

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the most common type of cancer and the second leading cause of cancer mortality among women in the United States [1]. Alcohol is a well-known breast cancer risk factor that has shown consistent positive associations in the majority of studies [2]. Alcohol intake increases the risk of breast cancer by 7% for each additional 10 g of alcohol consumed per day [3]. However, studies on the association between alcohol and breast cancer outcomes such as recurrence, second primary, and mortality are inconsistent [4567].
Adjuvant hormone therapy is used after breast cancer diagnosis and surgery to improve overall survival. Previous studies have shown that adjuvant hormone therapy improves breast cancer-free survival by reducing mortality and the risk of recurrence by 34% and 40%, respectively, within 5 years of treatment [8]. Whether there is an interaction between alcohol consumption and adjuvant hormone therapy on patient outcome is unknown, but some previous studies have shown that concurrent alcohol consumption of >20 g/day and postmenopausal hormone therapy increases breast cancer risk two-fold compared to women with no alcohol consumption [9]. Several biological mechanisms may explain a potential interaction between alcohol consumption and adjuvant hormone therapy, including effects on the metabolism of estrogens and xenobiotics via activation of the P450 cytochrome family enzymes [101112]. Activation of aromatase can lead to an increase in estrogen levels which may interfere with the effectiveness of the treatment, while activation of other P450 cytochrome family enzymes participating in xenobiotic metabolism may result in more rapid conversion of tamoxifen into biologically active metabolites [1011121314].
The potential interaction between alcohol use and adjuvant hormone therapy has never been investigated. We examined, for the first time, the interaction between alcohol consumption and adjuvant hormone therapy in relation to breast cancer- free survival in women diagnosed with primary breast cancer.
METHODS
Study population
The current study utilized resources from the Health and Research Informatics (HRI) data warehouse at the Moffitt Cancer Center in Tampa, FL, USA. The HRI data warehouse at the Moffitt Cancer Center links patient data across several systems including medical records, cancer registry, tissue banking, billing, and patient questionnaires. Moffitt new patients complete an electronic clinical intake form as part of clinical care, and these discrete data are uploaded into the HRI data warehouse and were utilized in this analysis. For the current study, we queried the HRI data warehouse to identify all women who were diagnosed with incident invasive breast cancer and were treated between 2007 and 2012, completed the patient survey prior to diagnosis, and had available data on alcohol consumption (n=1,407). From these, we excluded eight women due to missing data on adjuvant hormone therapy or age at diagnosis. The final study population thus included 1,399 women. This study was approved by the University of Florida and Moffitt Cancer Center Institutional Review Boards as non-human subjects research (protocol numbers 201500573 and Pro00014441, respectively). Patients provided written informed consent for their data to be used for research.
Breast cancer outcomes
The history of a secondary malignant breast neoplasm and chemotherapy indicator codes from the cancer registry and patient billing system were used to identify women with the outcomes of interest. This approach was similar to the methods previously described by Hassett et al. [15]. Breast cancer-free survival was defined as the time between the breast cancer diagnosis and one of the adverse outcomes (recurrence, second primary breast cancer, or death from breast cancer) or, for women without an adverse outcome, the end of the study or death from other causes, whichever occurred first. Second primary breast cancer was defined as having International Classification of Diseases version 9 (ICD-9)-Clinical Modification code 198.81 during the follow-up. Recurrence was defined as having any of the relevant breast cancer-related treatments that occurred at least 15 months after the date of original diagnosis, in the absence of any new cancer diagnosis at another site. Death from breast cancer was identified through the cancer registry. Women without an outcome of interest were censored at the time of death by other causes or at the end of the study (7/31/2015).
Alcohol consumption
Alcohol consumption during the 12 months preceding diagnosis was assessed through a self-administered patient survey prior to breast cancer diagnosis. Participants were asked to report the frequency of alcohol consumption, the number of drinks typically consumed, and the type of beverage. One drink was defined as one 355-mL can or a bottle of beer, one 148-mL glass of wine, one can or bottle of a wine cooler, one cocktail, or one shot of liquor. Alcohol consumption was categorized as binary (none [0 drinks/month] and any [>1 drink/month]) and, among women with available data on the number of drinks per day (n=1,182), as never (0 drinks/week), moderate (≤7 drinks/week), and heavy (>7 drinks/week) [16].
