

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Accurate classification of stroke etiology is crucial for optimizing stroke management.1) Cardio-embolic stroke is the most frequently predicted cause of cryptogenic stroke; the most frequent cause of cerebral cardio-embolism is atrial fibrillation (AF), including paroxysmal AF.2) AF is the most common etiology of ischemic stroke; the incidence of stroke in individuals with non-valvular AF is estimated to be 5 times higher than in individuals without AF.3) The prevalence of AF in the whole stroke population has been reported to range from 17%−25.6%.4)5) The risk for stroke and thromboembolism in patients with AF has been shown to escalate proportionally with combined vascular risk factors.6)7) However, by routine arrhythmia screening methods, it is difficult to detect the short and usually asymptomatic presentations of paroxysmal AF (also called occult AF).
There is evidence that abnormal levels of plasma free fatty acids (FFAs) are associated with an increased risk of myocardial disease, including AF and heart failure.8)9) Adipose tissue covers a significant portion of the epicardial surface,10) and myocyte-adipocyte cross linking is known to be important in the physiological function of the normal myocardium.11) Myocardial injury and ischemia are followed by changes in the levels of adipocyte-derived biomarkers (FFAs and adipokines) and adipose deposition.12)13) Fat can accumulate around the heart in epicardial adipose tissue or inside the heart as lipid droplets.14) The mechanism by which fatty infiltration promotes arrhythmogenicity is not well characterized.15) Recent studies have shown that increased epicardial adiposity can directly modulate the electrophysiological properties of the heart and ion currents, causing higher arrhythmogenesis in left atrial myocytes, which contributes to an increased risk of AF.16)17)
Epicardial fat is a metabolically active tissue; echocardiography is a useful technique for measuring epicardial fat thickness (EFT).18) Previous studies have demonstrated associations between EFT and coronary artery disease, carotid atherosclerosis, metabolic syndrome, and obesity.19)20)21)22) In addition, increased EFT has been shown to be associated with the presence and chronicity of AF.23)
However, the potential association between EFT and FFA plasma level in ischemic stroke with or without AF has not been previously investigated. The objective of this study was to assess the performance of EFT and plasma FFA level in identifying patients with ischemic stroke and AF.
METHODS
We retrospectively included patients with acute ischemic stroke who were admitted within 3 days of symptom onset to a single university hospital between March 2011 and June 2014. We defined acute ischemic stroke as new focal or global neurological deficits with evidence of acute cerebral infarction on magnetic resonance imaging (MRI). Patients with chronic congestive heart failure, surgery within 60 days, infection, malignancy, rheumatologic disorder, immunological disorder, chronic renal insufficiency, acute coronary syndrome within 30 days before admission, mitral valve disease, and patent foramen ovale were excluded. In addition to the epidemiologic variables age and sex, classic cardiovascular risk factors were also considered. Old age was defined as > 65 years; hypertension was defined as systolic blood pressure (BP) > 140 mmHg and diastolic BP > 90 mmHg by repeated BP measurement or previous diagnosis; and diabetes mellitus (DM) was defined as a fasting plasma glucose level ≥ 126 mg/dL in 2 consecutive assessments or current treatment for DM. The presence of dyslipidemia was assumed if subjects were taking lipid-lowering drugs or had a high total cholesterol level (> 200 mg/dL). This study complies with the Declaration of Helsinki and was approved by the Institutional Review Board of our institution.
Laboratory measurements
Venous blood was drawn the morning after an overnight fast on the first hospitalized day. The following parameters were obtained by standard techniques on the examination day: total cholesterol, low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), triglycerides, high sensitivity C-reactive protein (hs-CRP), and fibrinogen. Plasma FFA was measured by the enzymatic colorimetric method. Specifically, the NEFA-HR (2) reagent kit (Wako Pure Chemical Industries, Osaka, Japan) was used to quantitatively determine FFA level (Hitachi 7600 Automatic Analyzer, Hitachi-High-Technologies Corporation, Nishi-Shimbashi 1-chome, Minato-ku, Tokyo, Japan). Height and weight were measured and used to calculate body mass index (BMI, kg/m2).
