

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The thyroid gland is an endocrine gland that synthesizes and secretes thyroid hormones, which play crucial roles in the control of energy homeostasis and thermogenesis [12]. Thyroid nodule is the most common thyroid disease. The incidence of thyroid nodules has been increasing worldwide in recent years, mainly caused by the widespread use of high-resolution neck ultrasonography (USG) and computed tomography [34567]. Hypothyroidism is a pathological condition of deficient thyroid hormone, whereas hyperthyroidism is a disorder in which excess thyroid hormone is present [12]. Understanding the current distribution of thyroid dysfunction in the population is important, because it is a potential risk factor for hypercholesterolemia, cardiovascular disease, osteoporosis, arrhythmia, and neuropsychiatric disease [8].
The prevalence of thyroid nodules was found to be 14% to 29% among men and 28% to 42% among women in previous studies of subjects who underwent health checkups in Korea [491011]. However, no studies have investigated the prevalence and annual incidence of thyroid nodules in the entire Korean population. The prevalence and incidence of thyroid dysfunction vary across populations and can be influenced by several factors such as age, sex, ethnicity, and iodine status [121213]. The prevalence of hypothyroidism in the general population has been reported to be from 0.3% to 3.7% in the United States and from 0.2% to 5.3% in European countries [181415]. When subclinical hypothyroidism is also included, the overall prevalence is as high as 15% [1216]. The prevalence of overt hyperthyroidism has been reported as 0.5% to 0.8% in Europe and 0.5% in the United States [814]. Although several studies have reported the prevalence and incidence of thyroid dysfunction in Korea, some studies were not able to take recent changes into account, and other studies did not reveal the current status of patients receiving treatment [16171819].
This study aimed to investigate the prevalence and annual incidence of thyroid nodules, hypothyroidism, and hyperthyroidism in the entire Korean population using the National Health Information (NHI) database after excluding subjects with thyroid cancer.
METHODS
Data source and study population
In this nationwide population-based cohort study, 51,834,660 subjects were included using the NHI database formed and maintained by the Korean National Health Insurance Service (NHIS), which is managed by the Korean Ministry of Health and Welfare, the governmental organization that supervises all medical services in Korea [20].
Retrospective cohort data were extracted from 2002 to 2015 based on data collected during the process of claiming health care services using Korean NHIS data. The database includes information on diagnoses based on the reported International Classification of Diseases, 10th revision (ICD-10) codes, utilization records (dates of visits, types of medical institutions, types of visits, length of stay, and medical costs), and prescription records (drug code, days prescribed, and daily dosage) [20]. Because the Korean NHIS has data from 2002, we used a wash-out period from 2002 to 2005, and investigated incidence starting in 2006 to exclude the possibility that patients diagnosed before 2002 were mistaken as new patients. We excluded subjects with thyroid cancer, defined as those with the ICD-10 code C73. This study was approved by the Institutional Review Board of Kangbuk Samsung Hospital (IRB 2017-06-004). It is not necessary to have informed consent in this study.
Definitions of the diseases
Subjects with thyroid nodules were defined as those who had the ICD-10 codes E04 and D34. The prevalence was calculated by dividing the number of subjects who had thyroid nodules by the total population in 2015. Incident cases of thyroid nodules were defined as new patients who had thyroid nodules in the study period and did not have thyroid nodules before 2005.
Subjects with hypothyroidism were defined as those with the ICD-10 codes E02, E03, or E06.3 who took thyroid hormone (levothyroxine, liothyronine, or combination of levothyroxine and liothyronine) for more than 60 days to exclude patients with transient hypothyroidism. The prevalence was calculated by dividing the number of subjects who had hypothyroidism by the total population in 2015. Incident cases of hypothyroidism were defined as new hypothyroidism patients who took thyroid hormone in the study period and did not have any prescriptions for it before 2005.
