conditioning. The 3-year PFS for BUMEL group was 70.3% compared to 52.5% for the HDMEL group (P=0.043). This result translated into better PFS overall, as seen in Fig. 1B, and the median PFS for BUMEL was not reached while the median PFS for HDMEL was 1,000 days (P=0.0351). On the other hand, the OS did not differ between the 2 groups. The 3-year OS for BUMEL was 83.5%, while it was 82.0% for HDMEL 82.0% (P=0.525), and no differences were observed between the survival curves, as shown in Fig. 1A.
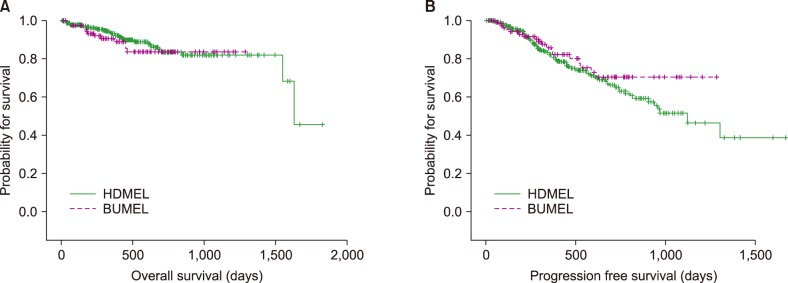 | Fig. 1(A) Overall survival compared between patients receiving high-dose melphalan conditioning regimen and patients receiving melphalan plus busulfan regimen (P=0.506). (B) Progression-free survival compared between the 2 groups (P=0.0351). MEL, HDMEL; Others, BUMEL.
|
Table 2
Outcomes of autologous stem cell transplantation.
a)Data presented as mean (±standard deviation). b)The number represents the number of patients requiring platelet transfusion or G-CSF support, respectively.
Abbreviations: BUMEL, busulfan plus melphalan; G-CSF, granulocyte colony stimulating factor; HDMEL, high-dose melphalan; OS, overall survival; PFS, progression-free survival; tf, transfusion; TRM, transplantation-related mortality.
![]()
There were 3 cases of TRM in HDMEL group. Patients in HDMEL group also required more granulocyte colony stimulating factor (G-CSF) support. Meanwhile, patients in BUMEL group were associated with longer hospitalization duration compared to those in HDMEL group (28.5 days vs. 25.3 days, respectively, P=0.002), and more platelet transfusion.
On multivariate analyses (Table 3), only the history of bortezomib exposure was recognized as an independent prognostic factor of OS. Conditioning regimen was not associated with survival differences, indicating BUMEL was not inferior to HDMEL with regards to both PFS and OS.

Go to :
DISCUSSION
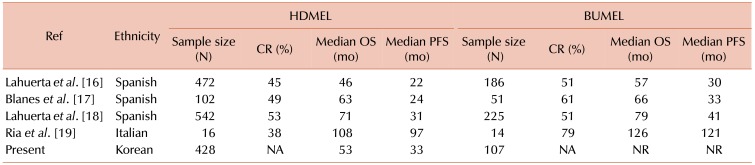
Despite recent advances in MM treatment, upfront ASCT in fit patients is a prerequisite for long-term disease control. Opportunities to optimize the outcomes of ASCT exist at all stages throughout the process, including induction, conditioning, and maintenance. Several improvements in the induction and maintenance regimens have been established, but few studies have focused on improving conditioning regimens. These previous studies have proposed BUMEL as an attractive alternative to HDMEL to achieve maximum anti-myeloma capacity [16171819]. In the present study, we sought to explore the role of the addition of busulfan in an often under-represented Asian population, as a significant correlation between glutathione S-transferase (GST) genotype and busulfan clearance exists [21], and the frequency of GST polymorphisms is higher in Asians [2223]. Our findings, similar to the results of previous studies (Table 4), showed that BUMEL conditioning was associated with longer PFS compared to HDMEL conditioning. The advantage of BUMEL in extending PFS did not translate into OS improvement, probably because as MM is a longstanding disease, OS is dependent on the effects of subsequent lines of salvage treatment. Patterns of hematopoietic recovery varied between the 2 groups, with patients in the HDMEL group requiring more G-CSF support and those in the BUMEL group requiring more platelet transfusion, but the differences did not reach statistical significance.
One major pitfall of our study is the lack of details regarding patient characteristics and treatment courses. Our analyses were restricted to the limited range of information available from the national databases. Consequently, responses to ASCT and the role of maintenance treatment could not be estimated. However, some of the missing parameters can be estimated. For example, although information regarding disease control status prior to ASCT is unknown, it is safe to assume that all patients showed partial or better response to induction treatment following the strict reimbursement regulations. Also, owing to the almost uniform insurance coverage of therapeutic agents used for MM treatment, it is likely that most patients received somewhat stereotyped treatment. Thus, we would like to point out that despite its retrospective nature, our study was conducted in a somewhat homogeneous setting. Furthermore, considering the scarcity of data from Asian populations, the importance of our findings is not diminished.
In conclusion, our study suggest BUMEL conditioning regimen for newly diagnosed MM patient undergoing upfront ASCT is an attractive alternative to HDMEL conditioning regimen in Korean population.
Go to :
 XML Download
XML Download