Covariates
The self-administered patient survey collected information on potential confounders, including demographics, menopausal status, reproductive history, and family history of breast cancer in first-degree relatives. Family history was categorized as having no family member with a history of breast cancer or having any first-degree family member with breast cancer (including mother, daughter, sister, father, brother, or son). Body mass index (BMI) was calculated using height and weight available from the medical record or reported on the survey. For the majority of the women with known BMI (982 out of 1,099), information was available from within the year preceding diagnosis. BMI was categorized as underweight/normal (<25 kg/m2), overweight (25–29.9 kg/m2), obese (≥30 kg/m2), or unknown. Clinical information including treatment details and tumor characteristics were available from the cancer registry.
Statistical analyses
Baseline characteristics of women with and without the study outcomes were compared using chi-square (or Fisher exact test) and t-tests, overall and by the status of adjuvant hormone therapy. Cox proportional hazards models were used to calculate hazard ratios (HRs) and corresponding 95% confidence intervals (CIs). Follow-up for women with a study outcome was defined as the number of months from the date of diagnosis to the first occurring outcome of interest: breast cancer recurrence, second primary breast cancer, or death from breast cancer. In our sample, 85 women had second primary breast cancer, 439 had recurrence, and 35 women died from breast cancer. Follow-up for women without the outcomes was defined as the number of months between primary breast cancer diagnosis and either date of death from other causes or the end of the study, whichever came first. The risk estimates were adjusted for potential confounders, and the final model was selected using a step-wise model selection approach. BMI and age at diagnosis were forced into the final survival model as they have shown associations with breast cancer-free survival in previous studies [1718]. The final models included the following covariates: age at diagnosis (years), BMI (normal, overweight, obese, unknown), menopausal status (post, other), chemotherapy (yes, no), surgery (yes, no), and immunotherapy (yes, no).
