

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Enchondral calcification and ossification of the hyaline laryngeal cartilages begins when skeletal maturity is attained and progresses thereafter as a physiological process. Calcified triticeous and thyroid cartilages are the laryngeal cartilages that are most frequently visualized on panoramic radiographs.1
Calcified laryngeal cartilages (CLC) are an incidental radiographic finding with no clinical importance. However, the detection of laryngeal cartilages (triticeous and thyroid cartilages) on panoramic radiographs is important because they may be confused with carotid artery calcifications (CAC) in the carotid bifurcation, which are a risk factor for stroke.23
On panoramic images, calcified triticeous cartilages are located in the soft tissues of the pharynx inferior to the greater horn of the hyoid bone and adjacent to the superior border of C4. Triticeous cartilages are mostly oval or circular.4 The periphery of calcified triticeous cartilage is well-defined and smooth. Ossification of thyroid cartilage was found to have radiographic manifestations ranging from linear shadows to dense laminar calcifications in patients in their third decade and beyond.5 Usually, the superior horn of a calcified thyroid cartilage appears medial to C4 and is superimposed on the prevertebral soft tissue.1 Generally, only the top 2 to 3 mm of this calcified cartilage is visible at the lower edge of the panoramic radiograph. If the cassette is positioned too far inferiorly, a greater length of this cartilage will be visualized.3 CLC may show different degrees of calcification. They generally demonstrate a homogeneous radiopacity, but may occasionally have an outer cortex.1
Interestingly, it is not well known how accurately CLC can be diagnosed on panoramic radiographs.
Although it has been suggested that on panoramic radiographs, the shape, outline, and location of triticeous cartilage can help differentiate it from CAC;4 the diagnostic indicators (sensitivity, specificity, accuracy, and false positive and false negative rates) of panoramic radiography for the diagnosis of CLC have not been evaluated. Thus, this study assessed the efficiency of panoramic radiography in the diagnosis of CLC using cone-beam computed tomography (CBCT) as the reference standard.
Materials and Methods
This retrospective study was based on 170 pairs of panoramic radiographs and CBCT scans covering the relevant region (140 males, 30 females; mean age, 41.4 years; range, 8–80 years). Initially, the CBCT scans were selected and then coupled with available panoramic images. CBCT scans obtained between December 2014 and December 2015 were chosen from the records of the Department of Dentomaxillofacial Radiology, Faculty of Dentistry, Hacettepe University (n=2177). The study protocol was reviewed and approved by the Non-Interventional Clinical Research Ethics Board of Hacettepe University. For this type of study, formal consent is not required. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Panoramic radiographs
Digital panoramic images were obtained using Orthophos XG 5 (Sirona Dental Company, Bensheim, Germany; 60–90 kVp, 3–16 mA, 14 s) or Veraview IC5 (Morita Corporation, Kyoto, Japan; 60–70 kVp, 1–7.5 mA, 5.5–10 s) equipment. Exposure parameters were selected according to the patient's size. Radiographs on which the hyoid bone was too low in the neck to be visualized were excluded. The images were anonymized before the analysis, and were numbered and saved.
Panoramic radiographs were examined to detect thyroid and triticeous cartilage calcifications according to the imaging features presented in an oral radiology textbook1 by an oral and maxillofacial radiologist (GA) with 11 years of experience. A calibration study was carried out for the observer before the examination of the panoramic images. Both types of calcifications were designated as laryngeal cartilage calcifications.
CBCT scans
The CBCT scans were acquired with an i-CAT Next Generation (Imaging Sciences International, Hatfield, PA, USA) unit. A tube voltage of 120 kVp was used for all acquisitions, with variation in the field of view, acquisition voxel size, tube current (3–7 mA), and exposure time. The images were viewed with i-CAT Vision software (version 1.9.3.14, Imaging Science International, Hatfield, PA, USA). The CBCT scans were reviewed by 2 oral and maxillofacial radiologists.
For optimal viewing, a task-specific image display for soft-tissue calcifications of the neck was used. The recommended protocol used a slice thickness of 30 mm and maximum intensity projection images.6 Therefore, in the present study, each scan was initially viewed with this protocol. Once a calcification was identified, thinner slices were obtained if more detail was needed.
Statistical analysis
The kappa coefficient (κ) was calculated to determine the level of intra-observer agreement for the panoramic radiography evaluations and to determine the level of agreement between the 2 methods.