Subjects who were treated due to hyperthyroidism were defined as those who had the ICD-10 code E05 and underwent treatment including antithyroid drugs (propylthiouracil [PTU], methimazole [MMI], or carbimazole [CAMZ]), thyroid surgery, or radioactive iodine (RAI) ablation. The antithyroid drug was defined as the first prescribed medicine. Subjects who had an antithyroid drug prescription for fewer than 60 days were excluded. Thyroid surgery was defined as codes P4551-P4554 and RAI ablation was defined as code HD071. Subjects who underwent thyroid surgery or RAI due to hyperthyroidism were included if they had the ICD-10 code E05 or had been prescribed antithyroid drugs. The prevalence and incidence of hyperthyroidism were calculated in the same way as for hypothyroidism.
Statistical analysis
For statistical analysis, SAS version 9.3 (SAS Institute Inc., Cary, NC, USA) was used. We used descriptive statistics to investigate the prevalence and annual incidence of thyroid disease and to evaluate trends in treatment modalities for hyperthyroidism. The prevalence and incidence of each disease was calculated by dividing the number of prevalent and incident cases by the total population, respectively, and presented per 1,000 population. Categorical variables are presented as numbers and percentages.
RESULTS
Prevalence and annual incidence of thyroid nodules in Korea
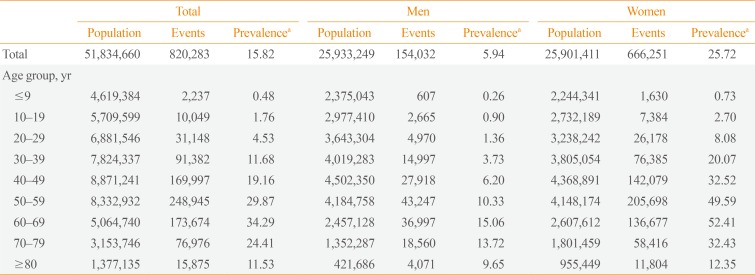
The prevalence of thyroid nodules according to sex and age group in 2015 is shown in Table 1. The number of patients with thyroid nodules was 0.82 million (0.15 million men and 0.66 million women). The prevalence of thyroid nodules was 15.82/1,000 population in Korea in 2015. Their prevalence among men and women was 5.94/1,000 population and 25.72/1,000 population in 2015, respectively. The prevalence of thyroid nodules was the greatest in the 60 to 69 years age group among both men (15.06/1,000 population) and women (52.41/1,000 population).
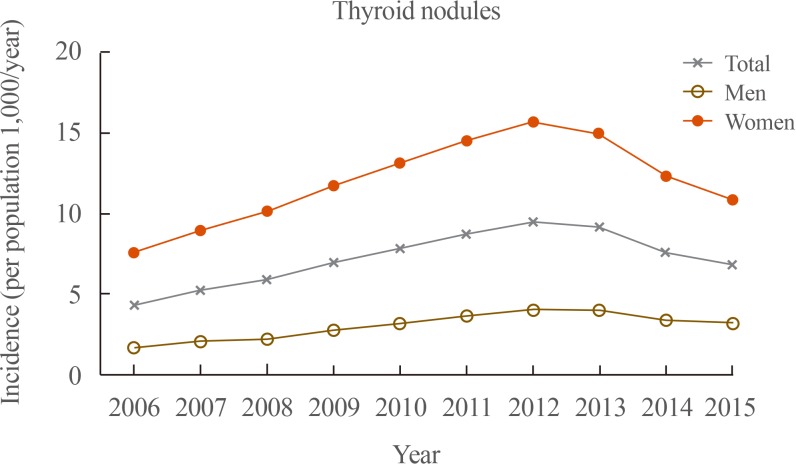
In total, the number of newly diagnosed patients with thyroid nodules steadily increased from 208,200 in 2006 to 458,500 in 2012, and then decreased to 325,400 in 2015 (Fig. 1). This corresponded to 4.36, 9.49, and 6.79 cases/1,000 population among NHIS beneficiaries in 2006, 2012, and 2015, respectively. Among men, the number of newly diagnosed patients with thyroid nodules steadily increased from 40,200 in 2006 to 100,200 in 2012, and then decreased to 80,000 in 2015. Among women, the number of newly diagnosed patients with thyroid nodules steadily increased from 168,000 in 2006 to 358,300 in 2012, and then decreased to 245,400 in 2015.
