

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Papillary thyroid carcinoma (PTC) and follicular thyroid carcinoma (FTC) are often referred to together as differentiated thyroid cancer (DTC). Recently, the incidence of DTC has been increasing worldwide [123]. Despite the increase in incidence, most patients with DTC have a favorable prognosis [45]. However, 1% to 9% of patients with DTC present with distant metastasis at the time of diagnosis, and the mortality rate is significantly higher when initial distant metastasis is present [6789].
Previous studies of DTC with distant metastasis show inconsistent results. Long-term survival rates range from 13% to 100% [9101112]. This difference is thought to be due to heterogeneity among patients. Because of the rarity of the disease, most of the previous studies did not distinguish distant metastasis at initial diagnosis from distant metastasis found during follow-up. However, these two groups had different disease entities, disease characteristics, and prognoses [10]. Furthermore, primary tumor histology and site of distant metastasis are associated with different disease characteristics and prognosis [891314]. Therefore, enrollment of a homogenous group is necessary to evaluate the disease characteristics more clearly.
The epidemiology of thyroid cancer has recently been changing [1516]. Earlier diagnoses of thyroid cancer have increased since the introduction of high-resolution ultrasound sonography. New therapeutic modalities, such as tyrosine kinase inhibitors (TKIs), have been developed for the treatment of radioactive iodine (RAI)-refractory DTC [1718]. Therefore, the current prognosis of DTC with distant metastasis might be different from the past. In this study, we analyzed the clinical characteristics and long-term prognoses of Korean patients with DTC and initial distant metastasis.
METHODS
We reviewed the clinical data of 242 patients with DTC and initial distant metastasis at the time of diagnosis that had been treated between 1994 and 2013 at Samsung Medical Center, Asan Medical Center, Chonnam National University Hwasun Hospital, Samsung Changwon Hospital, and Gyeongsang National University Hospital. Duplicated patients were identified by chart review and were treated as one person at the time of analysis. The Institutional Review Board at each participating hospital approved this study (IRB number: SMC 2017-02-058, IRB 2017-0601, CNUHH-2017-069, SCMC2017-11-001, 2017-10-009). Informed consent was waived due to retrospective design.
Initial distant metastasis was defined as distant metastasis detected before or within 6 months after initial treatment. Distant metastasis was found by pathological confirmation or imaging studies such as whole-body scan (WBS), computed tomography (CT), magnetic resonance imaging, bone scan, or positron emission tomography (PET) scans [19]. Distant metastasis was classified according to the metastatic site: (1) only lung, (2) only bone, (3) combined, and (4) other site metastasis. Lung metastasis included micronodular (smaller than 1 cm), macronodular (larger than 1 cm), and miliary lung metastasis. Bone metastasis included solitary or multiple bone metastases. The combined group included cases where two or more different metastatic sites were found. Iodine avidity was determined by visual uptake in the known site of metastatic disease by WBS after RAI therapy [8].
Various factors that influence distant metastasis were reviewed for analysis. Age at initial diagnosis, gender, histologic finding of thyroid cancer after surgery, data on additional therapy for distant metastasis, and RAI avidity of the metastatic site were included for analysis. Histologic findings of thyroid cancer included primary tumor histology (PTC, FTC, Hürthle cell carcinoma [HTC]), tumor size, lymph node metastasis, extrathyroidal extension, involvement of resection margin, and lymphovascular invasion. Additional therapy included RAI therapy, TKI, external radiotherapy, and systemic chemotherapy. Disease-specific death and survival were used for prognostic analysis.
Statistical analysis
Continuous data were expressed as mean±standard deviation. Data on categorical characteristics were expressed as percent values or absolute numbers. For comparisons of clinical and pathological characteristics between the initial distant metastasis groups, a chi-sqaure test was used for categorical data and t test was used for continuous data. A multivariate Cox proportional hazard model applying the backward elimination method was used to identify factors associated with disease-specific death. P<0.05 was considered significant. Statistical analysis was performed using SPSS software version 23 (IBM Co., Armonk, NY, USA).