Proportional hazards assumption was evaluated, and chemotherapy was the only variable to violate the proportional hazards assumptions. To account for the nonproportionality, we added an interaction term with chemotherapy and time into the models [19]. The interaction between alcohol consumption and adjuvant hormone therapy was evaluated by including an interaction term in the overall models. Next, the survival analysis was stratified by adjuvant hormone therapy.
A secondary analysis was also performed to assess the potential masking effects of immune- and chemotherapy on survival by excluding women with immune- or chemotherapy. The associations were examined overall and by the status of adjuvant hormone therapy. All the tests were two-sided and statistical significance of the effects was assessed at p≤0.05 significance level. All analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, USA).
RESULTS
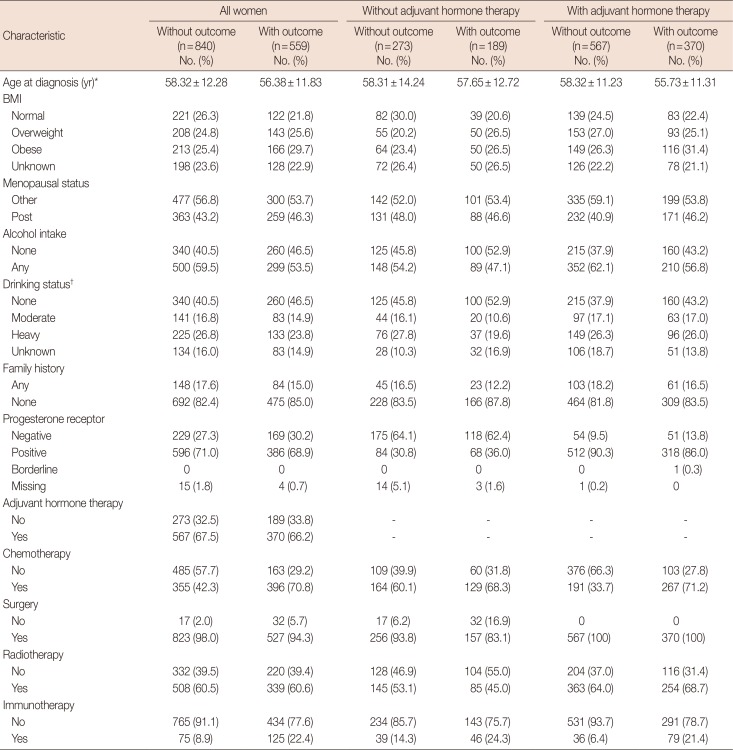
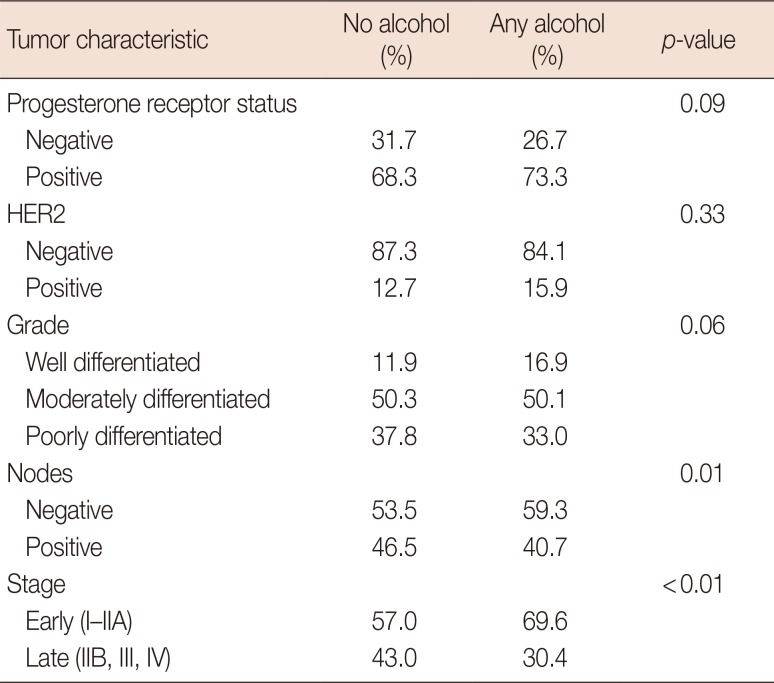
This study included 1,399 women with invasive breast cancer (462 women without adjuvant hormone therapy and 937 with adjuvant hormone therapy). The average follow-up time was 31.56±18.75 months. Characteristics of women in the study are presented in Table 1. Compared to women without any of the adverse study outcomes (recurrence, second primary breast cancer, or death from breast cancer), women with an outcome were less likely to be drinkers (53.5% vs. 59.5%, p=0.03) and to have had surgery (94.3% vs. 98.0%, p<0.01) and more likely to have had chemotherapy (70.8% vs. 42.3%, p<0.01) and immunotherapy (22.4% vs. 8.9%, p<0.01). Among women with adjuvant hormone therapy, those with the outcome were less likely to have a progesterone receptor positive tumor (86.0% vs. 90.3%, p=0.03) and more likely to have had chemotherapy (71.2% vs. 33.7%, p<0.01) or immunotherapy (21.4% vs. 6.4%, p<0.01). Among women without adjuvant hormone therapy, those with a study outcome were less likely to be heavy drinkers (19.6% vs. 27.8%, p=0.04) or to have had surgery (83.1% vs. 93.8%, p<0.01) and more likely to have had immunotherapy (24.3% vs. 14.3%, p=0.01) (Table 1). Distribution of tumor characteristics, including receptor statuses and grade, were similar in drinkers and nondrinkers (Table 2). Compared to nondrinkers, women who consumed alcohol were more likely to have negative nodes (59.3% vs. 53.5%, p=0.01) and early-stage tumors (69.6% vs. 57.0%, p<0.01).
