

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Freshly consumed apples can induce allergic reactions due to 4 classes of allergens: Mal d 1, Mal d 2, Mal d 3, and Mal d 4.1 These allergens have been extensively studied due to their high cross-reactivity with homologous antigens present in common plants and food and their substantial clinical relevance in allergic reactions.2345678 According to recent reports, up to 90% of patients allergic to birch pollen Bet v 1 or its homologues show immunoglobulin E (IgE)-mediated reactions to plant fruits including apples.91011 An increasing number of reports have demonstrated Bet v 1-specific T lymphocyte reactions with related food homologues.231213 Jahn-Schmid and colleagues3 showed that T lymphocytes specific for the Bet v 1142-156 epitope were triggered to produce cytokines and proliferate in response to homologous pathogenesis-related (PR)-10-like allergens such as Api g 1, Cor a 1, Dau c 1, Gly m 4, Pru av 1, and Mal d 1. Furthermore, Schimek and colleagues13 demonstrated that digested Bet v 1-related food allergens (non-IgE-binding fragments) are able to induce proliferation and cytokine secretion in Bet v 1-specific T cells. This strong evidence in the literature indicates that T cell-mediated reactions against Bet v 1 may also occur in the absence of IgE binding and IgE-mediated reactions in birch pollen allergy patients. Therefore, pollen-related foods should be considered important stimuli for pollen-specific T cells in patients without immediate clinical symptoms of food allergy. Moreover, the fact that the atopy patch test (APT) may be the only positive test in patients emphasizes the importance of including the APT in the allergy diagnostic workflow. In other words, patients with negative specific IgE (sIgE) or skin prick test (SPT) results that do not receive a follow-up APT may be incorrectly diagnosed as non-allergic.14
Previously, we evaluated the allergenicity of 11 apple cultivars and showed that Bet v 1 sensitization plays a substantial role in the allergic response to the tested apple cultivars in relation to oral allergy syndrome (OAS) status.4 In the medical literature there is lack of studies describing observations of late reactions to apples in patients sensitized to the Bet v 1. To address this, in a follow-up study we recruited 45 patients with birch pollen allergy and evaluated the concomitance of delayed-type hypersensitivity reactions (type IV immunologic reactions) and immediate IgE-mediated type I reactions against apples.
Go to : 
MATERIALS AND METHODS
Subjects
The study group included 45 birch-pollen allergic adult subjects. Patients were eligible for participation in the study based on a positive history of birch pollen allergy, the occurrence of clinical manifestations of allergic rhinitis/rhinoconjunctivitis during tree pollen season, a positive SPT with birch extract and the presence of specific IgE to birch pollen (Bet v 1). The mean age of patients was 29 years (range 17–52 years). All subjects were interviewed and completed the pollen-food allergy syndrome questionnaire (ALK-Abelló Poland SP. z.o.o., Krakow, Poland), which assessed typical adverse reactions after fruit and vegetable consumption including OAS symptoms. Patients meeting the inclusion criteria (45 subjects) were examined for immediate and late allergic reactions by APTs and SPTs with fresh apples pulp. The study was approved by the Bioethics Committee of the Regional Medical Chamber in Lodz (No. RNN/731/11).
SPT procedures
A total of 45 subjects with clinical symptoms of birch pollen allergy were confirmed by SPTs as previously described.4 Tests were performed according to a standard procedure with standard birch extract (Betula alba, 50.000 SBE/mL; Allergopharma, Reinbek, Germany) with histamine dihydrochloride (1.7 mg/mL) as a positive control and SPT diluents (0.9% natrium chloride) as a negative control. The SPT results were regarded as positive when the diameter of the wheal was 3 mm or larger.
SPTs with fresh apples (prick by prick test) were performed shortly after harvesting using apple material obtained from the pulp of the apple. Apple material was obtained from the middle area of the fruit, approximately 3 cm below the stem. Tests were performed similarly as described above for the SPT procedure with birch pollen extract.
