

 PDF
PDF ePub
ePub Citation
Citation Print
Print


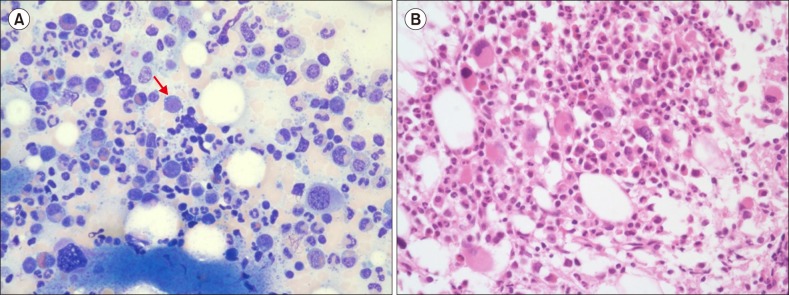
A 76-year-old woman was admitted with dizziness for 2 weeks. No organomegaly or lymphadenopathy was revealed on physical examination. Initial blood cell values were as follows: hemoglobin, 5.4 g/dL; mean corpuscular volume, 105 fL; white blood cell count, 8.1×109/L (differential count: neutrophils, 54%; lymphocytes, 37%; monocytes, 6%; eosinophils, 3%); platelet count, 402×109/L; and absolute reticulocyte count, 3.9×109/L. Biochemical and serologic test results were unremarkable. Direct Coombs test result was negative. Bone marrow (BM) examination showed hypercellular marrow with marked erythroid hypoplasia (1.4% erythroblasts). The estimated myeloid-to-erythroid ratio was 72:1. Most erythroblasts found were early erythroid precursors, and late erythroblasts were rarely observed (A, BM aspiration, Wright-Giemsa stain, ×400, arrow). Granulopoiesis was normal; however, dysplastic megakaryocytes with non-lobulated and hypolobulated nuclei were observed in several fields (B, BM biopsy, hematoxylin and eosin stain, ×400). No evidence of thymoma was detected on computed tomography scans. Subsequently, chromosome study demonstrated 46,XX,del(5)(q15q33)[18]/46,XX[2]; therefore, the patient was diagnosed with myelodysplastic syndrome (MDS) with isolated del(5q). Erythroid hypoplasia is frequently observed in 5q- syndrome; however, a marked decrease with maturation arrest of erythropoiesis mimicking pure red cell aplasia is very unusual. TP53 activation has been suggested to cause erythroid suppression in MDS with del(5q).
 XML Download
XML Download