

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cardiac metastases occur more frequently than primary cardiac tumors, with a highly variable incidence ranging from 2.3% to 18.3% in autopsy reports.1) Although in theory, any malignant tumor can metastasize to the heart, the most common tumors showing cardiac metastatic potential are lung cancer, breast cancer, hematologic malignancies and malignant melanoma.2)3)4)5) Whole-body oncologic positron emission tomography/computed tomography (PET/CT) using 2-[18F]-fluoro-2-deoxy-D-glucose (FDG) is a useful imaging tool for cancer detection and staging that assesses tumor metabolic activity.6-8) However, cardiac uptake of 18F-FDG on PET/CT has been overlooked due to intense physiological myocardial FDG uptake and numerous benign conditions.9)10)11)12)
Transthoracic Doppler echocardiography (TTE) has been widely used as an initial imaging modality to provide information on hemodynamic consequences and the presence of cardiac metastases.13)14)15)16) To the best of our knowledge, there have been no studies comparing cardiac or pericardial 18F-FDG uptake on PET/CT with findings on TTE in patients with non-cardiac malignancy. The aim of this study is to investigate echocardiographic features corresponding to cardiac or pericardial 18F-FDG uptake on whole-body oncologic PET/CT.
METHODS
Study population
Forty-three consecutive patients (32 men, 11 women; mean age, 62 ± 19 years) with newly diagnosed non-cardiac malignancy showing cardiac or pericardial 18F-FDG uptake on oncologic whole-body PET/CT who underwent TTE within 1 month of PET/CT were retrospectively reviewed. The present study was approved by the Institutional Review Board and conducted with ethical principles of the Declaration of Helsinki. Written informed consent was obtained from all patients before enrollment.
The primary tumors of all patients were histopathologically confirmed by analysis of surgically resected tumor or tumor biopsies. Patients with previous history of primary cardiac tumor or cardiac surgery, coronary artery disease, atrial fibrillation, significant valvular heart disease, chronic obstructive pulmonary disease, acute infection or sepsis and poor image quality were excluded.
18F-FDG PET/CT scanning
All scans were obtained using an integrated PET/CT inline system, either Biograph Duo or Biograph TruePoint (Siemens Medical Solutions, Knoxville, TN, USA). All patients fasted for at least 6h before the PET/CT study. Approximately 1h before PET/CT, each patient received an injection of 370-555 MBq of 18F-FDG. No patients had blood glucose levels > 130 mg/dL before the injection. There were 6-8 bed positions, and acquisition time was 2-3 min per bed position. Non contrast-enhanced CT was performed from the base of the skull to the upper thighs for attenuation correction and diagnosis (130kVp, 80mA, and 5-mm slice thickness; 120kVp, 50mA, and 5-mm slice thickness). PET immediately followed over the same body region, and images were reconstructed using a standard ordered-subset expectation maximization (OSEM) algorithm. The axial spatial resolution was 6.5 or 4.5mm at the center of the field of view.
Image analysis
All PET/CT images were reviewed at a workstation with fusion software (Syngo; Siemens Medical Solutions, Knoxville, TN, USA) that provided multi-planar reformatted images and displayed PET images after attenuation correction, CT images, and PET/CT fusion image. CT images were used to identify the location and morphological features of the lesion, in addition to its relation to surrounding tissues. 18F-FDG uptake in cardiac and pericardial lesions was quantified by calculating the maximum standardized uptake values (SUVmax), which were obtained by normalizing the tissue concentration of FDG activity and patient weight. All PET/CT scans were reviewed and interpreted by 2 board certified nuclear medicine physicians who were blinded to the clinical data and the applied imaging convention.
