

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Cervical cancer is a malignant tumor that develops in the uterine cervix and high risk human papilloma virus causes the disease. Despite the widespread screening programs, cervical cancer still remains the second most common cancer in developing countries, and it is the fourth most common cancer worldwide [12]. The primary therapy for early stage cervical cancer is surgery and that for locally advanced disease is concurrent chemoradiotherapy.
After primary therapy, regular follow-up surveillance is recommended due to the possibility of recurrence. According to the recommendations by the Society of Gynecologic Oncology (SGO) and the National Comprehensive Cancer Network (NCCN), histories and physical examinations at each visit and annual cervical/vaginal cytologies are recommended during post-treatment surveillance. Imaging studies and laboratory assessment (complete blood count, blood urea nitrogen, creatinine) are indicated based on symptoms or physical examination findings for recurrence [3].
Although a serum tumor marker test is not included in the routine post-treatment surveillance recommended by the SGO, tumor markers such as squamous cell carcinoma antigen (SCC-Ag) and carcinoembryonic antigen are evaluated and they are used to detect recurrent disease [4]. SCC-Ag is a subfraction of the tumor-associated antigen TA-4, and it is a 45-kDa glycoprotein. Increased serum SCC-Ag levels are observed in squamous cell carcinoma of the esophagus, lung, head and neck, and cervix, but increased levels may also be found in benign diseases such as skin disorders [5], pelvic inflammatory disease, cystitis, and renal failure [67]. The reason why performing the SCC-Ag test during post-treatment surveillance is not recommended for asymptomatic patients is that the survival benefit of post-recurrence salvage therapy is still uncertain, except for surgery for central pelvic recurrence after primary radiotherapy [89].
To utilize serum SCC-Ag testing at follow-up, it is required to determine the ideal threshold value for diagnosing recurrence. However, previous studies used various cutoff values of serum SCC-Ag, ranging from 1.5 to 3.0 ng/mL, which was determined to correspond to the 95th, 98th, and 99th percentiles, or 2 times the 95th percentile of serum concentrations measured in a population of healthy women [68101112131415161718]. These cutoff values were to discriminate normal from abnormal, but were not evaluated according to the suitability of detecting recurrent cervical squamous cell carcinoma in terms of cost-effectiveness (i.e., less missing recurrent disease, and less excessive imaging studies). Using these criteria, the purpose of this study was to suggest the optimal cutoff value to obtain the best cost-effectiveness, considering both sensitivity and specificity in detecting recurrent cervical squamous cell carcinoma during post-treatment surveillance.
Materials and methods
Between January 2000 and December 2014, a total of 158 women with cervical squamous cell carcinoma were treated with radiotherapy with or without concurrent chemotherapy at our department. Patients with adenocarcinoma and those who had never undergone serum SCC-Ag testing during follow-up were excluded. Patients were also excluded if they had received radiation and concurrent chemoradiotherapy as adjuvant therapy after radical hysterectomy as the primary treatment. Serum SCC-Ag tests performed during primary therapy and those performed within 3 months from the last day of radiotherapy were excluded.
A diagnosis of recurrence was defined as a recurrence confirmed by biopsy or a radiological test showing progression of a lesion. In addition, when lesions persisted for 3 months after primary treatment with radiation or concurrent chemoradiotherapy, it was considered persistent cervical cancer and diagnosed as a recurrence.
The results of serum SCC-Ag test when the disease status was uncertain were excluded from this study as follows: In the patients diagnosed as having recurrent cervical cancer, the test results obtained before diagnosis of recurrence were excluded. The results of serum SCC-Ag tests obtained when there was no evidence of disease after salvage therapy for recurrent disease were also excluded. However, the results of serum SCC-Ag tests obtained when there was an obvious recurrent lesion were included.
The patients' medical records and all test results for the diagnosis of recurrence were retrospectively examined.
1. Serum SCC-Ag measurement
Serum SCC-Ag level was measured using an immunoradiometric assay (Abbott Diagnostics, Chicago, IL, USA).
2. Statistical analysis
To determine the optimal cutoff level of serum SCC-Ag for detection of recurrent cervical squamous cell carcinoma, receiver operating characteristic (ROC) curve analysis was performed. To determine the optimal cutoff level to detect recurrent disease, Youden's index (J=sensitivity+specificity−1) was used. The serum SCC-Ag cutoff value to obtain the highest Youden's index was considered as the best cutoff level. Differences with a P-value <0.05 were considered statistically significant. Statistical analysis was performed using SPSS version 19 (IBM Co., Armonk, NY, USA).
Results
During post-treatment surveillance, 53 patients were diagnosed as having recurrent cervical cancer based on biopsy or a radiological test showing progression of a lesion. The characteristics of patients enrolled in this study are summarized in Table 1. After diagnosis of recurrent disease, 26 patients received aggressive salvage therapy (such as surgery, radiotherapy, or concurrent chemoradiotherapy), and the other 27 patients with recurrence received chemotherapy or only conservative management.
Table 1
Characteristics of the enrolled patients (n=158)

