

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Fibroblast growth factor 21 (FGF21) is a metabolic hormone that is expressed mainly in the liver to maintain homeostasis [1]. High level of circulating FGF21 is known to be induced by many metabolic disorders, such as type 2 diabetes, obesity, chronic kidney disease, non-alcoholic fatty liver disease, and cardiovascular diseases [2345]. Recently, Markan et al. [6] demonstrated that the serum FGF21 is produced from the liver, and not from adipose tissue.
In animals, both transgenic and pharmacologic FGF21 gain of function resulted in significant bone loss by augmenting the effects of peroxisome proliferator-activated receptor γ (PPAR-γ) along with diminished osteoblastic activity and increased osteoclastic activity [7]. However, in human studies, there was an independent positive association between plasma FGF21 levels and bone mineral density (BMD) in 24 healthy young women, but not men [8], suggesting a paradoxical response in mice and humans.
Recently, another study demonstrated that mice treated with recombinant human FGF21 showed no bone loss on dual-energy X-ray absorptiometry (DXA) scan and FGF21 knockout mice also did not show high bone mass [9], suggesting a neutral effect of FGF21 on bone metabolism. In another human study regarding FGF21 and BMD in 168 Han Chinese adults, plasma FGF21 concentrations were negatively correlated with BMD in the femoral neck, but there was an inverse association between only Ward's triangle BMD and plasma FGF21 in 119 women, except for the femoral neck and spine BMD [10].
However, the association between plasma FGF21 concentrations and BMD in human studies is controversial. Therefore, here, we evaluated the association between plasma FGF21 levels and BMD in healthy postmenopausal women in Korea.
METHODS
Subjects
Our study included a previously formed cohort of 337 healthy postmenopausal women volunteers older than 50 years, from June 2009 to October 2009 in Kangwon National University Hospital [11]. Serum FGF21 levels were measured from 115 consecutively selected subjects, who were not different from the unselected subjects in terms of clinical characteristics. Menopause was defined as the absence of menstruation for at least 1 year. Exclusion criteria for this study were women taking glucocorticoids and estrogen for longer than the preceding 3 months or women with diseases that could affect bone metabolism, such as Graves' disease or Cushing syndrome, hysterectomized women, and premenopausal bilaterally ovariectomized women. The study protocol was approved by the Institutional Review Board of Kangwon National University Hospital (IRB number 09-07). Written informed consent was obtained from each participant.
Laboratory tests
Areal BMD (g/cm2) values were determined in the spine, femoral neck, and total hip in all subjects using a Lunar Prodigy Vision DXA system (Lunar Corp., Madison, WI, USA). Osteoporosis was determined as a T-score ≤−2.5 standard deviations at any site according to the definition of World Health Organization. Single investigator performed all densitometry tests and analyses in all subjects. Participants' blood samples were collected during fasting for at least 6 hours after breakfast. Serum FGF21 concentration was measured using human FGF21 Quantikine ELISA Kit (R&D Systems, Minneapolis, MN, USA) with a coefficient of variation of 2.9% to 3.9% (intra-assay) and 5.2% to 10.9% (inter-assay).
Statistical analyses
The correlation between FGF21 concentration and other continuous variables was evaluated using Pearson correlation analysis. In the analysis of bone mass, actual BMD values were used, not T-scores or Z-scores. Multivariate analyses were performed with adjustment for age, BMI, and systolic blood pressure. Thereafter, we performed subgroup analyses by fracture history to examine the difference of the association between BMD scores and FGF21 levels. Statistical analyses were performed using STATA version 12.1 (StataCorp., College Station, TX, USA), and all P values were two-tailed with P values <0.05 being considered significant.