RESULTS
Baseline characteristics
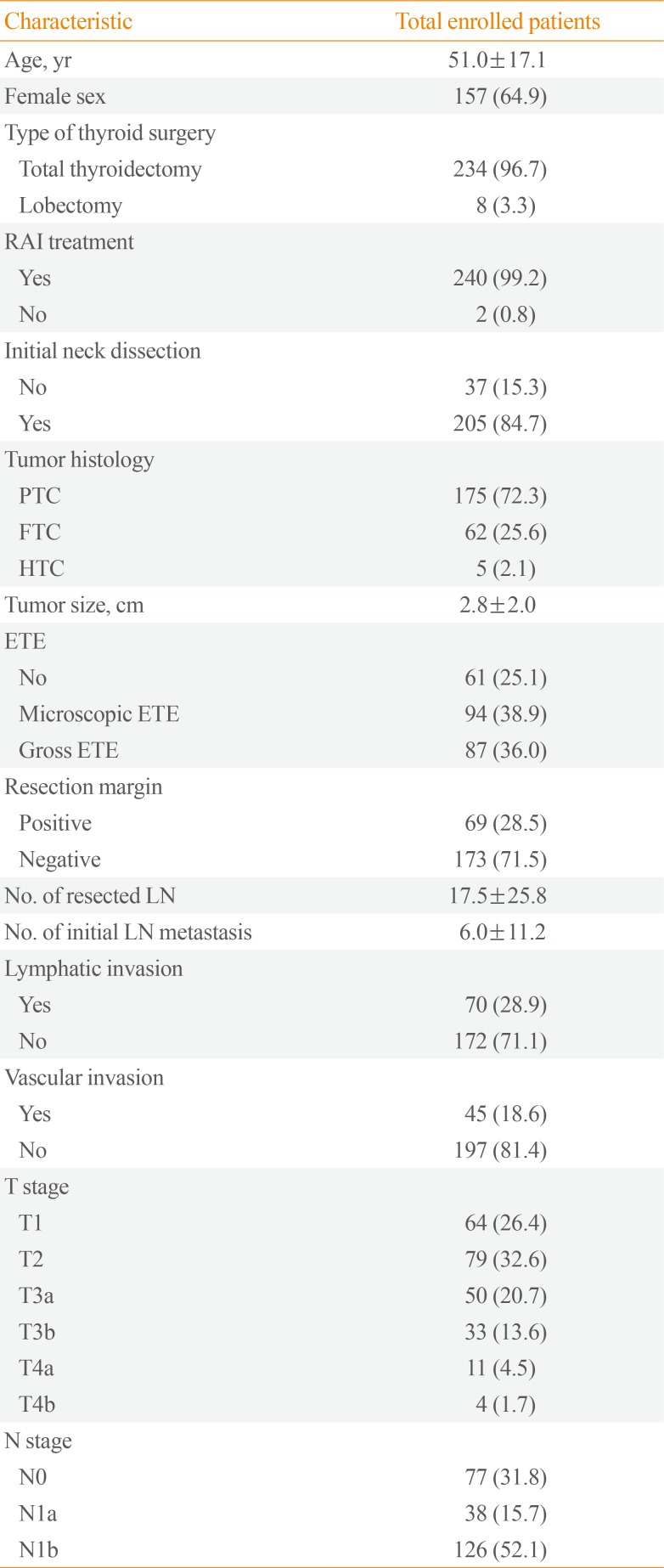
We studied 242 Korean patients with DTC and initial distant metastasis. The incidence of initial distant metastasis was 0.7% during the study period. The baseline characteristics of enrolled patients are shown in Table 1. Their median age was 51.0±17.1 years with a range from 13 to 79 years, and 65% were women. They were followed for a median of 7 years (interquartile range, 4.1 to 10.1). PTC was diagnosed in 175 patients (72%), FTC in 62 (26%), and HTC in five (2%). Among PTC subtypes, classic PTC was 147, follicular variant PTC was six, and other type of PTC was six. The median primary tumor size representing initial distant metastasis was 2.8 cm (interquartile range, 0.1 to 11.5). Gross extrathyroidal extension was found in 87 patients (36%), and positive resection margin was detected in 69 patients (29%). Nearly all patients had undergone total thyroidectomy (97%) and RAI therapy (99%), respectively.
Characteristics of initial distant metastasis
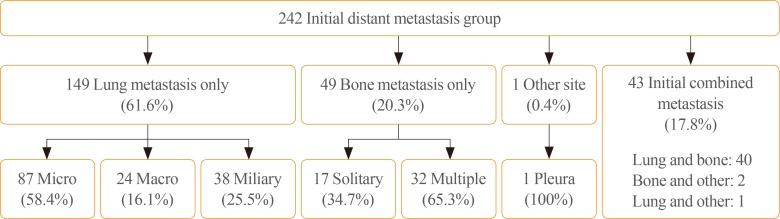
Of the 242 enrolled patients, 149 (62%) were classified as only lung metastasis, 49 patients (20%) were classified as only bone metastasis, and 43 patients (18%) were classified as combined metastasis. One patient presented with only pleural metastasis. Among other site metastasis except lung and bone, three patients showed pleural metastasis and one patient showed brain metastasis. Pleural metastasis was found in CT and brain metastasis was found in PET CT.