TTE
All ultrasound examinations were performed with a commercially available echocardiographic device (vivid 7 [GE Vingmed Ultrasound AS, Horten, Norway], with a 2.5-MHz phased array probe). Standard M-mode, two-dimensional (2D), and color Doppler measurements were obtained according to the American Society of Echocardiography (ASE) recommendations.17)18)19) Briefly, echocardiographic data included morphology, size, location and echogenicity of metastatic lesions. Pericardial thickness greater than 4mm was defined as pericardial thickening. Left ventricular (LV) wall thickness and chamber dimension were measured from 2D-guided M-mode echocardiography. Regional LV myocardial wall motion was visually estimated by examining LV myocardial wall thickness and was classified as normal (normal wall thickening and motion), hypokinesia (reduced wall thickening and motion), and akinesia (absence of wall thickening and motion). Respiratory variation of ≥ 25% in mitral inflow peak early (E) velocity with abnormal septal notching or abrupt diastolic flattening of the posterior wall was considered diagnostic of constrictive pericarditis. Pulmonary venous (PV) velocities were also recorded, and monophasic flow or flow velocities > 1.6 m/s were regarded as functionally significant obstructions. Right ventricular (RV) chamber dimension and wall thickness were measured from the apical four-chamber view and subcostal view, respectively. All echocardiographic examinations were performed by skilled sonographers and interpreted by experienced cardiologists who were blinded to clinical information of the study population.
Statistical analysis
Data were analyzed using SPSS 18 software (SPSS, Inc., Chicago, IL. USA). Continuous variables were presented as the mean ± standard deviation (SD), and categorical data were presented as frequency percentages. Group comparison of mean SUVmax was performed by Mann-Whitney U test. A p value < 0.05 was considered statistically significant.
RESULTS
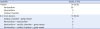
Among 43 patients with cardiac or pericardial 18F-FDG uptake on PET/CT, the most frequent site of primary tumor was lung (15/43, 34.9%), followed by lymph node (8/43, 18.6%), thyroid (4/43, 9.3%), breast (3/43, 7.0%), liver (3/43, 7.0%), stomach (2/43, 4.7%), pleura (2/43, 4.7%) and five other sites (chronic myeloid leukemia [CML], mediastinum, esophagus, ovary, and metastasis of unknown origin [MUO]). Of 15 patients with lung cancer, 10 patients (66.7%) had non-small cell lung carcinoma (five each cases of adenocarcinoma and squamous cell carcinoma) and five (33.3%) had small cell lung carcinoma. All patients with lymphoma had non-Hodgkin's lymphoma (diffuse large B-cell lymphoma in six patients and T cell lymphoblastic lymphoma in two patients). Thyroid cancer was follicular carcinoma in three patients and anaplastic carcinoma in one patient. All three cases of breast cancer were invasive ductal carcinoma. The stomach cancer was adenocarcinoma and the pleural tumor was mesothelioma (Table 1).
Table 1
Pathology of primary non-cardiac malignant tumors in 43 patients with cardiac or pericardial fluorodeoxyglucose uptake on whole-body 18F-fluorodeoxyglucose positron emission tomography-computed tomography

![]()
FDG uptake in the heart
Although primary tumors tended to have a higher mean SUVmax than those of metastatic lesions in the heart, the difference was not statistically significant (Figure 1). Of 43 patients, 33 patients (75.0%) had only one metastatic FDG uptake, including the pericardium in 29 patients, myocardium in three patients, and cardiac chamber in one patient. Among the rest, there were seven cases (16.3%) with FDG uptake in two sites (cardiac chamber and great vessel in five patients, pericardium and myocardium in two patients) and three cases (6.9%) with FDG uptake in three sites (myocardium, cardiac chamber, and great vessels in two patients, and pericardium, cardiac chamber, and great vessel in one patient) (Table 2).
 | Figure 1Comparison of mean SUVmax between primary tumor and metastatic cardiac FDG uptake. FDG: fluorodeoxyglucose, HCC: hepatocellular carcinoma, SUVmax: maximum standardized uptake value.
|
Table 2
Location of cardiac or pericardial fluorodeoxyglucose uptake on 18F-fluorodeoxyglucose positron emission tomography-computed tomography
![]()
Echocardiographic features of metastatic FDG uptake lesions
Among study population, pericardial effusion was the most common echocardiographic finding (22/43, 51.2%) in concordance with 18F-FDG uptake on PET/CT. Table 3 shows echocardiographic features according to the site of FDG uptake. Examples of each site are shown in Figure 2.
Table 3
Echocardiographic features according to the location of FDG uptake on 18F-FDG positron emission tomography-computed tomography

18F-FDG: 18F-fluorodeoxyglucose, IVC: inferior vena cava, PV: pulmonary vein, SVC: superior vena cava. *Intrapericardial mass or materials, pericardial thickening, decreased sliding motion of the pericardium, constrictive pericarditis. †Disturbance of SVC, IVC or PV inflow.