Prevalence and annual incidence of hypothyroidism in patients taking thyroid hormone in Korea
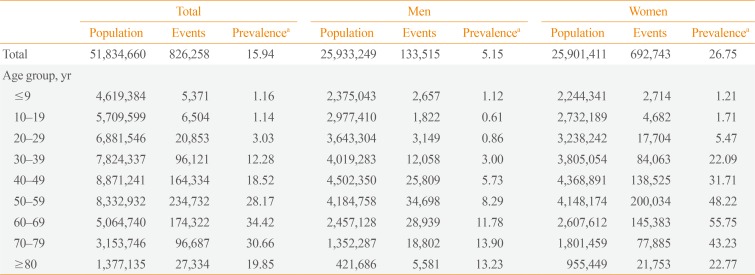
The prevalence of hypothyroidism in patients taking thyroid hormone according to sex and age group in 2015 is shown in Table 2. The number of patients who had hypothyroidism and were taking thyroid hormone was 0.82 million (0.13 million men and 0.69 million women). The prevalence of hypothyroidism in patients taking thyroid hormone was 15.94/1,000 population in Korea in 2015. Its prevalence among men and women was 5.15/1,000 population and 26.75/1,000 population, respectively. The prevalence of hypothyroidism in patients taking thyroid hormone was the greatest in the 70 to 79 years age group (13.9/1,000 population) among men, and in the 60 to 69 years age group (55.75/1,000 population) among women.
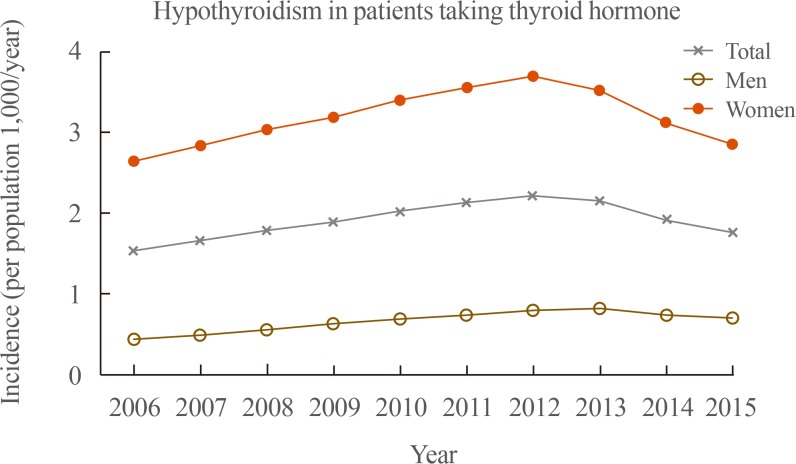
In total, the number of newly diagnosed hypothyroidism patients treated with thyroid hormone steadily increased from 73,300 in 2006 to 110,500 in 2012, and then decreased to 88,600 in 2015 (Fig. 2). This corresponded to 1.53, 2.21, and 1.76 cases/1,000 population among NHIS beneficiaries in 2006, 2012, and 2015, respectively. Among men, the number of newly diagnosed hypothyroidism patients treated with thyroid hormone steadily increased from 10,600 in 2006 to 20,000 in 2013, and then decreased to 17,800 in 2015. Among women, the number of those patients steadily increased from 62,600 in 2006 to 90,500 in 2012, and then decreased to 70,700 in 2015.
