

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The 4th edition of the World Health Organization (WHO) classification of breast tumors defines encapsulated papillary carcinoma (EPC) as a variant of papillary carcinoma that is surrounded by a thick fibrous capsule and lacks myoepithelial cells (MECs) within the papillae and around the periphery of the tumor, as demonstrated by a panel of immunohistochemistry (IHC) markers [1]. According to the classical breast pathology textbooks, the lack of MECs suggests malignant clinical behavior breast neoplasms; however, EPC is reported to be a relatively indolent tumor, and very few cases have shown axillary lymph node metastases [2]. Several hypotheses about the biological nature of EPC exist; for example, a tumor in transition from an in situ to an invasive phase and an indolent low-grade carcinoma with pushing rounded invasion [3]. The WHO Working Group advocates that EPC should be staged as an in situ lesion (Tis) [14]. EPC is a well-circumscribed tumor of the elderly and can be accompanied by a conventional in situ and/or invasive carcinoma component, most frequently in the form of invasive no special type (NST) carcinoma [5]. The present case perfectly matches these characteristics.
Apocrine breast neoplasms are characterized by a specific histologic appearance, which resembles apocrine metaplasia on hematoxylin and eosin (H&E) stained slides. Such tumors consist of abundant granular eosinophilic cytoplasm and large nuclei, with prominent nucleoli [1]. This subset of breast tumors is generally estrogen receptor (ER) negative, progesterone receptor (PR) negative, and androgen receptor (AR) positive [6]. Our previous results suggest that these tumors are also almost uniformly positive for growth hormone-releasing hormone-receptor (GHRH-R) [78]. The majority of apocrine carcinomas can be considered special variants of NST carcinomas, although apocrine differentiation has also been reported in several special-type cancers, including EPC [9101112].
Go to : 
CASE REPORT
On a breast screening mammography, a 70-year-old woman was diagnosed with a complex breast lesion in the upper-outer quadrant of her right breast. The lesion contained a cystic part and a neighboring spiculated area, which was suggestive of an infiltrative component (Figure 1A-1C). Fine needle aspiration cytology of the lump showed atypical apocrine epithelial cells, but confirmation of the suspected malignancy was not possible. The subsequent core needle biopsy disclosed an invasive carcinoma with apocrine differentiation. The patient underwent breast-conserving surgery with a sentinel lymph node biopsy.
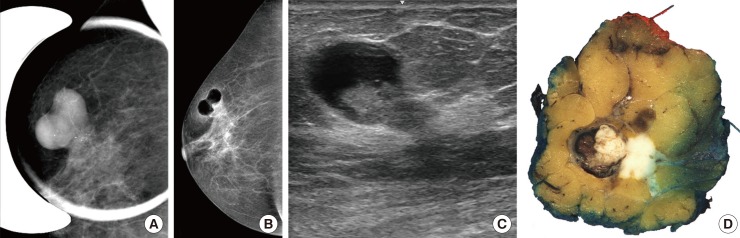 | Figure 1Imaging and gross findings. Architecture of the dual tumor with mammography (A), pneumocystography (B), ultrasound (C), and gross morphology (D). Note the sharply outlined component, showing a clear cystic nature (B, C) with an intraluminal mass. In connection with the intracystic tumor an ill-defined lesion with coarse microcalcifications (A) suggestive of an infiltrative tumor component is also present.