![]()
 | Figure 2Cardiac and pericardial FDG uptake on whole body oncologic PET/CT and their echocardiographic features. (A) A 69-year-old man with multifocal pericardial FDG uptakes on PET/CT (left). TTE showed RV pericardial echogenic mass protruding into the RV and RA (right, arrow) with RV free wall hypokinesia and compressed RA by the pericardial mass (right, arrow head). (B) A 52-year-old man with focal FDG uptake and central photon defect in IVS on PET/CT (left). TTE revealed a round, homogeneous and hyperechogenic protruding mass on IVS with hypokinetic wall motion (right, arrow). (C) A 69-year-old man with intense FDG uptakes involving RA and IVC on PET/CT (left). TTE demonstrated a round, echogenic mass with irregular margin attached to the septum of the RA side (right upper) that is linked to an irregular heterogeneous echogenic mass from the IVC, showing flow acceleration at IVC entrance (Vmax = 1.8 m/s) (right lower). FDG: fluorodeoxyglucose, IVC: inferior vena cava, IVS: interventricular septum, PET/CT: positron emission tomography/computed tomography, RA: right atrial, RV: right ventricular, TTE: transthoracic Doppler echocardiography.
|
Of 32 patients with pericardial FDG uptake, 25 patients (78.1%) showed pericardial abnormalities including pericardial effusion (88.0%), intrapericardial mass or materials (40.0%), pericardial thickening (36.0%), hyperechogenicity of the myopericardium (24.0%), decreased sliding motion of the pericardium (12.0%), and constrictive pericarditis (8.0%). Despite only two cases showed pericardial and myocardial FDG uptakes simultaneously, 6 patients (18.8%) demonstrated myocardial abnormalities such as regional wall motion abnormality (RWMA) (66.7%) and increased myocardial wall thickness (33.3%). Of 29 cases with FDG uptake limited to the pericardium, 17 cases (58.6%) showed pericardial abnormalities on TTE and their mean SUVmax was not significantly different from that of others with normal echocardiogram (n=7) (7.4 ± 4.7 vs. 6.4 ± 4.8, p = 0.684) (data not shown). When comparing the mean SUVmax of pericardial FDG uptake lesions according to the type of abnormal echocardiographic features, lesions with RWMA (14.3 ± 4.7 vs. 6.4 ± 4.0, p = 0.004) or constrictive pericarditis (13.1 ± 3.4 vs. 6.6 ± 4.1, p = 0.021) had significantly higher mean SUVmax than those without. Furthermore, lesions showing pericardial thickening (8.4 ± 6.1 vs. 6.8 ± 4.1, p = 0.433) or increased pericardial echogenicity (10.1 ± 5.9 vs. 6.7 ± 4.3, p = 0.138) were more likely to have higher mean SUVmax. However, the presence of pericardial effusion or intrapericardial materials was not associated with mean SUVmax (Figure 3).
 | Figure 3Comparison of mean SUVmax at isolated pericardial FDG uptake lesions with and without echocardiographic abnormal features (n = 29). *p = 0.004, †p = 0.021. FDG: fluorodeoxyglucose, RWMA: regional wall motion abnormality, SUVmax: maximum standardized uptake value.
|
Of seven cases with myocardial 18F-FDG uptake, 6 patients (85.7%) revealed pericardial abnormalities such as pericardial effusion (66.7%), hyperechogenicity of the myopericardium (33.3%), and others (Intrapericardial mass or materials, pericardial thickening, decreased sliding motion of the pericardium, constrictive pericarditis in one patient each). Among 5 patients showing myocardial abnormalities on TTE (71.4%), RWMA in 4 cases (80.0%) and increased myocardial wall thickness in 3 cases (60.0%) were found.
All nine cases with cardiac chamber 18F-FDG uptake revealed a mass in the cardiac chambers including the RA (6/9, 66.7%), RV outflow tract (1/9, 11.1%), RV (1/9, 11.1%), and LA (2/9, 22.2%) on TTE. Eight cases with great vessel 18F-FDG uptake included disturbances of SVC, IVC, or PV inflow in 5 cases (62.5%), pericardial effusion in 3 cases (37.5%), and intracardiac mass in 3 cases (37.5%). FDG uptake confined to the great vessels was not found.