Prevalence and annual incidence of hyperthyroidism in patients undergoing treatment in Korea
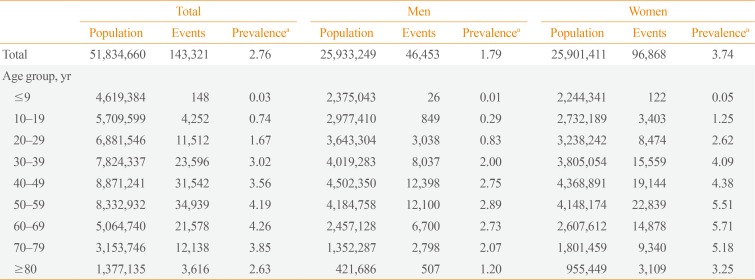
The prevalence of hyperthyroidism in patients undergoing treatment according to sex and age groups in 2015 is shown in Table 3. The number of patients who had hyperthyroidism and were undergoing treatment was 0.14 million (46,500 men and 96,900 women). The prevalence of hyperthyroidism in patients undergoing treatment was 2.76/1,000 population in Korea in 2015. Its prevalence among men and women was 1.79/1,000 population and 3.74/1,000 population, respectively. The prevalence of hyperthyroidism in patients undergoing treatment was greatest in the 50 to 59 years age group (2.89/1,000 population) among men, and the 60 to 69 years age group (5.71/1,000 population) among women.
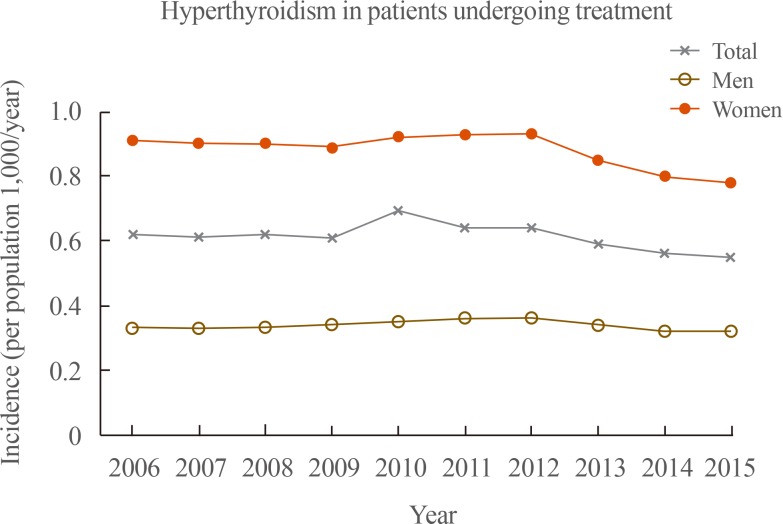
In total, the number of patients newly diagnosed with hyperthyroidism who were undergoing treatment slightly increased from 29,900 in 2006 to 32,400 in 2012, and then decreased to 28,200 in 2015 (Fig. 3). This corresponded to 0.62, 0.64, and 0.55 cases/1,000 population among NHIS beneficiaries in 2006, 2012, and 2015, respectively. Among men, the number of newly diagnosed hyperthyroidism patients who were undergoing treatment slightly increased from 7,900 in 2006 to 9,000 in 2012, and then decreased to 8,200 in 2015. Among women, the number of those patients slightly increased from 21,900 in 2006 to 23,300 in 2012, and then decreased to 19,800 in 2015.
Changes in the prescription patterns of antithyroid drugs in patients with hyperthyroidism
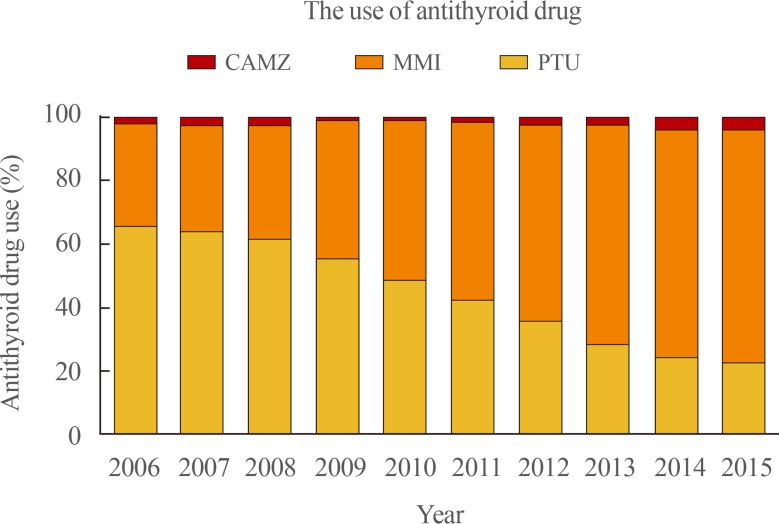
The use of different types of antithyroid drugs in patients with hyperthyroidism is illustrated in Fig. 4. PTU was the most commonly used drug for patients with hyperthyroidism before 2009, but MMI overtook PTU in 2010. Among 30,000 patients with hyperthyroidism in 2006, 65.8% of all prescriptions for antithyroid drugs were PTU, while MMI was used only in 30% of patients. The use of MMI continuously increased to 74.4% of total antithyroid drug prescriptions in 2015, and it became the most frequently prescribed antithyroid drug in Korea. In contrast, the use of PTU steadily decreased to 22.3% in 2015.