Identification of AF
Electrocardiographs (ECGs) of all selected patients were reviewed. Patients with a sinus rhythm were placed on 24-48 hour Holter monitoring to monitor for paroxysmal AF. Subjects with 12-lead ECGs demonstrating AF or arrhythmia > 30 seconds in duration on Holter monitoring or telemetry recordings were considered to have AF.
Neurologic assessment
All patients with stroke underwent computerized tomography (CT) scans of the brain followed by MRI. CT angiography or magnetic resonance angiography of the brain and neck was also performed for all patients with stroke. Ischemic stroke was classified as large-artery atherosclerosis, cardioembolism, small-vessel occlusion, stroke of other determined etiology, or stroke of undetermined etiology, according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria.24) Stroke severity on admission was assessed by a stroke neurologist using the Korean version of the National Institutes of Health Stroke Scale (NIHSS).25) Functional outcomes were measured at 3 months after stroke onset using the modified Rankin Scale (mRS).26)
Echocardiographic measurement
Standard two-dimensional and strain echocardiography scans were performed on all patients using a 3.5-MHz transducer (Philips iE33, Philips Medical Systems, Bothell, WA, USA). The scans were acquired with the patient in the left lateral decubitus position. All echocardiography examiners were blinded to patient information. Measurements of the thickness of the interventricular septum and posterior wall, the diameter of the left atrium (LA), left ventricular (LV) cavity, and the LV mass index (LVMI) were performed according to the American Society of Echocardiography criteria.27) Pulsed wave Doppler of the transmitral LV inflow was performed in an apical 4-chamber view with the sample volume placed at the level of the mitral valve tips. The following measurements of global LV diastolic function were determined: peak early (E) and late (A) diastolic mitral flow velocity, ratio of E and A, E/A; early (Ea) diastolic mitral annular velocity; deceleration time of the E wave; and LV isovolumetric relaxation time (IVRT).
EFT was measured perpendicular from the free wall of the right ventricle at end-systole in three cardiac cycles according to a method we previously described.28) Epicardial fat was defined as the echo-free space between the outer wall of the myocardium and the visceral layer of the pericardium. The maximum EFT was measured from the point on the free wall of the right ventricle along the midline of the ultrasound beam perpendicular to the aortic annulus as the anatomic landmark. Since a critical issue in EFT measurement is inconsistency of the measurement location, the mean EFT was averaged from the parasternal long axis and parasternal short axis view images. Offline measurement of EFT was performed by two cardiologists who were blinded to the clinical data. Measurement of EFT was performed at least twice to ensure high reliability. The intra-observer and inter-observer variability values of EFT were 3.2% and 5.6%, respectively.
Statistical analysis
Statistical analyses were performed using SPSS 18.0 for Windows (SPSS Inc., Chicago, IL, USA) and R (http://www.r-project.org). Observed values of continuous and discrete variables were summarized as mean ± standard deviation or as frequency with percentage (%), respectively. The normality assumption was validated using the Kolmogorov–Smirnov test. For continuous variables, mean differences between patient groups (without and with AF) were compared using Student's t-test; differences between categorical variables were compared using the Chi-square test. Multivariable logistic regression models were employed to identify variables independently associated with ischemic stroke with AF. To avoid potential multi-collinearity issues, we performed variable selection in a stepwise fashion. The Hosmer-Lemeshow test and C-index were utilized to evaluate the calibration and discriminability of logistic regression models, respectively.29) Utilizing likelihood ratio tests and Delong's tests,30) we compared the goodness-of-fit and discriminability of four different logistic regression models: Model 1, which includes age; Model 2, which extends Model 1 with EFT; Model 3, which extends Model 1 with FFA; and Model 4, which extends Model 1 with EFT and FFA. p-values less than 0.05 were considered statistically significant.