A total of 1,550 serum SCC-Ag tests during post-treatment surveillance of the 158 patients were included in this study. The results of tests performed 227 times from 53 patients with recurrent cervical squamous cell carcinoma and those of tests performed 1,323 times from 105 patients without evidence of recurrence were analyzed.
ROC curve for serum SCC-Ag to diagnose recurrent cervical squamous cell carcinoma showed that the area under the ROC curve was 0.914 (95% confidence interval, 0.887–0.942; P<0.001, Fig. 1), which indicates that serum SCC-Ag test during surveillance was helpful in detecting recurrent cervical squamous cell carcinoma. The optimal cutoff value for serum SCC-Ag using Youden's index was ≥2 ng/mL (sensitivity, 80.2%; specificity, 94.6%, Table 2).
Fig. 1
Receiver operating characteristic (ROC) curve to determine the optimal cutoff value of serum squamous cell carcinoma antigen (SCC-Ag) for diagnosis of recurrent cervical squamous cell carcinoma. The area under the ROC curve was 0.914 (95% confidence interval, 0.887–0.942; P<0.001). (A) SCC-Ag≥1 ng/mL, Sensitivity=92.5%, Specificity=50.3%. (B) SCC-Ag≥1.5 ng/mL, Sensitivity=86.3%, Specificity=85.0%. (C) SCC-Ag≥2.0 ng/mL, Sensitivity=80.2%, Specificity=94.6%. (D) SCC-Ag≥2.5 ng/mL, Sensitivity=73.1%, Specificity=97.7%. (E) SCC-Ag≥3.0 ng/mL, Sensitivity=67.8%, Specificity=98.9%.

Table 2
Sensitivities and specificities according to the different cutoff values of serum squamous cell carcinoma antigen

Recurrent diseases were classified into 4 categories considering the severity and the possibility of salvage therapy. These 4 categories were central pelvic recurrence, isolated para-aortic lymph node (LN) recurrence, pelvic side wall recurrence, and distant recurrence. To avoid an overlap, the recurrent disease with multiple lesions was classified into the most severe category (e.g., If there was central pelvic recurrence and distant recurrence, the recurrent disease was classified into distant recurrence.). The levels of serum SCC-Ag at the time of diagnosis of recurrence in the patients with recurrence amenable to salvage therapy (e.g., central pelvic recurrence or isolated para-aortic LN recurrence without previous para-aortic radiotherapy) were lower than those in the patients who were not candidates for salvage therapy (e.g., pelvic side wall recurrence or distant recurrence) (Fig. 2). The mean value and range of the serum SCC-Ag level at the time of diagnosis of recurrence according to the recurrence type are shown in Table 3.
Fig. 2
Serum squamous cell carcinoma antigen (SCC-Ag) level at the time of diagnosis of recurrence according to the recurrence type.
LN, lymph node.
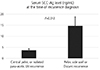
Table 3
Serum squamous cell carcinoma antigen level at the time of diagnosis of recurrence according to the recurrence type