|
The gross examination discovered a correlating dual lesion, which consisted of an intracystic proliferation and a tumor mass that was ill-defined and infiltrative in appearance (Figure 1D). Microscopically, the intracystic portion showed a thick fibrous capsule, an intraluminal dominantly papillary, partially solid proliferation, and a total absence of MEC, under H&E staining and p63, cytokeratin 5, smooth muscle actin, and CD10 IHC (Figure 2) [13]. The ill-defined component represented a NST invasive carcinoma with desmoplasia. Both the intracystic and infiltrative parts showed cytomorphologies that agreed with apocrine differentiation, with eosinophilic granular cytoplasm, large nuclei, and prominent nucleoli. Small apocrine ductal carcinoma in situ foci were also present. The invasive tumor was categorized as grade 2 (2+3+ 2=7 points for tubule formation, pleomorphism, and mitotic activity, respectively), according to the Elston-Ellis modification of the Scarff-Bloom-Richardson system. With respect to prognostic and predictive IHC markers, all tumor components were negative for ER, PR, and human epithelial growth factor receptor 2 (HER2), and showed a Ki-67 labeling index of 15%. The tumor was positive for AR, with an Allred score of 8, gross cystic disease fluid protein 15 (GCDFP-15) and GHRH-R were both observed in the intracystic papillary carcinoma, and the tumor contained an infiltrative NST carcinoma component (Figure 2). Based on our findings, the diagnosis of apocrine EPC of the breast, associated with an invasive NST (ductal) carcinoma with apocrine differentiation, was established.
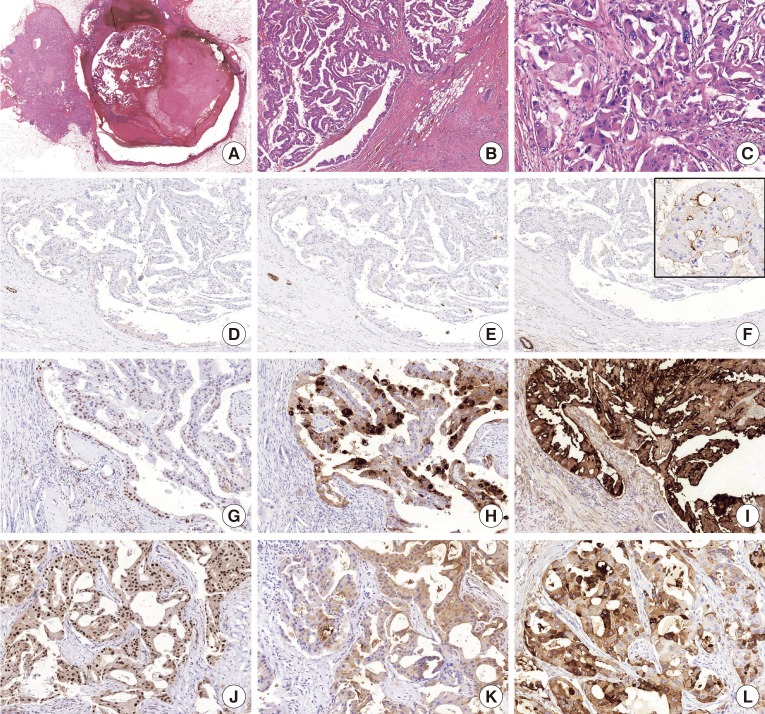 | Figure 2Histological characteristics and immunoprofile. (A) An intracystic papillary component (right) is surrounded by a thick fibrous capsule and an invasive carcinoma (left) component on the low-power view of the lesion (H&E stain, ×1.2). (B) The intracystic part shows a prominent papillary architecture and apocrine cytomorphology (H&E stain, ×5). (C) The invasive carcinoma part also demonstrates apocrine cytomorphology (H&E stain, ×20). The p63 (D, H&E stain, ×5), cytokeratin 5 (E, H&E stain, ×5), and CD10 (F, H&E stain, ×5) immunohistochemistry markers demonstrate the absence of myoepithelial cells in the intracystic papillary component; note the positive internal control and the focal luminal CD10 expression (insert) frequently observed in apocrine lesions [13]. As an evidence for apocrine differentiation, both the encapsulated papillary carcinoma component (G-I, ×15) and the invasive component (J-L, ×20) express androgen receptor (G and J, respectively), gross cystic disease fluid protein 15 (H and K, respectively), and growth hormone-releasing hormone-receptor (I and L, respectively).