Among the only lung metastasis group, 87 patients (58%) were classified with micronodular lung metastasis, 24 (16%) with macronodular lung metastasis, and 38 (26%) with miliary metastasis. Among the only bone metastasis group, 17 patients (35%) were classified with single bone metastasis and 32 (65%) with multiple bone metastases (Fig. 1). The combined metastasis group included 40 patients with lung and bone, two with bone and other site, and one with lung and other site metastasis. Only lung metastasis was more frequent in PTC than in FTC (79% vs. 13%, P<0.001), and only bone metastasis was more frequent in FTC than in PTC (50% vs. 8%, P<0.001).
Among 242 patients, 50 (21%) had non-RAI avidity. According to the metastatic site, 25 of the patients (17%) with only lung metastasis, six of the patients (12%) with only bone metastasis, 18 of the patients (42%) with combined metastasis, and one of the patients with pleural metastasis had non-RAI avidity, respectively. The combined metastasis group (42%) had a higher rate of non-RAI avidity than the other lung and bone only groups.
Treatment response and survival characteristics
A total of 240 patients (99%) had undergone initial RAI therapy. Two patients were not treated with RAI for personal reasons. TKI was used in 20 patients (8%) and systemic chemotherapy in 10 patients (4%). External radiotherapy was performed on 54 patients (22%) with bone metastasis.
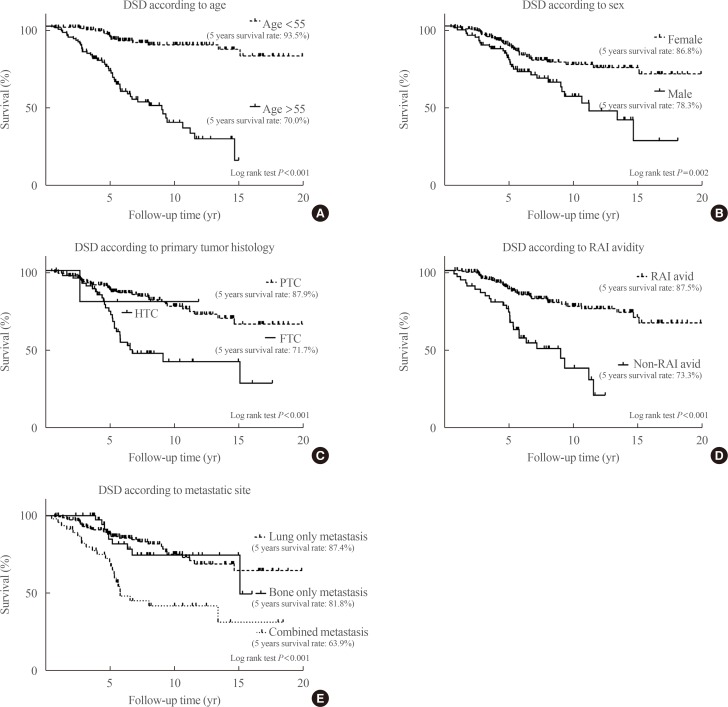
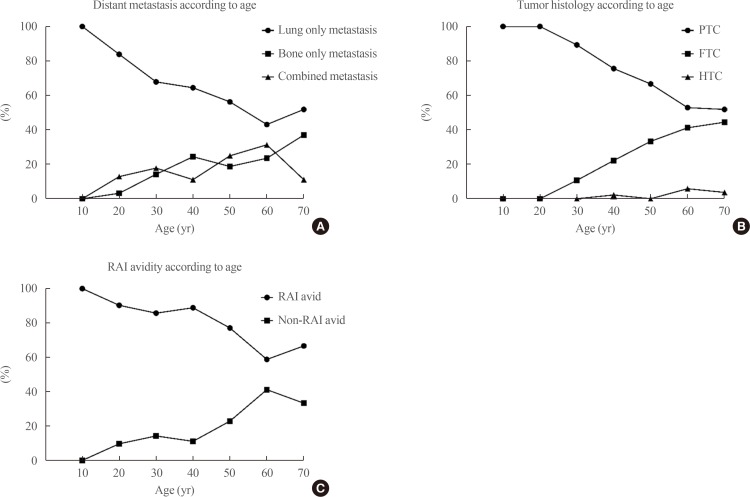
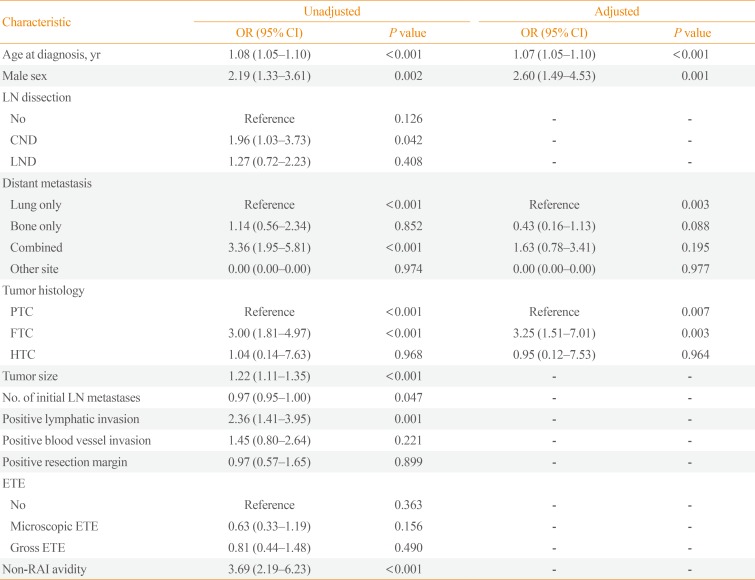
Sixty-three patients (26%) died of thyroid cancer after a median of 5 years (interquartile range, 0.5 to 15.1) after initial surgery. The 5-year survival rate was 84.8%, the 10-year survival rate was 68.1%, and the 15-year survival rate was 59.4%. Kaplan-Meier analysis and a log-rank test were used to evaluate the risk factors for disease-specific death. Age (>55 years), male sex, tumor histology (FTC), site of distant metastasis (combined metastasis), and non-RAI avidity were significant risk factors for disease-specific death (Fig. 2). After adjustment for all other variables using a Cox proportional hazard model, old age, male sex, tumor histology (FTC), and site of distant metastasis were independent risk factors for disease-specific death (Table 2). Combined metastasis had a worse prognosis than single-organ metastasis by univariate log-rank test, but there was no statistical significance according to the multivariate Cox proportional hazard model (hazard ratio, 1.63; 95% confidence interval, 0.78 to 3.41; P=0.195). The following prognostic factors were stratified according to age: site of metastasis, tumor histology, and RAI avidity. After this stratification, bone and combined metastasis, FTC, and non-RAI avidity were increased with age (Fig. 3).