RESULTS
Comparison of clinical and echocardiographic characteristics in the ischemic stroke groups with or without AF
The baseline characteristics between patients with stroke with or without AF are shown in Table 1. Patients with ischemic stroke with AF (n = 35) were older, more likely to be female, and had higher prevalence of coronary artery disease and heart failure. In the patients with AF, the mean AF duration was 13.5 months, and the subtypes included paroxysmal AF (34.3%) and non-paroxsymal AF (persistent and chronic AF, 65.7%). Regarding the laboratory data, patients with ischemic stroke with AF showed significantly higher serum FFA level (1379.7 ± 717.5 vs. 757.8 ± 520.5 uEq/L, p < 0.001) (Table 2).
Table 1
Baseline clinical characteristics between stroke patients with AF and without AF

Table 2
Baseline laboratory characteristics between stroke patients with AF and without AF

Comparison of echocardiographic parameters showed that the stroke with AF group had significantly greater EFT (6.5 ± 1.2 vs. 5.3 ± 1.2 mm, p < 0.001), LA diameter, and LA volume compared with the stroke without AF group (Table 3). In subgroup analysis, there were no significant differences in EFT (paroxysmal vs persistent or permanent: 6.36 ± 1.06 vs 6.50 ± 1.28 mm, p = 0.769) and FFA (paroxysmal vs persistent/permanent: 1060.2 ± 557.6 vs 1546.4 ± 745.3 uEq/L, p = 0.056).
Table 3
Comparison of echocardiographic parameters between stroke patients with AF and without AF
All values are presented as the mean ± SD.
E: peak early diastolic mitral filling velocity, Ea: mitral annular velocity, EF: ejection fraction, EFT: epicardial fat thickness, IVSTd: diastolic interventricularseptal wall thickness, LA: left atrial diameter, LVEDD: left ventricular end-diastolic diameter, LVESD: left ventricular end-systolic diameter, LVMI: left ventricular mass index, PWTd: diastolic posterior wall thickness.
Comparison of neurologic clinical characteristics showed that the stroke with AF group had significantly higher hospital mortality (22.9% vs. 6.7%, p = 0.007), mRS discharge (2.8 ± 2.1 vs. 1.6 ± 1.5, p < 0.004), and NIHSS admission (7.4 ± 5.4 vs. 3.4 ± 4.2, p < 0.001) (Table 4) than the stroke without AF group.

Association of serum FFA and EFT with ischemic stroke with AF
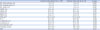
According to simple logistic regression analysis, marginally significant baseline covariates of age, gender, heart rate, eGFR, LA size, presence of coronary artery disease, heart failure, FFA, and EFT were entered into a multivariable logistic regression model (Table 5). According to the final model, which was selected in stepwise fashion, both EFT (adjusted odds ratio [OR], 2.031; 95% confidence interval [CI], 1.454–2.938; p < 0.001) and FFA [adjusted OR, 1.002; 95% CI, 1.001–1.002; p < 0.001] were independent prognostic factors associated with ischemic stroke with AF after adjusting for age (Table 5). There was no evidence against the goodness-of-fit of the fitted model (Hosmer-Lemeshow test statistic = 5.16; df = 8; p = 0.741).
Table 5
Risk factors significantly associated with the ischemic stroke patients having AF according to logistic regression models
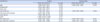
As shown in Table 6, the incremental effect of EFT and FFA on ischemic stroke with AF was investigated by comparing four different logistic regression models. Comparison of these models showed that EFT and FFA significantly improved the goodness-of-fit and discriminability of Model 1 (log likelihood difference, 21.35; p < 0.001; c-index difference, 17.9%; p < 0.001) (Figure 1).
Table 6
Incremental values of free fatty acid and epicardial fat thickness assessed by the goodness-of-fit and discriminability

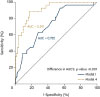
Figure 1
Comparison of four different logistic regression models of the incremental effect of EFT and FFA on ischemic stroke with AF. Comparison of these models showed that EFT and FFA significantly improved the goodness-of-fit and discriminability of Model 1 (log likelihood difference, 21.35; p < 0.001; c-index difference, 17.9%; p < 0.001).