RESULTS
Clinical characteristics
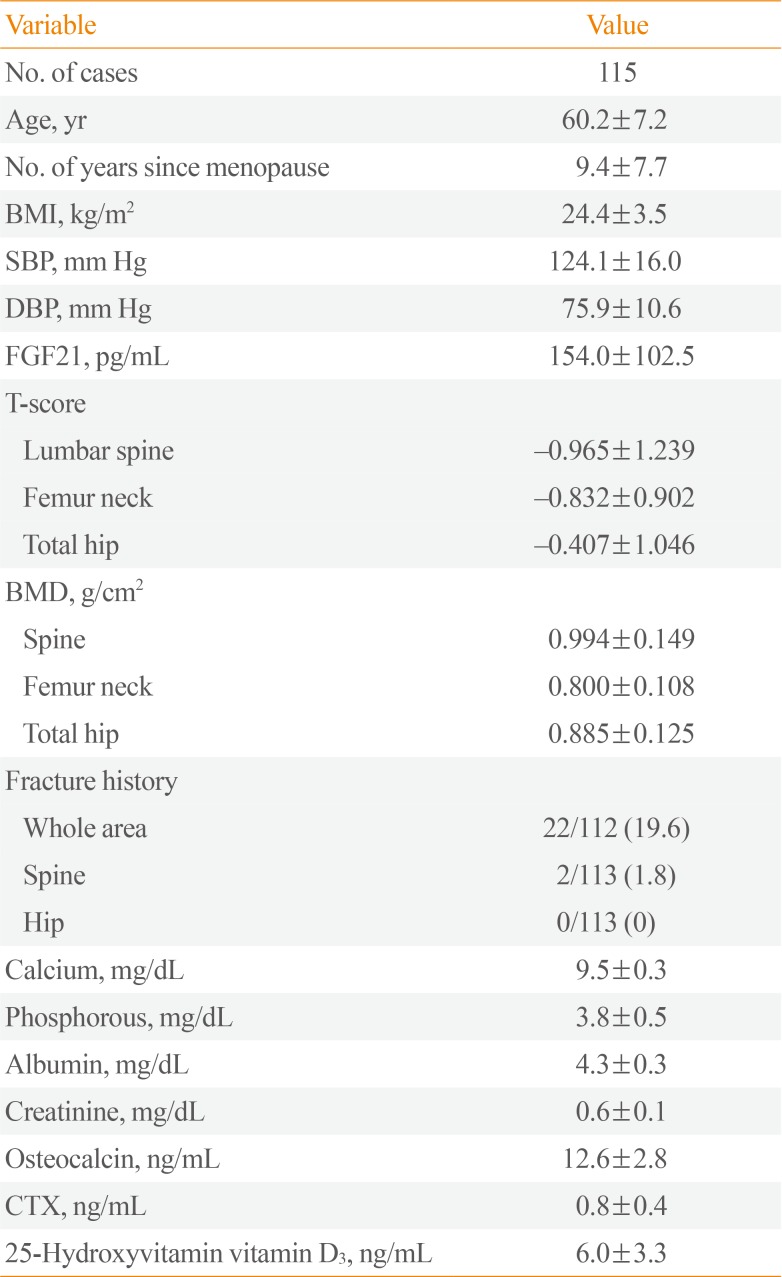
The baseline clinical characteristics of the study subjects were shown in Table 1. Among the 115 postmenopausal women, the mean age was 60.2±7.2 years, and the mean BMI was 24.4±3.5 kg/m2. The mean serum FGF21 concentration was 154±102.5 pg/mL. There were no differences in clinical characteristics between the subjects included in our study and those excluded (data not shown).
Correlation between serum FGF21 level and BMD
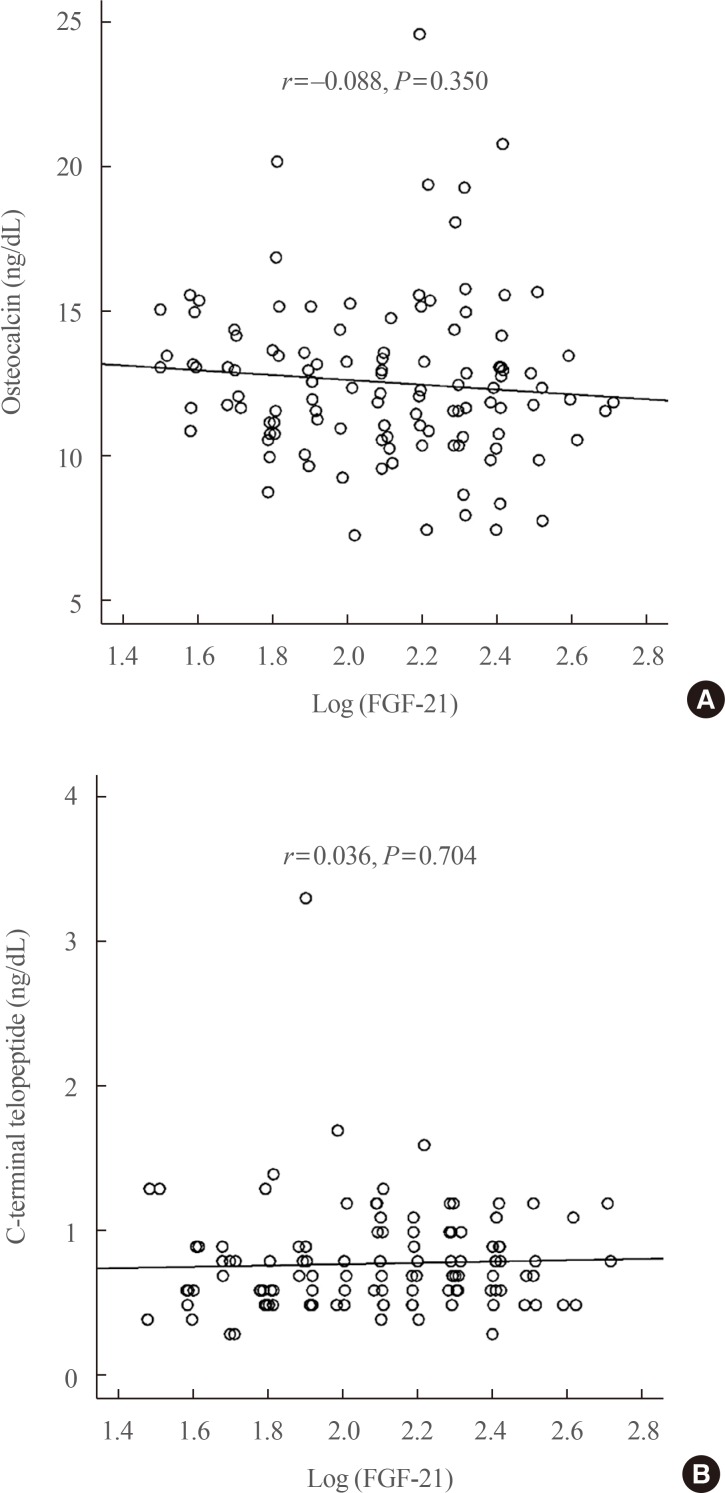
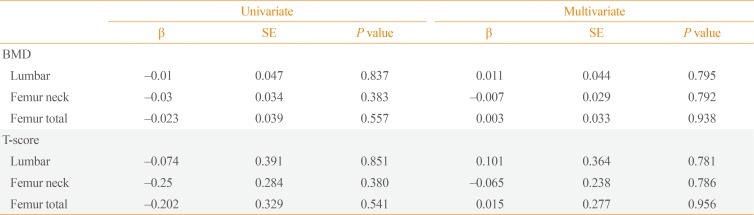
In the correlation test, we analyzed the Pearson correlation between log-transformed serum FGF21 level and T-score or regional BMD. Log-transformed serum FGF21 level did not show any significant correlation with the absolute BMD values at all three loci: lumbar, femoral neck, and total femur. Log-transformed serum FGF21 level did not show any significant correlations with osteocalcin (r=−0.088, P=0.350) and C-telopeptide (r=0.036, P=0.704) levels (Fig. 1). The other anthropometric or laboratory values also did not show any significant correlations with FGF21 levels (data not shown). The association between log-transformed serum FGF21 levels and absolute BMD scores was not observed in multivariate analyses, with adjustment for age and BMI (Table 2).
DISCUSSION
Several studies have shown the beneficial effects of FGF21 on glucose and lipid metabolism [11213]. However, some animal-based studies reported that high levels of circulating FGF21 were associated with a decrease in bone mass by inhibiting osteoblastogenesis by potentiating PPAR-γ activity in bone marrow mesenchymal stem cells [7] or promoting osteoclastogenesis by induction of insulin-like growth factor-binding protein 1 [14]. In FGF21 transgenic mice, decreased BMD was observed, along with increased bone mass with higher markers of bone formation and low markers of bone resorption in FGF21 knockout mice [7]. Originally FGF21 works through FGF receptors and β klotho complex of cell membrane and FGF receptor express in various organs, including growth plate and chondrocyte [1516]; however, there are no studies about FGF receptor on osteoblast or osteoclast so far. The indirect effect of FGF21 through increasing the activity of PPAR-γ is known to be a major mechanism of high bone resorption [7].