DISCUSSION
We analyzed 242 patients with DTC and initial distant metastasis. To the best of our knowledge, this study was the largest study investigating DTC and initial distant metastasis, specifically regarding long-term prognosis and recent treatment status. The 10-year survival rate associated with DTC and initial distant metastasis was 68.1%, which was higher than in previous reports. Age, gender, histology, and site of distant metastasis were revealed to be the prognostic factors.
Survival rates in this study were higher than in other studies. Ruegemer et al. [20] reported that the 5- and 10-year survival rates of DTC with distant metastasis were 35% and 25%, respectively. Recently, Nixon et al. [14] reported that the 5-year disease-specific survival rate was 68% in 52 patients with DTC and initial distant metastasis at the Memorial Sloan-Kettering Cancer Center. In our study, the 5- and 10-year disease-specific survival rates were 84.8% and 68.1%, respectively. These discrepancies could be explained by a few differences. First, the study population is different. In a study by Shaha et al. [21], 43% (19/44) of the patients had PTC, 41% (18/44) had FTC, and 16% (7/44) had HTC, respectively. However, in our study, patients with PTC were predominant (PTC 72% [175/242] vs. FTC/HTC 28% [67/242]). In another study in Korea, patients with PTC were also predominant (72%) [22]. The survival rate of patients with DTC with distant metastasis in our study should be better than that in the Western studies, because of good prognosis associated with PTC compared to FTC and HTC [891314]. Second, some patients with early diagnosis of DTC, such as those with papillary thyroid microcarcinomas (PTMC) less than 1 cm in diameter, were enrolled in our study [1516]. Patients with PTMC accounted for 11% (19/174) of total PTC patients. Therefore, early detection of metastatic cancer may affect better prognosis than previous studies. Third, new therapeutic modalities such as TKI were available in our study and they might have increased the survival rate, although a limited number of patients had undergone additional therapy (TKI 8%, chemotherapy 4%) [1718].