Specific IgE measurement
Serum sIgE antibodies against Bet v 1 and Mal d 1 were measured by the radioallergosorbent test using ImmunoCAP and the Pharmacia ImmunoCAP 250 analyzer (Pharmacia, Stockholm, Sweden) according to the manufacturer's instructions.
APT procedure
APTs were performed based on the European Task Force on Atopic Dermatitis (ETFAD) standardized APT technique with modifications.15 Finn chambers on Scanpor filled with fresh apple pulp slices (approximately 1 cm2 of Golden Delicious or Grey French Reinette) were applied on patients' upper backs for 48 hours. Readings were performed at 48 and 72 hours. The APT reaction on the skin was evaluated in relation to healthy non-tested upper back skin.
Statistical analysis
The strength and direction of the linear relationship between variables (SPT results, sIgE Bet v 1, and sIgE Mal d 1) were evaluated via adjusted Pearson's correlation coefficient (radj), calculated using statistical formula described by Yehia and colleagues16 with the aid of GraphPad 5 software (GraphPad Software, Inc., La Jolla, CA, USA).
Go to :
RESULTS
We studied the immediate and late allergic reactions of patients to high- and low-allergenic apple cultivars (accordingly, Golden Delicious and Grey French Reinette) using SPTs and APTs. The highest incidence of immediate reaction was found for Golden Delicious (87%), while Grey French Reinette (Szara Reneta) accounted only for 56% of SPTpositive results to tested apples. Within the study group 25 patients experienced OAS according to detailed pollen-food allergy syndrome questionnaire. Further examination of patients via APTs revealed that 4 patients developed delayed hypersensitivity reactions to either Golden Delicious or Grey French Reinette apples (9% of examined group); these reactions manifested clinically as erythema with papules (class ++) (Table 1). Interestingly, all APT-positive patients were also diagnosed with OAS after detailed interview. Two APT-positive patients (patients #1 and #4) were concomitantly SPT-negative for Golden Delicious and Grey French Reinette apples. One patient (patient #3) exhibited positive SPT/APT reactions for both high- and low-allergenic apple cultivars. In addition, although both patients #1 and #4 were SPT-negative for Golden Delicious and Grey French Reinette apples, a detailed examination of APT-positive patients using SPTs with other available apple cultivars indicated that allergic late reactions developed irrespective of SPT results to tested apples and their allergenicity status (data not shown). These observations are in line with observed sIgE levels for Bet v 1 and Mal d 1. Both SPT-positive/APT-negative and SPT-positive/APT-positive patients exhibited similar patterns of serum specific IgE concentration (accordingly, 28.15 kU/L and 33.09 kU/L for Bet v 1; 7.4 kU/L and 5.32 kU/L for Mal d 1). Next, we investigated the relevance of Bet v 1 sensitization in the development of the immediate reactions to apples. As expected highly allergenic cultivar Golden Delicious, but not Grey French Reinette, showed a correlation between SPT results and patient blood levels of Bet v 1-sIgE (radj=0.490, P<0.001; Table 2). Finally, we observed no correlation of SPT results to apples with patient blood levels of Mal d 1-sIgE for both apple cultivars (radj=0.110 and radj=0.072; Table 2). Interestingly, comparing levels of sIgE for Bet v 1 and Mal d 1 revealed a positive correlation between them and indicated that levels of these antibodies were related (radj=0.682, P<0.001). Finally, we performed correlation analyses in the APT-positive group. As shown in Table 2, we observed that sIgE levels for Bet v 1 and Mal d 1 were unequivocally negatively correlated with SPT results to apples in APT-positive patients. Interestingly, the association between Bet v 1-sIgE and Mal d 1-sIgE levels was preserved (radj=0.998; Table 2).