To date, few published studies have reported the association between plasma FGF21 level and BMD in humans. One study firstly showed the positive correlation between serum FGF21 level and total BMD and spine BMD only in 16 healthy women with mean age of 34±10 years, but not young men [8]. The authors suggested that the different results observed between men and women was because brown adipose tissue (BAT) secretes FGF21 [17] and BAT was more commonly detected in women and younger individuals than men and older adults [18]. Therefore BAT-secreted FGF21 induced higher FGF21 levels and greater BAT mass resulted in higher BMD [8]. However, the study was limited by its small sample size of only 16 young female adults.
However, a recently published report demonstrated a negative association between serum FGF21 level and Ward's triangle BMD (P=0.022, β=−0.099) only in 119 females, but not in males [10]. In the same study, for the other three regions in BMD areas, there was no significant association neither in males nor females suggesting the minimal role of FGF21 in bone metabolism. On the other hand, an epidemiologic study showed a positive correlation between age and FGF21 [19], suggesting that higher FGF21 levels in the elderly may be associated with lower BMD. However, because our study included only post-menopause women, we could not perform direct comparison of FGF21 level between age groups. Further studies considering age factor are needed.
Recent animal studies showed that intraperitoneal injection of recombinant human FGF21 for 2 weeks did not induce bone loss on DXA in high-fat diet-induced obesity mice [9], suggesting contrasting results with previous findings [78]. A recent human study of a once-weekly synthetic FGF21 analog, PF-05231023, showed that weekly FGF21 administration decreased the levels of N-terminal propeptides of type 1 collagen on day 25, but minimally increased the levels of C-telopeptide cross-linking of type 1 collagen [20]. Our data did not demonstrate any significant association between serum FGF21 level and BMD or bone markers, suggesting the minimal role of FGF21 in bone metabolism.
The major limitation of this study was its cross-sectional design; thus, we could not imply causality from the association between FGF21 and BMD in humans. Second, our study did not have enough study power to assess statistical significance due to small sample size and the weak correlations between FGF21 levels and bone parameters; therefore, our study could not prove that there was no association between them.
In summary, our current study revealed the null or minimal association between serum FGF21 levels and BMD in 115 healthy postmenopausal women. These findings indicate that the recently reported association between high FGF21 levels and bone loss in animal studies may not directly be translated to humans, suggesting the need for further investigations in humans using a large-scale prospective study.
 XML Download
XML Download