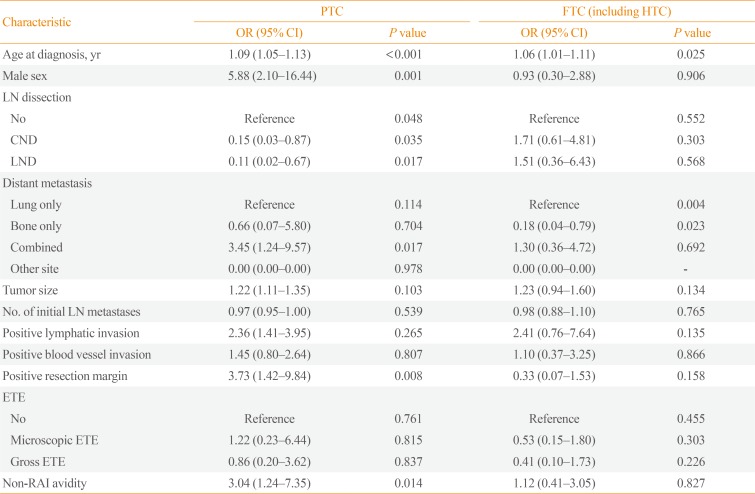
In the previous study, the prognostic factors associated with initial distant metastasis were age, number of involved organs, RAI avidity, extent of metastasis, and symptoms [1012142023]. In our study, older age, male sex, FTC, combined metastasis, and non-RAI avidity were associated with poor prognosis in a univariate log-rank test (Fig. 2). The non-RAI avidity and combined metastasis groups had poor prognosis (P<0.001). However, when the multivariate Cox proportional hazard model was used to adjust for the other variables, RAI avidity and combined metastasis were no longer significant (Table 2). As age increased, the ratio of FTC, combined metastasis, and non-RAI avidity were increased, which had a negative impact on prognosis (Fig. 3). This likely reflects that older patients tended to present with more aggressive clinical behaviors of metastatic DTC. When the patients were divided into PTC and FTC (including HTC) to analyze the factors affecting the prognosis, significant factors which affecting prognosis were different (Table 3). The factors affecting disease specific death of PTC were old age, site of metastasis (combined>lung metastasis), positive resection margin, and non-RAI avidity. However, only old age and site of metastasis (lung only>bone only) were significant prognostic factor for FTC. Because the numbers of FTC patients were relatively small, reassignment of a few cases might have changed the results.
In our study, there were two noteworthy features. One was that the youngest patient diagnosed with initial distant metastasis was 13 years old. This finding indicates that distant metastasis can occur even in children. The other was that initial distant metastasis was found in a patient whose primary tumor size was 0.1 cm in diameter, although this was an extremely rare finding. Distant metastases have usually been observed in DTC patients with tumors ≥0.8 cm [24]. Therefore, careful evaluation should be necessary even in young patients or patients with very small tumors.
Our study has several limitations. First, it was a retrospective multicenter study, and therefore some data were missing during the long-term follow-up. Also, the centers did not use the same guidelines for evaluation and treatment. Second, the proportion of patients with initial distant metastasis might have been overestimated because patients were selected from the institutional databases of tertiary care centers. Third, molecular markers such as BRAFV600E or telomerase reverse transcriptase (TERT) promoter mutations could not be used for prognostic analysis. Fourth, despite the relatively large number of DTC patients with initial distant metastasis, the numbers in some subgroups were small. Additional nationwide studies will be needed for detailed subgroup analyses. Nevertheless, this study has strength as the first large cohort study in patients with DTC and initial distant metastasis in Korea. This study presented a prevalence of initial distant metastasis in DTC patients, and also showed the distribution of initial metastasis sites, rate of initial RAI refractoriness in initial distant metastasis patients. Also it showed recent trend in treatment for advanced metastatic DTC patients and mortality. These results may be helpful in further clinical research and patient management.
In conclusion, this study showed the clinical characteristics and long-term prognosis of Korean patients with DTC and initial distant metastasis. Age, gender, tumor histology, and metastatic site were the prognostic factors for patients with DTC and initial distant metastasis, and their survival rates were better compared to those in other reports.
 XML Download
XML Download