|
Go to :
DISCUSSION
EPC of the breast, formerly known as intracystic and encysted papillary carcinomas, is a rare tumor type that represents approximately 1% of all breast carcinomas. The previously published 10 cases of apocrine EPC (A-EPC) all lacked a conventional invasive component and have been described to have indolent clinical behaviors (Table 1) [9101112]. MECs are sometimes very hard or even impossible to identify around benign cystic apocrine glands [1415], and they may virtually, partially, or completely lack benign cystic apocrine lesions with papillary proliferations [15]. Therefore, the definition that was used for classic EPCs should be applied to apocrine variants with caution. This doubt was also formulated in the first series of such lesions, where the term encapsulated apocrine papillary carcinoma was used, based on compliance with the WHO terminology: a papillary lesion without MECs in the papillary area and at the periphery. The authors also stressed that the malignant potential of A-EPC has not yet been proven [9]. A characteristic feature of EPCs, the presence of a thick fibrous capsule, was lacking in at least some of the five cases, as shown in Figure 8 of the paper [9]. The present A-EPC case, on the other hand, displayed a thick fibrous capsule and a threefold variation in nuclear caliber. This case is unique in the sense that it represents a two-component tumor, with an EPC and a conventional invasive NST component, both of which demonstrate apocrine differentiation. The reported case, therefore, may provide proof that A-EPC has the potential to display the same disease spectrum as conventional EPC, including an association with ductal carcinoma in situ and invasive carcinoma [5]. We therefore propose that A-EPCs are not necessarily as indolent as previously suggested by the nine pure A-EPC lesions. Our case implies that the clinical behavior of A-EPCs falls into the same unpredictable malignant potential category as the behavior of classical EPCs, rather than into a completely indolent category, as put forward by the first reported cases.
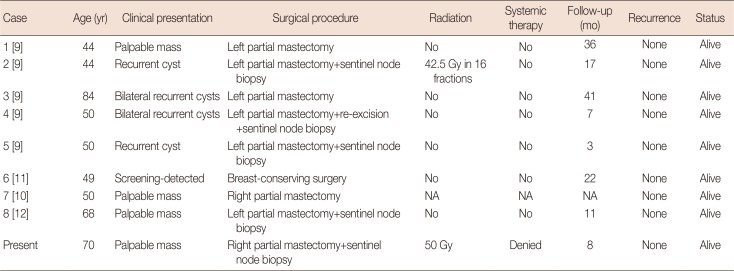
Table 1
Patient information, treatment, and outcome of previously published apocrine EPCs and present case
| Case | Age (yr) | Clinical presentation | Surgical procedure | Radiation | Systemic therapy | Follow-up (mo) | Recurrence | Status |
|---|---|---|---|---|---|---|---|---|
| 1 [9] | 44 | Palpable mass | Left partial mastectomy | No | No | 36 | None | Alive |
| 2 [9] | 44 | Recurrent cyst | Left partial mastectomy+sentinel node biopsy | 42.5 Gy in 16 fractions | No | 17 | None | Alive |
| 3 [9] | 84 | Bilateral recurrent cysts | Left partial mastectomy | No | No | 41 | None | Alive |
| 4 [9] | 50 | Bilateral recurrent cysts | Left partial mastectomy+re-excision+sentinel node biopsy | No | No | 7 | None | Alive |
| 5 [9] | 50 | Recurrent cyst | Left partial mastectomy+sentinel node biopsy | No | No | 3 | None | Alive |
| 6 [11] | 49 | Screening-detected | Breast-conserving surgery | No | No | 22 | None | Alive |
| 7 [10] | 50 | Palpable mass | Right partial mastectomy | NA | NA | NA | None | Alive |
| 8 [12] | 68 | Palpable mass | Left partial mastectomy+sentinel node biopsy | No | No | 11 | None | Alive |
| Present | 70 | Palpable mass | Right partial mastectomy+sentinel node biopsy | 50 Gy | Denied | 8 | None | Alive |
![]()
Go to :
 XML Download
XML Download