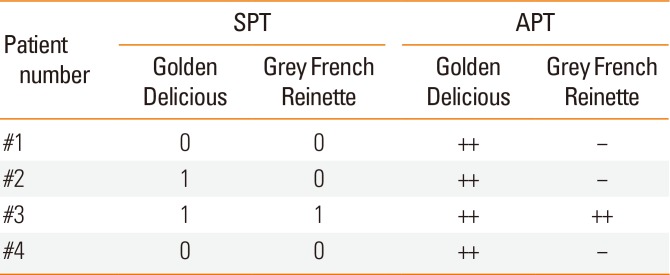

Table 1
Immediate and late allergic reactions to high- and low-allergenic apples in patients APT positive for apple (n=4)
| Patient number | SPT | APT | ||
|---|---|---|---|---|
| Golden Delicious | Grey French Reinette | Golden Delicious | Grey French Reinette | |
| #1 | 0 | 0 | ++ | - |
| #2 | 1 | 0 | ++ | - |
| #3 | 1 | 1 | ++ | ++ |
| #4 | 0 | 0 | ++ | - |
![]()
Table 2
Correlations between SPT results to apples and sIgE for Bet v 1/Mal d 1, between sIgE Bet v 1 and sIgE Mal d 1 in groups of patients APT-positive/negative for apple (radj/Pvalue)
![]()
Go to :
DISCUSSION
Bet v 1 (PR-10 class) is assumed to be the primary sensitizing agent, and the Bet v 1-specific IgE subsequently cross-react with apple Mal d 1 and elicit an allergic response as reflected by the clinical observation that an apple allergy develops only after the onset of birch pollinosis.17 In addition, several scientific reports indicate that T cell-mediated reactions toward PR-10 allergens may also occur in the absence of IgE binding and IgE-mediated reactions in patients allergic to birch pollen. T cells sensitized with a dominant epitope for Bet v 1142-156 were shown to produce cytokines and proliferate in response to homologous PR-10-like allergens.313 In addition, late eczematous reactions in patients with birch pollen allergy have been associated with Bet v 1-specific T cell responses in isolated skin lessions.12 Therefore, pollen-related foods should be considered important stimuli for pollen-specific T-cells in patients without immediate clinical symptoms of food allergy. To our knowledge, delayed hypersensitivity to apple has not yet been discussed in the context of the apple and birch cross-reactivity in scientific literatures.
In this work, we assessed the incidence of allergic late-phase reactions to apples among patients with birch pollinosis. We examined the reactions of 45 patients to high- and low-alergenic apple cultivars using SPTs and APTs to evaluate the involvement of IgE- and non-IgE-mediated reactions to the apple challenge. SPT/APT with fresh food that contains native allergens is widely accepted as a clinical tool for the assessment of sensitization to a particular food.18 Within the group of examined patients, the incidence of immediate reaction was 1.5-fold higher for Golden Delicious than for Grey French Reinette (87% vs 56%). These results are in line with those of our previous study, which indicated that Grey French Reinette was the least allergenic cultivar among 11 tested.4 In contrast to the reactions to Golden Delicious, the patients' SPT reactions to Grey French Reinette were neither related to Bet v 1- nor to Mal d 1-sIgE status. According to the study of Kitzmüller and colleagues,19 patients with birch pollinosis and associated apple allergy exhibit a higher concentration of sIgE to Bet v 1 than sIgE to Mal d 1 (3.4-fold). Notably, the results of our study showed similar sIgE characteristics and indicated that Mal d 1-sIgE levels were 4-fold lower than Bet v 1-sIgE levels (28.15 vs 7.4 kU/L). Furthermore, the levels of Bet v 1- and Mal d 1-sIgE were positively correlated, which is a characteristic feature of Bet v 1-driven pollen-food syndrome.