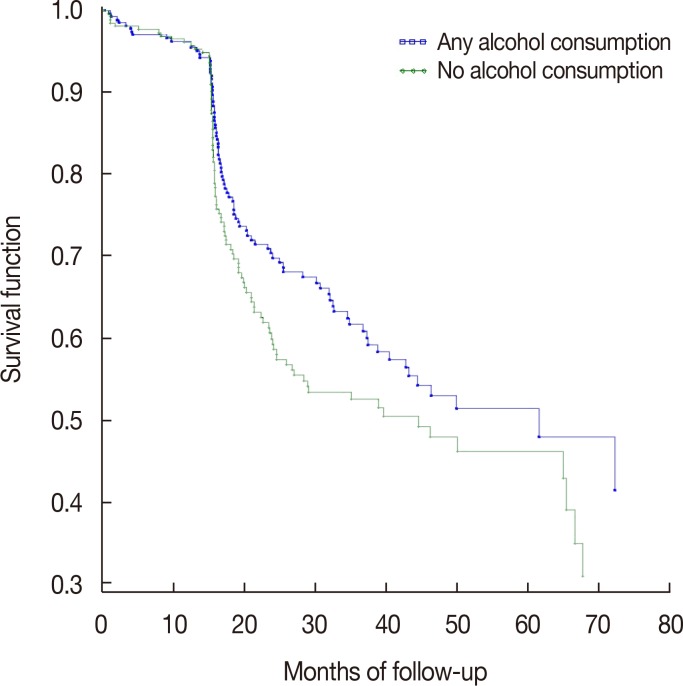
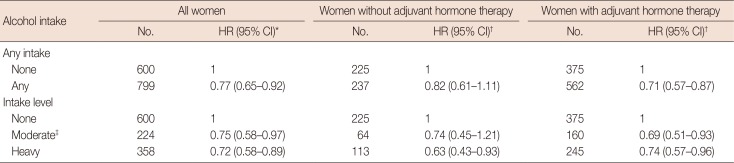
The results for the association between alcohol consumption and the outcome, overall as well as stratified by adjuvant hormone therapy, are presented in Table 3 and Figure 1. Overall, alcohol consumption within the preceding 12 months of diagnosis was associated with better breast cancer-free survival. Compared to nondrinkers, improved survival was observed for moderate consumption (HR, 0.75; 95% CI, 0.58–0.97), heavy consumption (HR, 0.72; 95% CI, 0.58–0.89), and any consumption (HR, 0.77; 95% CI, 0.65–0.92).
Among women without adjuvant hormone therapy, moderate alcohol consumption was not significantly associated with breast cancer-free survival (HR, 0.74, 95% CI, 0.45–1.21), whereas heavy drinking was associated with statistically significantly better survival (HR, 0.63; 95% CI, 0.43–0.93). Drinking any amount of alcohol as compared to none had no significant association with breast cancer-free survival (HR, 0.82; 95% CI, 0.61–1.11).
Among women with adjuvant hormone therapy, both moderate and heavy alcohol consumption were associated with better breast cancer-free survival (HR, 0.69, 95% CI, 0.51–0.93 and HR, 0.74, 95% CI, 0.57–0.96, respectively). Drinking any amount of alcohol as compared to none was associated with better breast cancer-free survival (HR, 0.71; 95% CI, 0.57–0.87). There was no significant interaction between alcohol consumption and adjuvant hormone therapy with either of the exposure modeling approaches (p-interaction > 0.05).
In the secondary analysis among women without immunotherapy or chemotherapy (n=639), breast cancer-free survival appeared to be better in women consuming alcohol though these associations no longer reached statistical significance (any consumption vs. none: HR, 0.86; 95% CI, 0.62–1.21). No significant results were observed in stratified analyses among women without adjuvant hormone therapy (any consumption vs. none: HR, 1.12; 95% CI, 0.62–2.03) or women with adjuvant hormone therapy (HR, 0.78; 95% CI, 0.52–1.17). The study findings remained similar after an additional adjustment for the clinical stage (data not shown).