Discussion
In general, more than half of the recurrences will occur within the first 2 years after the initial treatment for cervical cancer. Thus, the NCCN guidelines recommend follow-up evaluation every 3–6 months according to the risk of recurrence for the first 2 years, followed by every 6 months for the next 3 years. At every visit, history taking and physical examination are recommended [319]. This recommendation is based on the symptoms and physical examination will detect most cases of recurrent cervical cancer [20]. The guideline recommends annual vaginal/cervical cytologic evaluation, not at every visit. This is because retrospective studies have shown that cytologic evaluation gives a consistently low yield, with detection rates ranging from 0–17%. Especially, the role of cytologic evaluation in patients who have undergone pelvic radiotherapy may be limited [19]. Imaging studies and blood tests are only indicated based on symptoms or physical examination findings suspicious for recurrence. This recommendation is based on the fact that the rates of detection are low, and these tests have not proven useful for routine surveillance [3].
After primary surgical therapy, pelvic recurrence or para-aortic LN recurrence can be salvaged with radiotherapy or chemoradiotherapy. However, after primary radiotherapy or chemoradiotherapy, a more limited number of patients with recurrence can be candidates for salvage therapy. The survival benefit of surgical salvage therapy for central pelvic recurrence after primary radiotherapy is well established [2122]. Thus, pelvic examination and Pap smear are the most important diagnostic tools for detecting pelvic recurrence during follow-up. Some of the patients with isolated para-aortic LN recurrence without previous exposure to radiotherapy at the site were reported to survive for a long period and were considered cured [232425]. Furthermore, some of the patients with lung metastasis may have survival benefit from pulmonary metastasectomy [26]. This means that the role of aggressive salvage therapy is expanding and that the efforts to diagnose asymptomatic recurrent disease early need to be continued.
However, the drawback of using serum SCC-Ag test during in routine follow-up surveillance is that the survival benefit of the test is uncertain [27]. Ogino et al. [14] showed that routine SCC-Ag monitoring of patients with carcinoma of the uterine cervix can lead to the early diagnosis of isolated para-aortic LN recurrence, and prolonged survival can be achieved by applying radiotherapy to the para-aortic region. In contrast, Chan et al. [8] showed that post-treatment SCC-Ag monitoring is not cost-effective in the absence of curative treatment for distant spread of disease, and it does not alter clinical management. They also mentioned that most of the recurrent diseases were detected too late for curative treatment.
To use serum SCC-Ag test during post-treatment surveillance, the optimal cutoff value to detect recurrent disease needs to be determined. Previous studies used various cutoff values of serum SCC-Ag ranging from 1.5 to 3.0 ng/mL; hence, which cutoff value should be used for detecting recurrent cervical squamous cell carcinoma is still uncertain [68102829].
Several studies used the cutoff value of 1.4–1.5 ng/mL, which was determined corresponding to the 95th percentile of serum concentrations measured in a population of healthy women [1314]. Shimura et al. [16] used the cutoff value of 2.0 ng/mL, which represented the 98th percentile in a random sample of 616 healthy Japanese women. Reesink-Peters et al. [15] used the cutoff value of 1.9 ng/mL, which was the 99th percentile in a population of 250 healthy women tested at the University Hospital Groningen. In a study by Strauss et al. [17], a cutoff value of 3.0 ng/mL was selected as it corresponded to 2 times the serum concentration corresponding to the 95th percentile which was obtained in an analysis of 885 healthy women; i.e., the level corresponding to the 95th percentile in healthy women was 1.5 ng/mL in their study.
These previous studies showed that the 95th percentile of serum concentrations measured in a population of healthy women is 1.5 ng/mL, and the 99th percentile of serum concentrations is 2.0 ng/mL. The cutoff values used as the normal upper limit in these previous studies were determined according to the 95th to 99th percentile in healthy women, and they were not determined by considering the sensitivity and specificity in detecting a specific disease.
In this study, the optimal cutoff value was determined to obtain the best result considering both sensitivity and specificity in detecting recurrent cervical squamous cell carcinoma. For the purpose, we used ROC curve analysis and Youden's analysis. From this analysis, the cutoff value of ≥2 ng/mL was determined to obtain the highest Youden's index (J=sensitivity+specificity−1). With this cutoff value, a sensitivity of 80.2% and a specificity of 94.6% could be obtained, for detecting recurrent cervical squamous cell carcinoma.
If we use a very high cutoff value, most of the recurrent diseases will be detected very late for curative treatment. On the contrary, if we use a very low cutoff value, too many studies will be needed to identify the presence of a recurrent lesion (i.e., not cost-effective). This study showed that the levels of serum SCC-Ag at the time of diagnosis of recurrence in the patients with central pelvic or para-aortic LN recurrence amenable to salvage therapy were lower than those in the patients with pelvic side wall recurrence or distant metastasis.
In conclusion, serum SCC-Ag test was helpful in detecting recurrent cervical squamous cell carcinoma during post-treatment surveillance, and the optimal cutoff value was ≥2 ng/mL considering both sensitivity and specificity. Serum SCC-Ag test using the cutoff value had a sensitivity of 80.2% and a specificity of 94.6% in detecting recurrent cervical squamous cell carcinoma.
Although serum SCC-Ag level ≥1.5 ng/mL is abnormally high based on the population-based studies, the researchers recommend active imaging studies, when serum SCC-Ag level ≥2 ng/mL during post-treatment surveillance. The researchers also suggest the below protocol in addition to history taking, physical examination, and vaginal/cervical cytology. In cases of 1) SCC-Ag level ≥ 1.5 ng/mL; follow-up SCC-Ag level after 1–3 months, 2) SCC-Ag level ≥ 2 ng/mL; imaging studies and checks for other possible causes of elevated serum SCC-Ag levels (such as skin disorder, pelvic inflammatory disease, cystitis, and renal failure), 3) SCC-Ag level ≥2 ng/mL but no evidence of recurrence in imaging studies; follow-up SCC-Ag level after 1–3 months, 4) SCC-Ag level < 2.0 ng/mL with suspecting findings of recurrence in imaging studies; biopsy or follow-up imaging studies.
 XML Download
XML Download