DISCUSSION
18F-FDG uptake reflects glucose metabolism, and its uptake on PET/CT has been widely used as an imaging biomarker for cancer detection in oncology.6)7)8) Knowledge of pathological cardiac and pericardial FDG uptake on whole body PET/CT may provide important diagnostic clues to rule out metastatic involvement of the heart in patients with cancer or cancer screening.20) Here, we demonstrated for the first time echocardiographic features in concordance with cardiac and pericardial FDG uptakes that are incidentally encountered on oncology PET/CT among patients with non-cardiac malignancy.
Prior studies reported that the differentiation of focal pericardial FDG uptake from paracardiac lymph node uptake by 18F-FDG PET image is difficult.12) In this study, all but two patients showed focal pericardial FDG uptake, and we could exclude paracardiac nodal disease through FDG PET/CT fusion image. Pericardium was the most common site of FDG uptake however, only 60% of them revealed abnormal echocardiographic features and their mean SUVmax was similar with that of normal echocardiogram. Although normal FDG uptake in the heart was adequately suppressed by prolonged fasting, the possibility of physiologic uptake or inflammation could not be completely excluded in our study. This result shows the limitation of oncology PET/CT for detecting cardiac metastasis, and also suggests that interpretation of cardiac FDG uptake, particularly in pericardium, should be cautious. Furthermore, we found that pericardial FDG uptake showing RWMA and constrictive pericarditis on TTE were more likely to have higher mean SUVmax compared to other echocardiographic features. These findings seem to be inconsistent with previous reports demonstrating reduced FDG uptake in lesions of RWMA on TTE. However, most studies have been conducted in patients with coronary artery disease for assessing myocardial viability using cardiac PET/CT protocol.21)22) Considering that FDG uptake is related to metabolism, increased FDG uptake showing RWMA on TTE may strongly suggest cardiac metastasis. Accordingly, it is thought that aforementioned abnormal echocardiographic features reflecting hemodynamic impairment could provide important clinical clues for metastatic pericardial FDG uptake.
It is difficult to detect malignant myocardial FDG uptake on oncology PET/CT because physiologic variations in FDG uptake can obscure abnormal myocardial FDG uptake.9)11) However, we used a strict preparation fasting regimen and excluded common patterns of normal physiologic FDG activity in the myocardium. In the present study, echocardiographic abnormalities were identified in all seven patients with myocardial FDG uptake. Interestingly, patients with myocardial FDG uptake alone showed not only myocardial structural or functional abnormalities but also pericardial abnormalities. These findings suggest that myocardial FDG uptake on oncology PET/CT could be a pathologic finding showing abnormal pericardial or myocardial abnormalities on TTE.
Most cases of FDG uptake in cardiac chambers on oncology PET/CT accompanied by involvement of the great vessels including the SVC, IVC, or PV, and some of them (7/9, 77.8%) also exhibited venous inflow disturbance on TTE. Considering that metastatic masses were usually located in RA or LA, our results suggest intracavitary cardiac metastases through a transvenous route. Echocardiography may be helpful to understand hemodynamic condition of these patients. Intracavitary space-occupying growth of a secondary heart tumor is rare, and it has been mainly reported in cancers of the kidney, liver, lung and thyroid.1)23) Meanwhile, in our study, involvement of the cardiac chambers and/or great vessels was most frequently found in lymphoma. This seems to be related to the pathophysiology of lymphoma that can metastasize to the heart through hematogenous dissemination,24) along with relatively high proportion of lymphoma in our study population.
Our study has several limitations. First, this is a retrospective study with potential selection and information biases. Second, there was no comparison with other adjunctive imaging modalities such as CT or MRI. Finally, all cardiac and pericardial FDG uptake lesions were not confirmed by pathology. Risks related to myocardial biopsy limit their routine use in clinical practice, especially for cancer patients. Moreover, it is challenging to capture a small piece of affected cardiac tissue. Thus, clinical data was acquired and analyzed to rule out benign cardiac or pericardial lesions with increased FDG uptake on PET/CT.
In conclusion, echocardiographic abnormality for cardiac or pericardial 18F-FDG uptake on oncologic PET/CT is not uncommon, and its echocardiographic features differ according to which heart sites are involved. Echocardiography may provide incremental morphologic and hemodynamic information in combination with anatomic and metabolic data obtained by FDG PET/CT. Further longitudinal prospective studies with a larger sample size are needed to establish the optimal imaging approach for increased FDG uptake in the heart during cancer staging.
 XML Download
XML Download