The discrimination of radiographs with and without laryngeal cartilage calcification and diagnostic indicators (sensitivity, specificity, and accuracy) for the panoramic radiography evaluations were also calculated. Data analysis was performed using SPSS Statistics version 17.0 (SPSS Inc., Chicago IL, USA.). P values <.05 were considered to indicate statistical significance.
Results
A total of 312 regions (142 bilateral, 10 left, 18 right) were evaluated in 170 patients (140 males, 30 females). The observer re-evaluated 82 panoramic images to assess the level of intra-observer agreement. The kappa coefficient was calculated as 0.709, which was statistically significant (P<.05).
There was a statistically significant and acceptable relationship between the CBCT and panoramic image evaluations (κ=0.684, P<.05).
The sensitivity, specificity, and diagnostic accuracy rate of panoramic radiography for the discrimination of positive-CLC and negative-CLC images according to the CBCT gold standard were 85.4% (158 of 185), 83.5% (106 of 127), and 84.6% (264 of 312), respectively. In 127 CBCT images, CLC was not detected, while in 21 panoramic images it was mistakenly detected (false positive rate, 16.5%). Furthermore, in the CBCT images, 185 cases of CLC were detected, while in 27 panoramic images it was mistakenly not detected (false negative rate, 14.6%) (Table 1).
Discussion
In the dental literature, laryngeal calcifications have been described in relation to their appearance on panoramic radiographs, with a great emphasis on differentiating triticeous ossification from CAC. To the best of our knowledge, the present study is the first to assess the efficiency of panoramic radiography for the detection of CLC.
Recently, a study in a large population (age range, 18–97 years; mean age, 65 years) utilizing computed tomography images revealed that the presence of triticeous cartilage as a part of the laryngeal skeleton was quite common (53.1%).7 In contrast, the frequency of calcified triticeous cartilage on panoramic radiographs was reported to be 5% in men and 12% in women among 40 years and over.4 This disparity in the prevalence is partially due to the technique of panoramic radiography. The hyoid bone is the reference point for the diagnosis of laryngeal cartilages on panoramic radiography. However, in some cases, the hyoid bone may be too low to be visualized on panoramic radiographs.
A complicating factor in relation to the differential diagnosis is that the age range of the greatest prevalence of CAC coincides with the age range associated with the occurrence of patterns of mineralization and/or calcification that have been reported to be responsible for erroneous diagnoses, such as ossification of the triticeous, cricoid, and thyroid cartilages.2 Furthermore; Alqahtani et al.,7 in a study of computed tomography, reported a wide range of variation in the morphology, shape, ossification, and position of the triticeous cartilage within the thyrohyoid ligament. Due to this variation, symmetric contralateral comparison is not appropriate for the diagnosis of CLC.
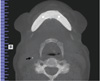
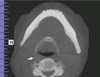
Initial decisions regarding soft-tissue calcification in the soft tissues of the lateral neck of panoramic images involve determining the location of the calcification relative to the hyoid bone and further characterization relative to other structures or appearances. In addition to CLC, calcified lymph nodes in the carotid sheath and CAC can be found below the hyoid bone. Calcified triticeous cartilages have been described as single, small, round radiopacities below the greater horn of the hyoid.8 Kamikawa et al.2 positioned radiopaque spheres in the anatomic structures of the cervical region that can be sites of calcification in cadaver specimens, and found that 75% of the examiners correctly indicated the reference point at the bifurcation of the carotid artery and 79.2% reported a triticeous cartilage as CAC. This study showed that the localization of radiopacities in the cervical region of panoramic radiographs alone is not enough for the diagnosis of calcified laryngeal structures. In contrast, Ahmad et al.4 showed that the shape, outline, and location of the triticeous cartilage can help differentiate it from CAC. The current study showed that the diagnosis of CLC is possible with panoramic radiography in most cases. However, when small, ill-defined opacities are present below the greater horn of the hyoid (Figs. 1,2,3,4), supplemental radiographs are needed because even small areas of CAC could be associated with an elevated risk of stroke or other cardiovascular events.9
In the present study, both types of calcifications were designated as laryngeal cartilage calcifications, and the exclusive efficiency of panoramic radiography for the diagnosis of calcified triticeous cartilage was not estimated. This retrospective study was based on CBCT scans that were obtained at our dental faculty from patients with diseases in the oral and maxillofacial region. Therefore, in most cases, the field of view did not allow triticeous cartilages to be distinguished from thyroid cartilages.
In conclusion, the present study showed that CLC could be diagnosed on panoramic radiographs in most cases. However, diagnosis may be difficult due to variation in the calcifications.



 XML Download
XML Download