DISCUSSION
This study examined the interaction between pre-diagnostic alcohol consumption and adjuvant hormone therapy in relation to breast cancer-free survival. Our findings suggest better breast cancer-free survival in women consuming alcohol in the 12 months preceding breast cancer diagnosis regardless of their adjuvant hormone therapy status.
Findings on associations of alcohol consumption with breast cancer-free survival from previous studies have been inconsistent [2021222324]. Kwan et al. [6] reported a 19% increase in the risk of breast cancer recurrence in postmenopausal women consuming three or more drinks per week compared to nondrinkers (HR, 1.19; 95% CI, 1.01–1.40) in a cohort of 9,329 women with invasive breast cancer. Another nested case-control study with 365 women reported an increase in the risk of second primary contralateral breast cancer among women with heavy alcohol consumption (≥7 drinks per week) [25]. In contrast, Reding et al. [7] observed an inverse association between alcohol consumption in the 5-year period prior to diagnosis and breast cancer mortality among 1,286 women diagnosed before age 45, with a 30% risk reduction among drinkers compared to nondrinkers (HR, 0.7; 95% CI, 0.5–0.9). Several other studies found no association between alcohol consumption and breast cancer mortality, breast cancer recurrence, or second primary breast cancer [52026].
Consistent with some of the previous reports, we found improved survival among women consuming alcohol before diagnosis. Results of our secondary analysis, excluding women with chemotherapy or immunotherapy, suggest that our findings were not influenced by the potential masking effect of these two treatments. The mechanism underlying the potential effect of alcohol consumption on survival after breast cancer diagnosis from previous studies is unclear but alcohol has been suggested to decrease breast cancer survival through its effects on estrogen metabolism [27]. Alcohol can induce CYP19 activity causing an increase in estrogen levels [10]. An increase in estrogen levels can result in a change of the hormone environment thus potentially affecting the effectiveness of adjuvant hormone therapy and negatively impacting breast cancer-free survival. On the other hand, alcohol is able to induce enzymes in the P450 cytochrome family that are involved in the metabolism of xenobiotics, including tamoxifen and other adjuvant hormone therapy drugs [12]. Some primary and secondary metabolites of tamoxifen, such as endoxifen and 4-hydroxytamoxifen, have better antiestrogenic effects through a higher affinity for estrogen receptors than tamoxifen [13]. The induction of enzymes in the P450 family by alcohol could accelerate the metabolism of tamoxifen resulting in an increase in concentrations of biologically active metabolites that inhibit the action of estrogen on estrogen receptors potentially leading to better survival [14]. The final net effect of alcohol on breast cancer-free survival would likely depend on the relative contribution of these two potential mechanisms working in opposite directions.
We report, for the first time, on the association between alcohol consumption and breast cancer free-survival by the status of adjuvant hormone therapy. One of the strengths of our study was utilizing the prospective cancer registry data supplemented with information from patient surveys and clinical records. However, our study had a few limitations. Information on alcohol consumption was self-reported. Previous studies have shown a high accuracy in the recall of self-reported alcohol consumption in men and women [282930]; however, misclassification of self-reported alcohol consumption cannot be completely ruled out. In addition to the ICD-9 codes, our study used patients' billing system to determine second primary breast cancer and breast cancer recurrence. Hassett et al. [15] reported a specificity of 99% using billing codes to define breast cancer recurrence. In a cohort of 2,726 women with breast cancer, the sensitivity for using billing codes for the outcome definition was 79% to 81% for either breast cancer recurrence or second primary breast cancer. Even though this method demonstrated high validity in the previous studies, some misclassification of the breast cancer outcomes cannot be ruled out completely. Finally, as we did not have information on the general health status of the women, we were unable to compare the presence of other comorbidities in women with and without alcohol consumption.
In conclusion, our findings suggest better breast cancer-free survival in women consuming alcohol, regardless of their adjuvant hormone therapy status. Future studies are needed to elucidate potential mechanisms underlying the observed associations and to confirm our findings.
 XML Download
XML Download