DISCUSSION
This nation-wide cross-sectional study investigated the prevalence and annual incidence of thyroid nodules, hypothyroidism, and hyperthyroidism in Korea using the NHI database after excluding of subjects with thyroid cancer. The prevalence of thyroid nodules, hypothyroidism in patients taking thyroid hormone, and hyperthyroidism in patients undergoing treatment was 15.82/1,000 population, 15.94/1,000 population, and 2.76/1,000 population in Korea in 2015, respectively. All these diseases were more prevalent among women than among men. In total, the number of incident cases of these three thyroid diseases steadily increased from 2006 to 2012, and then decreased through 2015. The incidence of thyroid nodules, hypothyroidism in patients taking thyroid hormone, and hyperthyroidism in patients undergoing treatment was 6.79/1,000 population, 1.76/1,000 population, and 0.55/1,000 population in Korea in 2015. The use of MMI continuously increased from 33% of total antithyroid drug prescriptions in 2006 to 74.4% in 2015, and it became the most frequently prescribed antithyroid drug in Korea, while the use of PTU continuously decreased.
Several studies of Korean subjects with thyroid nodules who underwent health checkups have been reported [491011]. The prevalence of thyroid nodules was 14% to 29% among men and 28% to 42% among women [491011]. However, those studies could not reflect the current state of the population and clinical practice, because the examinees of health checkup might be unusually interested in their health and have a relatively high prevalence of thyroid nodules. In the current study, the prevalence of thyroid nodules among men and women was 5.94/1,000 population and 25.72/1,000 population in 2015, respectively. The prevalence of thyroid nodules was the greatest in the 60 to 69 years age group among both men (15.06/1,000 population) and women (52.41/1,000 population).
In the current study, 5.15/1,000 population among men and 26.75/1,000 population among women took thyroid hormone due to hypothyroidism. Several studies have investigated the prevalence and incidence of hypothyroidism in Korea [161719]. A previous study using claims data provided by the Health Insurance Review and Assessment Service (HIRA) reported that the prevalence of hypothyroidism was 14.28/1,000 population in Korea in 2015 [17]. Another cohort study reported that the prevalence of subclinical hypothyroidism in the Ansung cohort and Korean Longitudinal Study on Health and Aging Study was 11.7% and 17.3%, respectively [19]. Recently, a study investigated the prevalence of hypothyroidism and hyperthyroidism using the Korea National Health and Nutrition Examination Survey VI (KNHANES VI, 2013 to 2015) by applying the reference interval of serum thyroid stimulating hormone in the Korean reference population [16]. The study reported that the prevalence of overt and subclinical hypothyroidism was 0.73% and 3.10%, respectively [16]. However, the study could not reflect the actual clinical prevalence of the disease, because the authors evaluated the prevalence of the disease after excluding patients with a prior history of thyroid disease or taking medicine that could influence thyroid function [16].