The APT has been described as a diagnostic procedure to assess delayed-type hypersensitivity against allergens known to elicit IgE-mediated reactions. Although the APT has primarily been established as a model for early AD lesions, it has been found to be a valuable tool for the diagnosis of food allergies.18 The endpoint of an allergen-induced positive APT reaction is characterized by infiltration of Th1/Th2 lymphocytes followed by inflammatory dendritic epidermal cells and closely resembles the early stages of AD lesions.202122 Numerous studies have shown that the APT method may be found more specific and sensitive than SPT or sIgE in the diagnosis of delayed-type food allergy in children.1823 In comparison to SPTs, the APT may even detect relevant sensitization in the absence of a specific IgE response.22 Recently, studies by Fuiano and colleagues24 have further expanded the clinical importance of the APT by demonstrating that this test is also positive in patients with respiratory allergies. In an unselected paediatric population in Southern Italy, 12.5% of subjects had a positive APT result, indicating the importance of including this test in the diagnostic workup of respiratory allergies. Following this proof of concept, in the present study we evaluated the incidence of delayed-type hypersensitivity reactions to apple by testing 45 individuals who were allergic to birch pollen with an APT using fresh apple pulp. Our study showed for the first time that contact of apple pulp with skin may elicit a delayed reaction that clinically manifests as erythema with papules. Four patients (9% of the examined group) developed a clear-cut type IV immunological response with class ++ intensity. Interestingly, 9% (6/65 subjects) of children from the Fuiano study that were SPT-positive for plant pollens (Cypress, Compositae, Grass and Parietaria) were also APT-positive.24 According to our observations, positive allergic late reactions to apple developed irrespective of SPT results to apples and their allergenicity status. Only 50% of subjects who were APT-positive for Golden Delicious apples were concomitantly SPT-positive for apple. In other words, a positive SPT reaction to apple is not a prerequisite for the development of a delayed skin hypersensitivity reaction to a particular apple cultivar. Interestingly, we also observed concomitant OAS symptoms in all 4 patients who developed skin delayed hypersensitivity reaction to apple, though OAS is a clinical manifestations of local IgE-mediated allergy reaction to ingested apple that include itching and swelling of the lips, tongue and throat. Since, all examined patients were confirmed allergic to birch pollen and sIgE-positive for Bet v 1, the experienced symptoms of OAS must have been associated with cross-reaction of ingested apple Mal d 1 allergen with sIgE against Bet v 1, known as pollen-food syndrome. In addition to the humoral cross-reactivity between Bet v 1- and Mal d 1-sIgE, cross-reactivity at the T cell level between T lymphocytes specific for Bet v 1142–156 and related food allergens of the PR-10 protein family (Api g 1, Cor a 1, Dau c 1, Gly m 4, Pru av 1 and Mal d 1) has been also showed in vitro (proliferation of specific T cells and synthesis of IL-4 and IL-5).3 Moreover, presence of a high percentage of individuals with birch pollen allergy that harbor T-cells specific for Bet v 1142-156 in their blood implies that such similar cross-stimulation might also occur in vivo.3 Thus, according to our study results and literature data, it is likely that observed APT reaction to apples in patients might be related to preliminary induction of Bet v 1-specific TH cells by birch pollen, and then subsequent stimulation of Bet v 1-primed T cells with homologue apple Mal d 1 allergen after skin apple pulp contact. Altogether, we suggest that observed positive SPT and APT reactions to apple among birch pollen allergic patients in the present study are associated, at least in part, with their particular initial sensitization to Bet v 1 at humoral and cellular levels, and cross-reactivity with homologue Mal d 1. Finally, our study demonstrated that APT may be the only positive test in patients with allergy and highlights the importance of including an APT test in the diagnostic workup for allergies. Indeed, several observations from clinical studies confirm that the APT may provide positive results in concordance with the SPT but may also be the only positive test.24252627 Apart from diagnostic value of APT to apple, the results of our study also suggest that patients diagnosed as APT-positive with apple might potentially suffer from gastrointestinal distress associated with delayed hypersensitivity reaction after apple digestion. Therefore, the clinical relevance of APT-positive diagnosis to apple should be further evaluated by patients itself by employing apple elimination/challenge diet and watching for any gastrointestinal symptoms (diarrhea, nausea, flatulence, or constipation) and/or skin reactions (e.g., pruritus, eczema).
In summary, this study provides the first clinical evidence of delayed-type hypersensitivity reactions to apples among patients with birch pollinosis. Our survey demonstrated a 9% incidence of late phase allergic responses to apples in Polish patients, indicating the clinical relevance of this outcome in food allergy diagnostics. We believe that a combination of skin prick and atopy patch testing might significantly improve the identification of food allergies to apples.
Go to :
 XML Download
XML Download