AF: atrial fibrillation, AUC: area under curve, EFT: epicardial fat thickness, FFA: free fatty acid.
DISCUSSION
It is critically important to detect AF in patients with stroke to predict prognosis and determine the optimal treatment direction. We found that, among patients with ischemic stroke, those with AF had poorer prognosis, significantly higher serum FFA level, and a significantly higher mean EFT than those without AF. In addition, serum FFA level was significantly correlated with EFT and serum FFA level and EFT were independently associated with stroke with AF.
Some previous studies have concluded that EFT performs well in predicting the risk of AF.31)32) Also, there is evidence supporting that abnormal levels of plasma FFAs are associated with an increased risk of AF,8) and that FFAs can predict the prognosis of AF.33)34) Seo et al.35) reported that FFA was highest in cardioembolic stroke compared with other stroke subtypes, and also that FFA was higher in patients with AF than in those without AF. We recently demonstrated that FFA is a promising biomarker for predicting outcome events in stroke with AF, in addition to the CHADS2 and CHA2DS2-VASc scoring systems.36) The present study is the first to report that both EFT and FFA are independent prognostic factors of ischemic stroke with AF.
We suggest two possible mechanisms that can explain our results. First, since FFA is involved in the formation of visceral fat such as epicardial fat, increased FFA levels can cause thicker EFT, which can contribute to the occurrence of AF. An increase in FFA tracer storage per adipocyte is associated with AF.37) In obesity, increased numbers of adipocytes in epicardial fat tissue can cause high arrhythmogenesis in LA myocytes. This arrhythmogenesis might play an important role in the pathophysiology of AF.16) Abed et al.17) demonstrated that obesity progression changes LA size, conduction, histology, and expression of profibrotic mediators; moreover, these changes were associated with more persistent AF. Second, increased levels of FFAs might result in ion channel changes due to their properties, which could increase arrhythmogenesis in LA myocytes. A recent study demonstrated that the FFA stearic acid in sheep atrial myocytes disrupts their t-tubular architecture and remodels properties of membrane ionic currents, with potential implications for arrhythmogenesis.38)
Similar to a previous study reporting that ischemic stroke due to cardioembolism had poorer prognosis than ischemic stroke, due to macro- or microangiopathy,5) we also report a higher rate of in-hospital death and significantly higher mRS and NIHSS values in the ischemic stroke with AF group. Since a cardioembolism source can cause major stroke without atherosclerosis of the cerebral vessel, it is difficult to predict stroke occurrence. In cardioembolic stroke, structural diseases such as mitral valve disease or patent foramen ovale can be detected by echocardiography. However, patients with paroxysmal AF, which is not always detected by 24-hour Holter monitoring, could be missed. An ongoing prospective study is testing possible correlations between detection of AF by an implantable ECG recorder and gene mutations in patients with cryptogenic stroke/TIA; results will be available in 2018.39) Additive biomarkers or clinical variables that have the power to discriminate between ischemic stroke with or without AF would be helpful for outlining future directions, specifically how to best determine whether AF is present and/or whether to start anticoagulant therapy. The results from our study will be useful for identifying undetected AF in patients with ischemic stroke.
Our study has several limitations. First, the studied population with AF was relatively small (n = 35), limiting generalization of our results. Second, we assessed AF by documented ECG or Holter monitoring, meaning that patients with paroxysmal AF without documented ECG could have been missed. Third, with respect to baseline characteristics, the ischemic stroke with AF group showed higher prevalence of old age, heart failure, coronary artery disease, and statin use; these characteristics might have influenced the development of stroke or prognosis. Fourth, the retrospective design could have led to selection bias. Fifth, we did not analyze abdominal circumference; thus, an effect of central obesity cannot be ruled out. Finally, serum FFA levels were based on a single measurement. Future studies are needed to test whether serum FFA levels change over time and whether FFA levels on subsequent tests remain a predictor of the severity of stroke with AF.
 XML Download
XML Download