The prevalence of hyperthyroidism in patients undergoing treatment was 1.79/1,000 population among men and 3.74/1,000 population among women in this study. The prevalence of hyperthyroidism reported by previous studies from Korea was similar to that of other countries [814]. In a previous study published in 2013 using the HIRA database, the prevalence of hyperthyroidism was 3.40/1,000 population (2.09 among men and 4.70 among women), and the incidence of hyperthyroidism was 0.72/1,000 population (0.40 among men and 1.03 among women) [18]. The study using the KNHANES VI reported that the prevalence of overt and subclinical hyperthyroidism in the disease-free population was 0.54% and 2.98%, respectively [16].
The number of incident cases of thyroid nodules, hypothyroidism, and hyperthyroidism steadily increased from 2006 to 2012, and then decreased to 2015. In 2010, the Korean Thyroid Association (KTA) presented revised guidelines for the diagnosis and management of thyroid nodules and cancer and size criteria of thyroid nodules for applying fine-needle aspiration cytology (FNAC) based on the risk factors for thyroid cancer [21]. They recommended that FNAC should be performed in nodules larger than 5 mm, even if in patients at a high risk for thyroid cancer or with malignant features on neck USG [21]. For these reasons, physicians might have started to perform examinations less frequently, not only for thyroid nodules and cancer, but also for thyroid dysfunction. Ahn and Welch [22] reported that the number of operations for thyroid cancer decreased after screening for thyroid cancer with USG was discouraged in March 2014. However, the current study showed that the incidence of thyroid nodules, hypothyroidism, and hyperthyroidism decreased starting in 2013.
Recently, MMI became the most frequently prescribed antithyroid drug among the three types of antithyroid drugs (PTU, MMI, and CAMZ). PTU was the most commonly used drug for patients with hyperthyroidism before 2009, but MMI overtook PTU in 2010. The U.S. Food and Drug Administration added a new boxed warning to the label for PTU about severe liver injury in 2010, because PTU can lead to potentially fatal fulminant hepatic necrosis [232425]. The American Thyroid Association and American Association of Clinical Endocrinologists guidelines, as well as the KTA guidelines, recommended using MMI to treat hyperthyroidism, except within the first trimester of pregnancy and in patients experiencing thyrotoxic crisis [2526]. For these reasons, the trends in physician's prescriptions changed and MMI became the most frequently prescribed antithyroid drug in 2015.
This retrospective cohort study has several limitations. Because of its population-based design, this study could be subject to several biases, including coding bias, selection bias, and the effects of confounding factors. A possible discrepancy existed between the actual diagnosis and claim data because the NHIS database depends on the diagnostic code and prescription submitted on the physician's claim. In addition, the NHIS database does not contain information about prescriptions not covered through insurance. Data from thyroid function tests were not available in this study. We were not able to include subjects who had hypothyroidism and did not receive medication or those with hyperthyroidism who did not receive treatment. We could not evaluate the causative disease of hypothyroidism and hyperthyroidism. We excluded subjects diagnosed with thyroid cancer, even if they had been treated for thyroid dysfunction or had thyroid nodules. This could have led us to underestimate the prevalence and incidence of these thyroid diseases. Nevertheless, this was the first study of the prevalence and annual incidence of thyroid nodules in the entire Korean population. We investigated the prevalence and annual incidence of hypothyroidism and hyperthyroidism, taking into account recent changes and including the current status of patients receiving treatment.
In conclusion, the prevalence of thyroid nodules, hypothyroidism in patients taking thyroid hormone, and hyperthyroidism in patients undergoing treatment was 15.82/1,000 population, 15.94/1,000 population, and 2.76/1,000 population, respectively, in Korea in 2015 using the NHI database after excluding subjects with thyroid cancer. All these diseases were more prevalent among women than among men. The number of incident cases of these thyroid diseases steadily increased from 2006 to 2012, and then decreased through 2015. The incidence of thyroid nodules, hypothyroidism in patients taking thyroid hormone, and hyperthyroidism in patients undergoing treatment was 6.79/1,000 population, 1.76/1,000 population, and 0.55/1,000 population in Korea in 2015. MMI is now the most frequently prescribed antithyroid drug in Korea.
 XML Download
XML Download